Knee joint is one of strongest joint in body and allows transmission of body weight to leg. Movement across knee helps in doing daily activities including walking, sitting, and standing.
Due to superior ability to produce high resolution images with exquisite soft tissue contrast, MRI is the modality of choice for evaluation of bone marrow. Increase in interstitial water content and hyperperfusion contributes to bone marrow oedema formation. The bone bruise or bone contusion are commonly used to define an occult bone alteration oedematous haemorrhagic due to trabecular microfractures as a result of a direct blow to the bone, application of compressive forces on contiguous bones with a consequent impact mechanism, and the action of a torsional force, and to stresses by traction on the subchondral bone by insertion of the ligament, tendon or capsular as occurs in traumatic avulsion [1].
In addition to trauma, marrow oedema can be seen in a broad spectrum of entities, including infection, transient osteoporosis of the hip bone marrow, and neoplasm demonstrates relatively hyperintense T2 and hypointense T1 signal, but the clinical history and location of injury typically allows the correct diagnosis to be made [2].
Bone marrow oedema on T2 weighted magnetic resonance (MR) images is recognized as an ill-defined hyperintensity in the bone marrow where standard radiographs showed nonspecific osteopenia or normal findings [3].
On MR images, trabecular contusion has the appearance of bone marrow oedema. Although bone marrow oedema is nonspecific and has a similar appearance in inflammatory and neoplastic disorders, a traumatic cause is usually obvious on the basis of the location of bone marrow oedema and the presence of other trauma related findings. After knee injury, bone marrow oedema is frequently subchondral in location [4].
These lesions also referred to as “bone bruises,” are presumably the result of microfracture of the medullar trabecula [5]. Bone bruise represents as acute, occult microfractures of subchondral trabecular bone with subsequent haemorrhage, oedema and hyperemia. On MRI these injuries appears as ill defined, subchondral, reticulated or stellate region of low signal intensity on T1W and high signal intensity on T2W images [6]. Bone marrow oedema of the knee may cause substantial clinical entities, as they cause acute pain and functional loss in the joint. Bone marrow oedema is responsible for patient symptoms and may lead to early degenerative changes [7]. A thorough understanding of knee injury patterns and their mechanisms may help achieve more accurate assessment of injuries [8].
Presence of contusion may also effect management of knee injuries often requiring prolonged rest even in absence of surgical correctible lesion and establishing diagnosis of bone marrow contusion may obviate further costly work up like arthroscopy. Diagnosis of bone marrow oedema following traumatic event prompt a closer inspection for lesions such as ligamentous and meniscal tears.
The primary aim of the study was to identify imaging pattern in bone marrow oedema and to correlate the pattern of bone marrow oedema retrospectively with type of knee injury from clinical history.
The secondary aims were to study bone marrow oedema patterns in setting of acute knee trauma, to associate the type of knee injury (from clinical history) with bone marrow oedema pattern, to determine the most common oedema pattern and to assess the most common type/mode of injury.
Materials and Methods
A cross-section study was done on all patients reffered to Krishna Hospital, Karad for MRI knee with history of recent (< 6 weeks) knee injury. Study was conducted between May 2014 to September 2015 with sample size of 200 patients, after taking the institutional ethical clearance.
MRI of affected knee joint was done as per imaging protocol and images stored in compact disc. Inclusion criteria were patients with recent knee injuries (<6weeks) and normal plain radiograph with no signs of pathology. Exclusion criteria were history of any infection, surgery or neoplasm of knee joint, patients having any prosthetic heart valve implant, any pacemaker implant, aortic stent graft, cochlear implant or any metallic orthopedic implants, any joint replacement surgery and claustrophobic patients. Informed consent was obtained from the patients in English or regional language.
