Tiger Food for Short Bowel: Two Cases
Aswini Kumar Pujahari1
1 Professor, Department of Surgery (Surgical Gastroenterologist), Vydehi Medical College, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aswini Kumar Pujahari, Department of Surgery, Vydehi Medical college, Bangalore-560066, Karnataka, India.
E-mail: akpuja@rediffmail.com
Bianchi’s procedure, Hydrochlorhydria, Thrombosis
Dear Sir,
Short Bowel Syndrome (SBS) refers to a critical reduction in the length of the intestine, leading to chronic diarrhoea, dehydration, malnutrition, weight loss and growth failure [1]. SBS is clinically evident when the total available length of small bowel is <200 cm and commonly caused by resection [2]. The nonsurgical options for management of SBS are: (a) total parenteral nutrition (TPN), which is costly, invasive and un-physiological; (b) para-sympathomimetics drugs, which cause dilatation of the bowel; (c) proton pump inhibitors and others. TPN in addition can lead to thrombosis of canulated vessel, bowel atrophy and sepsis. The surgical options are described to slow intestinal transit, taper dilated bowel segments in children in proximal to atretic segment and intestinal lengthening procedures such as serial transverse entero-plasty (STEP) and Bianchi’s procedure [3]. The third option is small bowel transplant.
The standard dietary management of SBS with colon is 50-60% of caloric intake with complex carbohydrate, 20-30% with fat and 20-30% with protein. Complex carbohydrate in small bowel will cause diarrhoea as these will take long time and has to cover more distance to break down and undergo absorption. These reach colon and work as osmotic agent causing diarrhoea and hence simple sugars (mono/diasacharides) are used as these get absorbed in stomach and in available proximal small bowel. Diet rich in fat and protein cause delay in gastric emptying, higher gastric acid and bile and pancreatic juice secretion. Whereas, protein part get broken down and get absorbed in proximal jejunum and fat in the terminal ileum. The presence of Ileo Caecal valve (ICV) delays the discharge of fat rich fluid and bile acid.
Living beings are divided into carnivorous (Flesh eating), herbivorous (plant eating) and omnivorous (eat flesh and plant). The herbivorous has got the longest small bowel, the carnivorous the shortest and omnivorous remain in the middle. Loss of a part of small bowel in human makes the bowel equivalent to carnivorous, where carnivorous diet (tiger food) is appropriate is the novel thinking.
Case 1
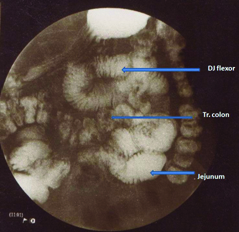
A 49-year-old male underwent bowel resection in three stages due to mesenteric vascular occlusion, leaving behind approximately 15 cm of proximal jejunum and 5-7 cm of terminal ileum with intact ileo-caecal valve and whole colon [Table/Fig-1]. He had an anastomotic leak, for which, he needed TPN for 6 weeks. After closure of the enterocutaneous fistula, he was given oral low residual diet. But he developed diarrhoea for which he was supplemented intermittent intravenous fluid. PPI and isabgole husk was added for reduction of gastric acid and bile diarrhoea respectively. His weight reduced to 48 Kg from 88 Kg over a period of 8 weeks. Thereafter, he was advised tiger food. His main diet was non-vegetarian (10-20 eggs, 2-2.5 Kg Chicken and meat daily). He had additional non residual diet in the form of glucose/sucrose, fruit juice (fructose) rice soup (kanji) totaling 100-150 gram approximately of carbohydrate daily. He was advised boiled water to avoid water borne infective diarrhoea, which is common in India and told to eat any other things he liked. With the modified diet, he stopped losing weight and in two months time he started gaining weight. Over the years he maintained his weight at 56-58 Kg during the 9 years follow up. The haematological and biochemical parameters were normal. He passed 2-4 motions per day and was fit for duty as a truck driver.
