Headache is most commonly experienced by almost every age group with increased influence on the younger age groups [1]. Severe and frequent headache episodes constitute a significant burden for both the individual and the community [2]. Headaches are one of the most prevalent diagnosis in clinical neurology. Raffaelli and Martins reported that 93% of their total study population exhibited some type of headache amid their lives [3]. The advancement of therapeutic experts needs to think about the non-specific imperative issues and diseases that are prevalent in the society [3]. Dental profession is known to be profoundly requesting and stressful learning experience [4]. Stress is defined as “pressure or worry caused by problems in somebody’s life” [5]. Headache is a matter of recognition, in light of the fact that not all are similarly influenced. Headache is not particular for a particular profession. Anxiety is a worldwide issue as it is accounted for everywhere throughout the world. Other expert fields likewise have scholastic weights however very little is composed about them. Abnormal amounts of headache and delayed anxiety introduction might accelerate burnout; a term that portrays the experience of long haul work related fatigue and decreased interest [5]. Headache is a major and common neurological problem and is a main reason of morbidity and incapacity, absenteeism at work place, disturbed academic performance, and is major cause of psychological illness, mood and behavioral disturbances and interrupted social interaction [6]. Considering the role of dental professionals in improving the community’s health, it negatively affects the productivity and quality of life by affecting job performance, causing a large burden for individual and the society [6, 7]. Limitations might emerge in daily activities and work due to frequent and severe headache with major impact on academic performance and quality of life [7].
In this present situation of augmenting normality of headaches, the present study was aimed to assess the prevalence and characteristics of headache in dental professionals.
Materials and Methods
A cross-sectional survey was conducted among all the dental professionals in Pacific Dental College, Udaipur. The study protocol was approved by the Institutional Review Board. Official permission to conduct the study was obtained from the authorities of the institution and ethical clearance was incurred.
Pretesting of the questionnaire-Mean Content Validity Ratio (CVR) was calculated as 0.87 based on the options expressed by a panel of six academicians. Questionnaire was also administered to a sample of 15 dentists twice on successive days who were interviewed to gain feedback on the overall acceptability of the questionnaire in the terms of length and language clarity.
Cronbach’s coefficient was observed to be 0.78. Face validity was likewise evaluated and it was found that 92% of the members observed the survey to be simple.
Questionnaire: Questionnaire was based on various characteristics of headache. These included onset, duration, frequency and intensity of headache, type and intensity of pain, location of headache, its triggering and relieving factors, prodromal and associated signs and symptoms, and duration of work inability due to headache.
Methodology: In the wake of informing the reason for the study, questionnaire were disseminated to all the dental experts of the Pacific Dental School, Udaipur, who were asked to fill in the written informed consent and were solicited to rate every item from the survey picking the suitable reaction. The data obtained was statistically analyzed using SPSS version 22 and descriptive statistics was used to compare the results obtained.
Results
A ramdom sampling technique was used and a total of 380 structured questionnaires were distributed to the respondents who were present at the time of study and willing to participate in the study. Of all the respondents 86.3% were undergraduate students, 7.6% post graduate students and 6.05% were faculty members, age stratification of the subjects showed that 42.8% respondents were of 17-20 years, 42.6% people of 21-24 years age group, 9.2% were in 25-30 years of age group and less than 6% were more than 30 years of age. There were 65% of females and 35% males in the study. Prevalence of headache in present population was found to be 87.1% and that females in this study were more attacked by headaches than males. As shown in [Table/Fig-1]. On comparison of frequency of headache, describing how often it happens, 42.6% respondents were found to have headache often in a month, 31.2% experienced it weekly, 13.2% had this complaint on daily basis and 12.9% cases did not have this complaint. It was seen that out of the cases those had headache complaints, 62.1% subjects affirmed that they did not experience an increase in frequency of headache, while 25% of them had that increase. A 33.4% people had headaches more often on weekdays [Table/Fig-2].