Patients were scanned using 1.5 Tesla Seimens Avanto (Tim + Dot) with Tx/Rx 15 channel knee coil # Tim. Patient was placed in supine position with knee externally rotated 10-20 degree 21. On 1.5 T, knee joint was examined in Saggital (T1, T2, PD, PDFS), Coronal (T2/ PDFS), Axial (T2, Medic) sequences. Imaging was done using FOV: 160 mm, slice thickness of 3 mm on Saggital images; FOV: 170 mm, slice thickness of 3 mm on coronal images; FOV: 170 mm, slice thickness on 3.5 mm and axial images with interslice gap of 1.5 mm. Matrix in various sequences were listed as : T1 Saggital – 307 x 384, T2 Axial - 314 x 448, T2 Saggital – 314 x 448, PD Saggital – 307 x 384, PD Coronal – 355 x 384, PDFS Saggital – 288 x 384, PDFS Coronal – 311 x 384, MEDIC Axial – 240 x 320. An axial acquisition through the patella femoral joint was used as the initial localizer for subsequent coronal and saggital images. The saggital plane was primarily used to evaluate the bone marrow oedema which was confirmed on coronal images.
Analysis of bone marrow oedema was done by a single observer based on MRI [9], its patterns were studied and possible type/mode of injury was determined before elucidating the history from the patient. Following informed consent, complete history from the patient and relative (attendant) about injury was recorded. The oedema pattern & suspected type/mode of injury on basis of MRI were then correlated with detailed patient’s history on mode of injury. Correlation between type or mode of injury and patterns of bone marrow oedema was determined using p-value and chi-square method.
Results
Out of 200 patients, 32 were women (16%) and 168 men (84%). The patients age ranged from 17-65 years and majority of patients were in 21-30years age group. A 124(62%) had trauma in right knee and 76(38%) in left knee.
In total 200 cases, bone marrow contusion was noted in 138 cases (69%) and absent contusion in 62 cases (31%). In patients with bone marrow contusion, 14 were women (10.1%) and 124 were men (89.9%). Right knee injury was noted in 87 cases (63%) and left knee in 51 cases (37%).
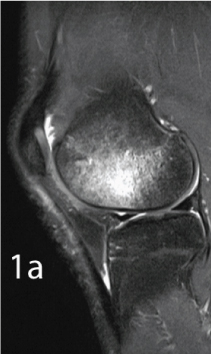
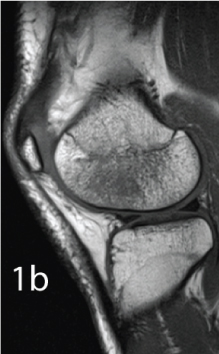
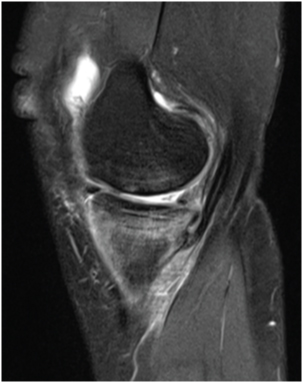
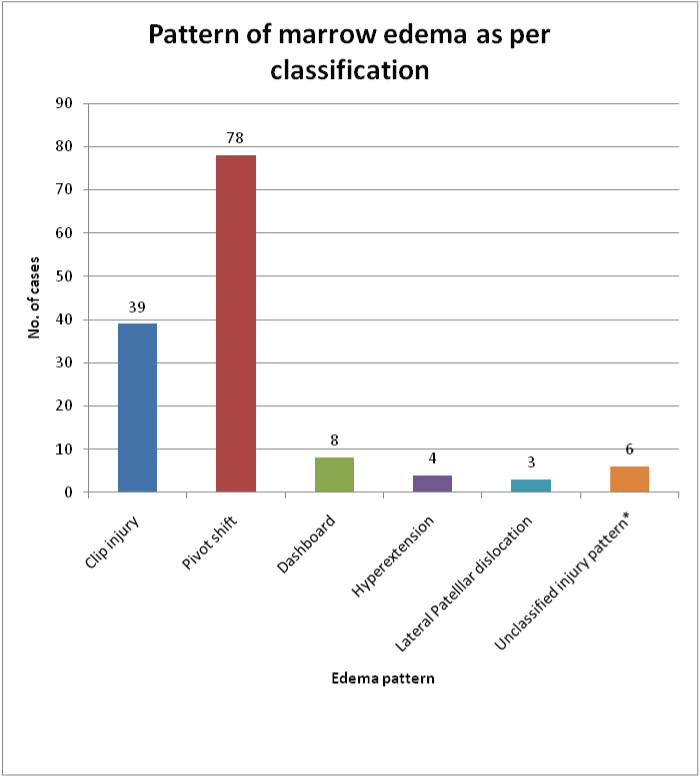
Five patterns of bone marrow contusion was noted in 138 cases: Clip injury in 39 cases (28.3%) [Table/Fig-1a&b], Pivot shift injury in 78 cases (56.5%) [Table/Fig-2a&b], Dashboard injury in eight cases (5.8%) [Table/Fig-3], Hyper extension injury in four cases (2.9%) [Table/Fig-4], Lateral patellar dislocation in three cases (2.2%) [Table/Fig-5]. In six cases (4.3%) no pattern of bone marrow contusion could be explained and was categorized as unclassified pattern [Table/Fig-6].