Case 2
A 52-year-old male had mesenteric vascular occlusion and all small bowels except 15-20 cm of proximal jejunum and 2-3 cm of terminal ileum was gangrenous. A jejuno-ileal stapler anastomosis going till the Ileo- Caecal valve (ICV) was done. He had an anastomotic leak [Table/Fig-2], but it healed up with parenteral and enteral nutrition. He has been surviving for the last 4 years with the same diet given to the first patient. Being a rice eater, he could not stay without eating rice and was having diarrhoea while on rice diet, after which he used to go back to the prescribed tiger food. He used to maintain his weight but gets pedal oedema periodically due to low albumin when he went to rice based diet.
Barium meal radiograph marking the anastomotic region (DJ- Duodeno-Jejunal flexor).

Barium meal radiograph showing the short length of bowel.
Discussion
Herbivorous small intestine is 10 to 12 times the length of their trunk and in carnivores three to six times. The total length of small bowel is 12 to 22 feet spanning from pylorus to the ceacum in human. All the available enzymes system makes the human an omnivorous [4]. The carnivorous like tiger, lion are likely to have an intestinal length of 3-7 feet. It is established in physiology that, protein digestion is simpler than complex carbohydrate. It starts in the stomach with acid and pepsin and in the duodenum by the pancreatic proteases. Absorption of amino acids is rapid in the duodenum and proximal jejunum [5]. In fact in most of the SMA occlusion proximal 15-20 cm of jejunum escapes gangrene due to the collateral between superior and inferior gastro-duodenal artery of coeliac and SMA circulation respectively. Presence of proximal jejunum helps in absorption of amino acids and ICV makes it more favorable fat absorption by delaying the emptying to large intestine. After a bowel resection in human, the length of small intestine equalizes to that of carnivorous animal. In such a scenario, there is hyper-hydrochlorhydria and rapid transit of intestinal content leading to diarrhoea [6] Tiger food will delay the gastric emptying, acid and pepsin helps in digestion of meat and avoid duodenal ulceration, broken down protein into amino acids get absorbed in proximal jejunum and very little left over to have diarrhoea. Possibly high protein diet helps in quicker adaptation. Other content of the meat sugar (glycogen), fat and vitamins in the meat and chicken, makes the diet complete.
The normal need of protein is one Gram/Kg /day. In normal physiological balanced diet, protein is not included in calculating the calorific requirement, as it is used for the protein synthesis. While in SBS it is not only for the protein synthesis but for calorific value too, because protein and simple sugars absorption are only predictable. In addition glycogenic amino acids add to the genesis of OAA and duplicate the TCA cycle and hence the requirement of high dose protein. It possibly gives higher endurance and strength like tiger and lion as in the first case.
Also, in any diet minimum 35% of calorie should come from carbohydrate. With this aim the simple sugars are given upto 100-150 gm. The meat with muscle glycogen will add to the rest. If the need is 2000 cal. 150X4= 600 cal., that is 30% and 5-10% is left for the meat glycogen.
Thus, it can be concluded that tiger food is appropriate for SBS patients with proximal jejunum and patent ICV.
[1]. Valdovinos D, Cadena J, Montijo E, Zárate F, Cazares M, Toro E, Cervantes R, Ramírez Mayans J, [Short bowel syndrome in children: a diagnosis and management update]Rev Gastroenterol Mex 2012 77:130-40.PMID:22921210] [Google Scholar]
[2]. Wilmore DW, Robinson MK, Short bowel syndromeWorld J Surg 2000 24:1486-92.PMID:11193712 [Google Scholar]
[3]. King B, Carlson G, Khalil BA, Morabito A, Intestinal bowel lengthening in children with short bowel syndrome: systematic review of the Bianchi and STEP proceduresWorld J Surg 2013 37(3):694-704.doi: 10.1007/s00268-012-1879-3. PMID:23232820 [Google Scholar]
[4]. Seth J. Karp, David I, Soyabel chapter small intestine in George D Zuldema & Charles J Yeo(Edrts) Shakelford’s Syrgery of Alimentary tract 2002 (5th edition)WB Saunders Company [Google Scholar]
[5]. Section V. Gastrointestinal Function 25. Digestion & Absorption review of medical physiology 21st edition (2003) Lange publication Willium F Ganong [Google Scholar]
[6]. Hyman PE, Everett SL, Harada T, Gastric acid hypersecretion in short bowel syndrome in infants: association with extent of resection and enteral feedingJ Pediatr Gastroenterol Nutr 1986 5:191-97. [Google Scholar]