Demographic details and participants with headaches.
| Category | n (%) | Age Group* | n (%) | Gender | n (%) | With Headachen (%) | Without Headachen (%) |
|---|
| Staff | 23 (6.05) | 17-20 | 163 (42.8) | Male | 133 (35) | 104 (78.1) | 29(21.8) |
| Post Graduate | 29 (7.6) | 21-24 | 162 (42.6) |
| Under Graduate | 328 (86.5) | 25-29 | 35 (9.2) | Female | 247 (65) | 227 (91.9) | 20(8.09) |
| | 30> | 20 (5.26) | Total | 380 (100) | 33 (87.1) | 49(12.89) |
* Age in years
| Questions | Options | n(%) |
|---|
| Frequency of occurrence | a. Day | 50(13.2) |
| b. Week | 119(31.2) |
| c. Month | 162(42.6) |
| Increase in frequency | a. Yes | 95(25) |
| b. No | 236(62.1) |
| More frequent period of occurrence | a. Weekdays | 127(33.4) |
| b. Weekends | 61(16.4) |
| c. Spring | 27(7.1) |
| d. Summer | 76(20) |
| e. Winter | 40(10.5) |
Only 30.3% people had sudden onset of headache, 41.8% people summarized that their headache usually begins in the afternoon, whereas 44.5% people reported that within few minutes, their headache reaches maximal intensity [Table/Fig-3]. Of all the respondents 60.3% people agreed that they usually have headaches bilaterally [Table/Fig-3]. [Table/Fig-4] depicts the duration and intensity of headaches. Majority of respondents i.e. 59.2% people précised that their headache lasts for few minutes after medication. Of all the respondents 48.4% people said that without medication their headache lasted for hours. The results displayed in [Table/Fig-4] also show that 50.5% people believed with medications their headaches are mild whereas, 37.6% said without medication their headaches were moderate.
Onset and location of headaches.
| Questions | Options | n(%) |
|---|
| Headaches typically begin | a. Gradually | 112(29.5) |
| b. Sudden | 115(30.3) |
| c. Varies | 104(27.3) |
| Usually begins in | a. Morning | 63(16.6) |
| b. Afternoon | 159(41.8) |
| c. Evening | 81(21.3) |
| d. Night | 28(7.4) |
| Reach maximal intensity in | a. Few Minutes | 169(44.5) |
| e. Hours | 162(42.6) |
| Location of headaches | a. Left Side | 36(9.5) |
| b. Right Side | 66(17.5) |
| c. Both Side | 229(60.3) |
Duration and intensity of headaches.
| Questions | Options | With Medicationn(%) | Without Medication n(%) |
|---|
| Headaches usually last | a. Few Minutes | 225(59.2) | 122(32.1) |
| b. Hours | 98(25.8) | 184(48.4) |
| c. Days | 8(2.1) | 25(6.5) |
| Intensity of headaches | a. Mild | 192(50.5) | 105(27.6) |
| b. Moderate | 109(28.7) | 143(37.6) |
| c. Severe | 25(6.6) | 73(19.2) |
| d. Incapacitating | 5(12.9) | 10(2.6) |
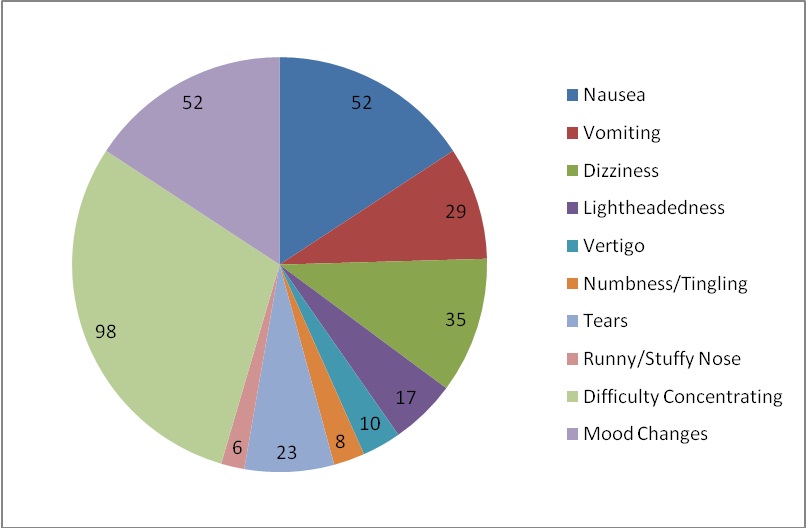