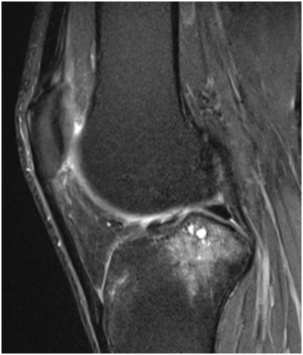
PDFS Saggital: Bone marrow oedema at Lateral femoral condyle in Clip injury pattern.
T1W Saggital: Bone marrow oedema at Lateral femoral condyle in Clip injury pattern.
PDFS Saggital: Bone marrow oedema at Lateral femoral and posterolateral tibial plateau in Pivot shift injury.

PDFS Coronal: Bone marrow contusion at lateral femoral condyle and lateral tibial plateau in Pivot shift injury pattern.

PDFS Saggital: Bone marrow oedema at proximal tibia in Dashboard injury.

PDFS Saggital: Bone marrow oedema at Medial femoral and Medial tibial condyle in Hyperextension injury.
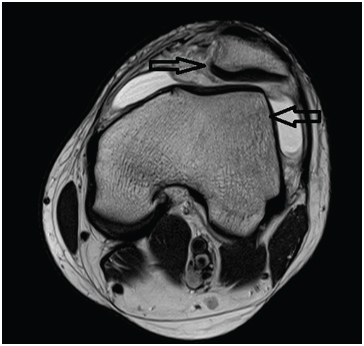
T2 Axial: Bone marrow oedema in Inferiomedial aspect of patella and lateral femoral condyle in lateral patellar dislocation.
Pattern of marrow oedema as per classification.
*no pattern of bone marrow contusion could be explained as per the classification.
Among the clip injury pattern, most common type/ mode of injury was two wheeler accident which was seen in 26 out of 39 cases (66.6%) [Table/Fig-7,8].
Type / Mode of injury in Clip injury pattern.
| Type/ Modeof injury | Lateral femoral | Lateral femoraland medialfemoral condyle | Total |
|---|
| Two wheeleraccident | 12 | 14 | 26 |
| Sports injury | 2 | 6 | 8 |
| Injury whilecrossing road,hit by vehicle | 0 | 2 | 2 |
| Fall while gettingdownstairs | 0 | 2 | 2 |
| Fall from stool | 1 | 0 | 1 |
| Total | 15 | 24 | 39 |
Correlation between contusion pattern in clip injury and type/mode of injury.
| Type/ Modeof injury | Lateral femoral | Lateral femoraland medialfemoral | Total |
|---|
| Two wheeler accident | 12 | 14 | 26 |
| Other causes | 3 | 10 | 13 |
| Total | 15 | 24 | 39 |
Most common location of marrow oedema in pivot shift pattern was posterolateral tibial plateau and lateral femoral condyle and medial tibial condyle and medial femoral condyle in 31 cases (39.7 %) [Table/Fig-9]. Among 46 cases, football was most common sports leading to injury followed by Kabaddi. [Table/Fig-10,11 and 12] show the aetiologies and location for pivot shift injury, Type /Mode of injury among dashboard injury pattern (8 cases) were - Impact from dashboard in 4 cases, fall from bike (2 cases), running downstairs (1 case) and fall while paying cricket (1 case). Location of bone marrow contusion in hyperextension injury (4 cases) was - medial tibial and medial femoral condyle (2 cases) and anterior aspect of proximal tibia and femur (2cases).
Pivot shift injury pattern according to Location of marrow oedema.
| Location of marrow oedema | Number of cases (n= 78) |
|---|
| Posterolateral tibial plateauand lateral femoral condyle | 19 (24.3%) |
| Posterolateral tibial plateauand lateral femoral condyleand medial tibial condyle | 28 (35.9%) |
| Posterolateral tibial plateauand lateral femoral condyleand medial tibial condyleand medial femoral condyle | 31 (39.7%) |
On applying fisher-exact test, p = 0.1655 i.e. No significant difference was noted in location of bone marrow contusion in clip injury for different type/mode of injury.
Table showing Type/Mode of injury in pivot shift injury.
| Type / Mode of injury | No. of cases |
|---|
| Sports injuries | 46 (59%) |
| Two wheeler accident | 15 (19.2%) |
| Hit by car/ motor vehicle | 5 (6.4%) |
| Domestic voilence/ Fighting | 5 (6.4%) |
| Running / jogging | 4 (5.1%) |
| Other cause * | 3 (3.8%) |
| Total | 78 |
*Other cause include fall while getting down from bus (1 case), fall while jumping (1 case), fall while getting downstairs.
Pivot shift injury depending on location and type/mode of injury.
| Type /Modeof injury | PLTand LF | PLT, LFand MT | PFLT, LF,MT and MF | Total |
|---|
| Sports injury | 11 | 14 | 21 | 46 |
| Two wheeleraccident | 3 | 6 | 6 | 15 |
| Hit by car/Motor vehicle | 1 | 2 | 2 | 5 |
| Fighting /Domesticvoilence | 2 | 2 | 1 | 5 |
| Running/Jogging | 2 | 2 | 0 | 4 |
| Other causes | 0 | 2 | 1 | 3 |
| Total | 19 | 28 | 31 | 78 |
PLT: Posterolateral tibial plateau, LF: Lateral femoral condyle, MT: Medial tibial condyle, MF: Medial femoral condyle.
Pivot shift injury in different location and its correlation with sports related injury and other type/mode of injury.
| Type/Mode of injury | PLT, LF | PLT, LT, MT | PLT, LF, MT, MF | Total |
|---|
| Sports injury | 11 | 14 | 21 | 46 |
| Other cause | 8 | 14 | 10 | 32 |
| Total | 19 | 28 | 31 | 78 |
PLT: Posterloateral tibial plateau, LF: Lateral femoral condyle, MT: Medial tibial condyle, MF: Medial femoral condyle.
There were 2 cases with hyperextension injury while playing football and 2 patients attained the injury after being hit by car.
Bone marrow contusion is transient dislocation of patella noted in anterior aspect of lateral femoral condyle and inferiomedial aspect of patella in all the cases (100 %). Type/Mode of injury were twisting injury while getting downstairs (1 case), twisting injury while doing household work (1 case) and injury while playing football (1 case). Most common type / mode of injury in patients with unclassified pattern in fall from bike (3 cases) followed by hit by car/ motor vehicle (2 cases) and injury while lifting heavy weight in 1 case [Table/Fig-13].
Unclassified injury pattern in 6 cases with type /mode of injury and location of bone marrow contusion.
| Type / Mode of injury | Location of contusion |
|---|
| Fall from bike | Medial and lateral tibial condyle |
| Hit by car while crossing road | Lateral tibial plateau and medial femoral condyle |
| Injury while weight lifting | Intercondylar eminence tibia |
| Fall from bike | Intercondylar eminence tibia [Table/Fig-14] |
| Hit by car | Medial femoral condyle, Metadiaphysis femurand lower pole of patella [Table/Fig-15] |
| Fall from bike | Medial femoral condyle, proximal tibia and headof fibula [Table/Fig-16] |
Chi-square = 1.926, p =0.3817 i.e. no significant difference in location for different type/ mode of injury.
PDFS Coronal: Bone marrow oedema at Medial femoral condyle and Metadiaphysis.