[Table/Fig-5] portrays the interference in activities due to headaches. It is observed that 62.6% respondents felt difficulty in performing their activities due to headaches. However 46.31% people said they have never missed work or college due to headaches. [Table/Fig-6] shows that 23.7% having both throbbing and pressure type of pain, 19.7% experience stabbing headaches, others experience felt tight band like, burning and dull aching pain during headaches. It shows that 32.8% participants had mood changes as the premonitory symptom; while personality changes, changes in appetite, food cravings, neck pain and fatigue are also reported as premonitory symptoms. [Table/Fig-6] also demonstrates the alleviating factors, which include lying down (49.2%), being in a dark and quiet room (7.4%), 3.7% people like to be physically active, 1.3% pace back and forth, 15.8% are relieved by head massage, 7.6% tie something around their head for relief and 2.1% are relieved by fragrance. [Table/Fig-7] shows the trigger factors for headache. Up to 30.5% people think stressful state of affairs triggers their headache; while others consider caffeine, lack of sleep, hunger, menstruation, prolonged computer usage, weather changes and loud sounds, also as trigger factors for their headaches. [Table/Fig-8] figures out the symptoms associated with headaches. Of the all subjects 27.4% experience nausea and mood changes along with their headaches, 7.6% experience vomiting, 9.2% felt dizziness, 4.5% had lightheadedness. Others also experience vertigo, numbness, tears, running nose and difficulty in concentrating while having headaches.
Headache prevented activities and missed days at work.
| Questions | Options | n(%) |
|---|
| Headaches prevent activities | a. School | 238(62.6) |
| b. Work | 40(10.5) |
| c. Household | 53(13.9) |
| Missed days at work/college | a. 1-10days | 129(33.9) |
| b. 11-20days | 26(6.8) |
| c. 21-30days | 10(2.6) |
| d. >30days | 5(1.3) |
| e. None Missed | 176(46.3) |
Pain type, premonitory symptoms and alleviating factors of headaches.
| Questions | Options | n(%) |
|---|
| Headache pain type | a. Pressure | 90(23.7) |
| b. Stabbing | 75(19.7) |
| c. Throbbing | 90(23.7) |
| d. Tight Band | 22(5.8) |
| e. Burning | 5(1.3) |
| f. Dull Ache | 35(9.2) |
| g. Other | 14(3.6) |
| Premonitory Symptoms | a. Mood Changes | 125(32.8) |
| b. Personality Changes | 23(6.1) |
| c. Change in Appetite | 28(7.3) |
| d. Food Cravings | 8(2.1) |
| e. Neck Pain | 12(3.2) |
| f. Fatigue | 29(7.6) |
| g. None | 106(27.8) |
| Alleviating Factors | a. Lying down / Sleeping | 187(49.2) |
| b. Being in a dark quiet room | 28(7.4) |
| c. Keeping physically active | 14(3.7) |
| d. Pacing back-and-forth | 5(1.3) |
| e. Massage your head | 60(15.8) |
| f. Tying something around your head | 29(7.6) |
| g. Fragrance | 8(2.1) |
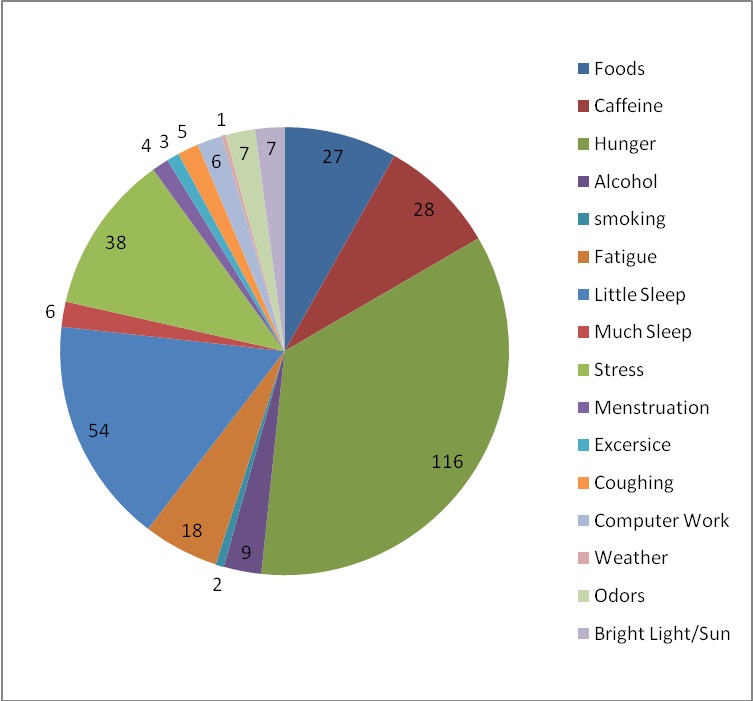
Headache trigger factors.
Headache associated symptoms.
Discussion