PDFS Saggital: Bone marrow oedema in Intercondylar region tibia with subchondral cysts.
PDFS Coronal: Bone marrow oedema at Medial femoral condyle and proximal tibia.

Correlation between various pattern of bone marrow oedema and type/mode of injury are shown in [Table/Fig-17]. Chi-square: 41.961 and p <0.001 suggests that clip injury was significantly high in fall from two wheeler and pivot shift injury was significantly higher in sports related injury.
Correlation between various pattern of bone marrow oedema and type/mode of injury.
| Patterns ofbone marrowoedema | Sportsinjury | Fall fromtwowheelers | Hit bycar/motorvehicle | Fallrunningdownstairs | Other | Total |
|---|
| Clip injury | 8 | 26 | 2 | 2 | 1 | 39 |
| Pivot shift | 46 | 15 | 5 | 1 | 11 | 78 |
| Dashboardinjury | 1 | 2 | 4 | 1 | 0 | 8 |
| Hyperextensioninjury | 2 | 0 | 2 | 0 | 0 | 4 |
| Lateral patellardislocation | 1 | 0 | 0 | 1 | 1 | 3 |
| Unclassifiedpattern | 0 | 3 | 2 | 0 | 1 | 6 |
| Total cases | 58 | 46 | 15 | 5 | 14 | 138 |
Discussion
Conventional radiograph evaluation of skeleton following trauma divides injury into presence or absence of fracture. MRI is used widespread to interpret more complex injuries. Many patients coming with complain of pain following injury without radiographic evidence of fracture, MRI yields presence of extensive injury marrow which is characterised by marrow oedema and haemorrhage termed as bone bruise.
Oedema or interisital fluid within marrow extracellular space similar to free fluid shows long T1 and T2 decay characteristics and appear hypointense on T1 and hyperintense on T2W. Bone marrow oedema may also show delayed enhancement following administration of gadolinium DTPA. Reflecting presence of increased free water oedema, appears hyperintense on inversion recovery and fat suppressed images and shows increase diffusivity on Diffusion weighted images [10].
On MR images, trabecular contusion has the appearance of bone marrow oedema. Although bone marrow oedema is nonspecific and has a similar appearance in inflammatory and neoplastic disorders, a traumatic cause is usually obvious on the basis of the clinical history, location of bone marrow oedema and the presence of other trauma related findings. After knee injury, bone marrow oedema is frequently subchondral in location and may be associated with either trabecular or cortically based lines [4]. Bone marrow bruise is ill defined subchondral reticular or stellate region of low signal intensity on T1 and high signal intensity on T2W images [6].
MR feature of bone bruising reflects increase in water content in marrow cavity as a result of haemorrhage, therefore water sensitive sequence like fat saturated T2W, PD weighted image or STIR are used [1,11,12].
Compression and tension are two basic loads that commonly act on the knee [4]. In compressive load, bones collide leading to impaction. Compressive load causes bone marrow contusion and, if sufficient in magnitude, depressed cortical fracture. It can also damage interposed soft tissues, most commonly the articular cartilage and meniscus. In tensile load, on the other hand, bones pull apart leading to distraction across the joint and traction on stabilizing structures. Tensile load can cause ligament and tendon tears as well as avulsion fracture. In impaction, the compressive force directly strikes cortical bone and is dissipated into trabecular bone [4].
The magnitude of the force is a major determinant of the imaging findings. A load that is too low to cause cortical fracture may be sufficient to disrupt trabecular bone and produce marrow contusion. In distraction injury, excessive tension may damage the joint capsule, retinacula, ligaments, and tendons as well as their osseous attachment sites. The spectrum of damage includes stretching, partial tearing, and complete rupture [4].
Bone marrow contusion usually resolves in 6-8 weeks [6]. Boks et al., conducted a study of the natural course of bone bruises in posttraumatic knees and to describe possible determinants of this course and concluded that Median healing time of bone bruises is 42.1 weeks [5]. Prognosis is particularly influenced by the presence of osteoarthritis. Age, type of bone bruise, and number of bruises also have prognostic value. They found that all the lesions in one patient do not heal at exactly the same speed. Therefore, an influence by the number of bone bruises on healing time was marked; the higher the number, the more likely that there will be one slowly resolving lesion.
In this study, patients with history of knee injury <6 weeks were considered as recent knee injuries. In our study, bone marrow oedema was seen in 138 cases (69%) out of 200 cases. These findings are comparable to Arndt et al., who conducted a study in MR diagnosis of contusion of knee in < 6 weeks and described bone marrow contusion in 23 cases out of 51 cases (45.1%). In this study, inclusion criteria included history of knee injury within 6 weeks or suspected ACL injury [12]. In suspected ACL injury, bone marrow contusion may not be necessarily present.
Kapelov et al., conducted a study to demonstrate that T2 weighted fast spin echo (FSE) images with spectroscopic fat saturation (FS- FSE) increase conspicuity between marrow contusion and normal marrow in post traumatic knee and found bone marrow contusion in 21 out of 76 cases (27.6%) which is less than our study (69%) [11]. In this study, the time gap between injury and doing MRI was not considered. In many cases, Bone marrow contusion might have resolved at time of MRI.
Terzidis et al., 20 conducted a study on acute knee injuries in 255 athletes with acutely injured knees, 219 MRIs were done within the first month after the injury and 36 within two to four months [13]. Bone marrow contusion was noted in 71 cases out of 255 cases (27.8%). In this study, inclusion criteria were acute knee injury only in athletes while in our study there were no such selection criteria. We have included all the patients coming with acute knee injuries irrespective of type/mode of injury.
Sanders classified bone marrow contusions in five different patterns as: Clip injury, Pivot shift injury, Dashboard injury, Hyperextension injury, and Lateral patellar dislocation [8]. The clip injury is a contact injury that occurs after a pure valgus stress is applied to the knee while the knee is in a state of mild flexion (i.e. 10°–30°). Bone marrow oedema is usually most prominent in the lateral femoral condyle secondary to the direct blow, whereas a second smaller area of oedema in the medial femoral condyle secondary to avulsive stress to the MCL. Associated Soft tissue injuries include ACL and medial meniscus [8]. In present study clip injury pattern is noted in 39 cases (28.6%).
Bone marrow contusion was noted in lateral femoral condyle in 15 cases (38.5%) and involving lateral and medial femoral condyle in 24 cases (61.5%). Contusion in medial femoral condyle occurs secondary to the avulsion to medial collateral ligament from site of attachment at medial femoral condyle [8]. Most common type/mode of injury in clip injury pattern in fall from two wheeler in 26 cases (66.7%). Associated MCL injury is noted in 31 cases (79.5%). Other soft tissue injuries include: ACL (100%), PCL (7.6%), Medial meniscus (89.7%), Lateral meniscus (23.1%), LCL (7.6%).
Application of valgus load to the knee in various degree of flexion combined with external rotation of the tibia or internal rotation of the femur lead to pivot shift injury resulting in disruption of Anterior Cruciate Ligament (ACL). Resulting bone contusion pattern will be present in the posterior aspect of the lateral tibial plateau and midportion of the lateral femoral condyle near the condylopatellar sulcus. Bone contusion is also noted in posterior lip of the medial tibial condyle [8] or medial femoral condyle and medial tibial condyle [7]. This pattern is thought to result resolution from contrecoup forces in the medial compartment at the forced valgus forces. This mechanism of injury involves other soft tissue structures like tears/posterior capsule and arcuate ligament, medial collateral ligament (MCL) and the menisci. In our study pivot shift pattern is noted in 78 cases (56.5%).
Bone marrow contusion at posterior lip of medial tibial condyle was seen in 59 cases. Results are comparable to the study conducted by Kaplan et al., in which bone marrow contusion at posterior lip of medial tibial condyle was seen in 25 out of 215 cases (11.6%) and contusion in lateral compartment was noted in 24 out of 25 cases (96%) and contusion at medial femoral condyle was seen in 5 in 25 cases (20%) [7].