Headache is the most common and crucial trouble and an important symptom that bothers neuro-clinicians. Its increasing prevalence and high morbidity has made headache an important general health problem worldwide. It is the main cause which leads to incapacity, stress, diminished job performance, interrupted social interaction and hence deteriorates the productivity and quality of life and one’s personality [3,6–8]. In the current scenario of increasing prevalence of headache and its associated side-effects, several studies have been conducted to determine its characteristics and pattern and the in capacitance caused at workplace [1]. Population-based studies on headache in the general population are numerous [6–11]. However, little is known about its prevalence and characteristics in specific populations, particularly in dental colleges and hospitals, where conflict and instability in student faculty relationship, academic and curriculum stress, patient and clinical responsibilities, personal life issues, financial obligations constitute a major cause of strain, and hence headache [2,5–7]. This study was carried out to assess the distribution of headache and its characteristics in dental students and faculty, and hence create awareness and encouragement for adequate management of headache.
A total of 380 structured questionnaires were distributed to the participants from Pacific Dental College and Hospital, Debari, India. There was 87.1% prevalence of headache in the surveyed volunteers, i.e., they experience at least one headache episode in a year, and 12.9% respondents never had the experience during the year. Numerous past studies have also demonstrated high prevalence of headache ranging from 39% to 96% [3,12–14]. One such study was carried out with Norway students showing that 69.4% of boys and 84.2% of girls had experienced headaches within the past year [15]. Another similar analysis surveyed Brazilian college students which evoked that about 58% of students suffered headache in a year [16]. Juni et al., in their study also found that the prevalence of headache in paramedical students was 82.3% in males and 83.4% in females [17].
Nandha et al., showed pervasiveness of headaches in dental students in North India to be 63.9% which is low when contrasted with our discoveries [1]. Pervasiveness of cerebral pain was additionally examined by Abdo et al., in general population of Yemen which was determined as 76.5% [18]. This was additionally low when contrasted with our findings. The distinction in prevalence might be because of qualification in the meaning of headaches, number of test size, diverse society and the varying age gatherings of the population concentrated on [6,7]. It may also be due to the socio-economic condition in the developing countries especially, for those who have no certain income [7].
It was found that headaches were more often in females than males as was confirmed by earlier studies [1–3,5–7,10–16]. This may be attributed to the effect of female sex hormones specifically estrogen [6].
In the present work, 42.6% cases had monthly headache, 31.3% on weekly basis and 13.2% on daily basis. This is in near accordance with other studies. Vilela Braga PC et al., and Curry K et al., performed a questionnaire based survey in undergraduate students, showed that approximately 50% of students reported headache monthly and 17% students indicated headache episodes one or more times per week [19, 20].
This study found that 25% of respondents had increase frequency of headache episodes. This was similar to the findings of a study carried out in medical students of Andhra Pradesh, Menon B et al., which also reflected an increase in headache frequency in approximately 33% of its participants [21].
This study also demonstrated that in 30.3% of participants, headache begins suddenly and, 41.8% people summarized that their headache usually begins in afternoon. This was also confirmed by Deleu et al., while interviewing medical students in Oman [14] and in concordance with Vilela Braga PC et al., [19]. This study also affirmed that in approximately 60% respondents, headache lasted for few minutes only after self-medication and 48.4% people asserted that without medication their headache lasted for hours; i.e., self-medication relieves the headache. This was also proved by Nandha et al., Sweileh et al. and Abdo et al., [1,2,18].
Of all the respondents 62.6% of our interviewees affirmed that they experience interference with their social and academic activities due to headache episodes and is the main cause of absenteeism at work. Our observation data was higher in value but was in agreement with Ferri-de-Barros JE et al., who also suggested that 44% of their participants had interference with their activities [3]. Nandha et al., surveyed dental students and also concluded routine activity impairment in 81.25% of their subjects [1]. Silva Jr et al., in their study on Brazilian population also reported that 57% of their subjects had interference and reduced work efficiency [16]. Juni et al., findings were also in partial accordance with ours and suggest that their paramedical subjects had difficulties in performing activities due to headache which results in absenteeism at work [17]. Vilela Braga PC et al., surveyed undergraduate nursing students and found that 35.7% students had large impairment in subject activity and concentration ability and 22% had moderate impairment this was in agreement with present data [19].
Our findings indicate that 60.3% had bilateral headaches, in contrast to the results derived by Nandha et al., in dental students and Sweileh et al., in University undergraduate population in Palestine who suggested that headache in their interest of population was unilaterally localized [1,2]. This study revealed that 23.7% cases have both throbbing and pressure type of pain. This was in partial concordance with Vilela Braga PC et al., whose 74.3% participants had throbbing headache [19].
Up to 30.5% people think stressful state of affairs triggers their headache; while some respondents consider lack of sleep, hunger, menstruation, prolonged computer usage, weather changes and loud sounds, also as trigger factors for their headaches. This was in accordance with various studies in past such as that of Nandha et al., Sweilleh et al., Vilela Braga PC et al., and Hashel et al. They also considered stress, sleep deprivation and hunger as common trigger factors for headaches [1,2,18,22].
Mood change is the only symptom experienced before headache as confirmed by 32.8%, but 25.8% respondents reported that they mainly had difficulty in concentrating and about 13.7% said they experienced nausea and mood change secondarily; similar to as reported by Sweileh et al., [2].
This study thus, in accordance with studies in past, is suggestive that headache is most common and disturbing neurological disorder among students and faculties. Hence it is mandatory to create adequate awareness regarding common trigger factors precipitating headache, its effects on routine activities and satisfactory management skills to handle the calamity.
This study has both strengths and weaknesses. The population sample studied was adequate and the data were collected by making the questionnaire filled personally, and relied exclusively on information provided by the respondents about their headache which itself is a subjective and non-measurable complaint.
Limitation
Limitations of the study include the smaller sample size. Population studied was restricted to one single dental college. There is lack of etiological diagnosis of headache. Also it should include additional screening questions that focus on whether the student has had a headache assessment performed by a medical provider and what specific diagnostic studies, if any, the student has received in the past.
Conclusion
Considering the limitations and strengths of the study it can be concluded that headache if most prevalent worrisome neurological malady which impairs routine activities and leads to absenteeism; and hence negatively affects the quality of life and personality. Thus it is essential to counsel people about its impacts and techniques of management.
* Age in years