Dashboard injury occurs when force is applied to the anterior aspect of the proximal tibia while the knee is in a flexed position. This injury most commonly occurs when the knee strikes against the dashboard during an automobile accident or fall against the ground on flexed knee. Oedema is seen at the anterior aspect of the tibia and, occasionally, at the posterior surface of the patella [8]. Soft tissue injury associated with dash board injury includes PCL and posterior joint capsule. In this study 8 cases (5.7%) had dashboard injury pattern of bone marrow contusion at anterior aspect of proximal tibia. Type/Mode of injury in these cases are: impact during car accident in 4 cases, fall on flexed knee while playing cricket in 1 case, while getting downstairs in 1 case and fall from bike in flexed knee in 2 cases. Injury in PCL is seen in all the cases. Other associated injury in ACL (87.5%), Medial meniscus (50 %) and lateral meniscus (75%).
Hyperextension of the knee can result when direct force is applied to the anterior tibia while the foot is planted or from an indirect force, such as a forceful kicking. Contusion is seen in the anterior aspect of the distal femur and proximal tibia or located in medial femoral and tibial condyle (valgus force applied). Soft tissue abnormalities may include injury of ACL or PCL and a meniscal injury along with injury of the popliteal neurovascular structure, complete disruption of the posterolateral complex, gastrocnemius injury [8].
In this study hyperextension injury noted in 4 cases in 138 cases (2.9%). 2 cases (50%) are hyperextension injury with kissing contusion at anterior aspect of proximal tibia and distal femur caused due to hit by car in RTA. Other 2 cases (50%) are hyperextension with valgus component and kissing contusion at medial aspect of proximal tibia and distal femur caused due to kicking while playing football.
According to study conducted by Terzidis et al., Kissing contusion in acute knee injury is noted in 16 cases out of 225 (7.1%). In these 16 cases, contusion in medial compartment was noted in 2 cases (12.5%) [13].
While the knee is in a state of flexion, twisting motion of the knee can lead to transient dislocation of knee. It typically occurs in teenagers and young adults involved in athletic activities. When femur rotates internally on a fixed tibia on the flexed knee; contraction of the quadriceps occurs, leading to lateral dislocation of the patella out of the trochlear groove [8,14].
The classic bone contusion includes involvement of the antero-lateral aspect of the lateral femoral condyle and the inferomedial aspect of the patella. Bone marrow oedema may also be rarely seen at adductor tubercle of the medial femoral condyle due to avulsion injury of the medial patellofemoral ligament. Associated soft-tissue injuries include the medial retinaculum, the Medial Patellofemoral ligament, and the medial patellotibial ligament [9]. In present study transient dislocation of patella pattern is noted in 3 cases (2.2%).
This was comparable to study conducted by Kirsch et al., in who reported transient lateral patellar dislocation in 2% cases with acute knee injuries and bone marrow contusion is noted in lateral femoral condyle in 81% and contusion in patella in 19% cases [15]. In current study unclassifiable injuries pattern was noted in 6 cases. Traumatic mechanisms are sometimes too complex or poorly understood which cannot be comprehend [4].
Limitations
In 6 cases bone marrow contusion could not be explained by various patterns. Follow up scan could not be done to establish the presumable diagnosis of bone marrow contusion.
Conclusion
Pivot shift pattern is most common contusion pattern and the most common type/mode of injury is sports related injury. On analysing the bone marrow contusion pattern, type/mode can be determined in most of cases. Application of biomechanical approach in MR interpretation helps in effortless assessment of osseous contusion and ligament rupture and mark delicate but significant abnormalities.
On applying fisher-exact test, p = 0.1655 i.e. No significant difference was noted in location of bone marrow contusion in clip injury for different type/mode of injury.
*Other cause include fall while getting down from bus (1 case), fall while jumping (1 case), fall while getting downstairs.
PLT: Posterolateral tibial plateau, LF: Lateral femoral condyle, MT: Medial tibial condyle, MF: Medial femoral condyle.
PLT: Posterloateral tibial plateau, LF: Lateral femoral condyle, MT: Medial tibial condyle, MF: Medial femoral condyle.
Chi-square = 1.926, p =0.3817 i.e. no significant difference in location for different type/ mode of injury.