The childbirth experience is a process during women’s life and the most important consequence of labour [1]. The separation of woman from the family is a factor to increase the feelings of isolation and stress in the mother. During labour the increased anxiety level in mother enhances the pain perception, increases the labour duration and secretion of catecholamine which reduces the blood flow in the uterus. This decreases the effectiveness of uterine contractions and increases the labour duration [2,3]. Labour duration is one of the effective factors on the pregnancy consequences and maternal and neonatal complications. Due to prolongation of the labour there is risk of fetal or neonatal death, choking, infection and neural and physical damages in the infant. In addition, the mother is at risk of postpartum haemorrhage and infection and psychological distress due to the anxiety, lack of sleep and fatigue [4–6].
Massage is an ancient method that women had received relaxation through it for thousands of years but in modern labour rooms no accurate evaluation has been conducted [7]. Massage is an old technique that is widely used in childbirth [8] and can decrease the childbirth pain by reducing the adrenaline and noradrenaline secretion and increasing the endorphins and oxytocin release thus reducing the childbirth duration by increasing the uterine contractions [9–12]. In earlier studies on the effect of massage on labour duration, inconsistent results have been reported [13–15]. The complications caused by prolonged labour in mother and fetus are enormous and the massage for shortening of duration of labour is simple, affordable, safe and more acceptable for pregnant women.
There are inconsistent results about the effectiveness of massage therapy to decrease labour duration. The aim of the present study was to investigate the effect of massage therapy provided by the trained midwifery students on labour duration.
Materials and Methods
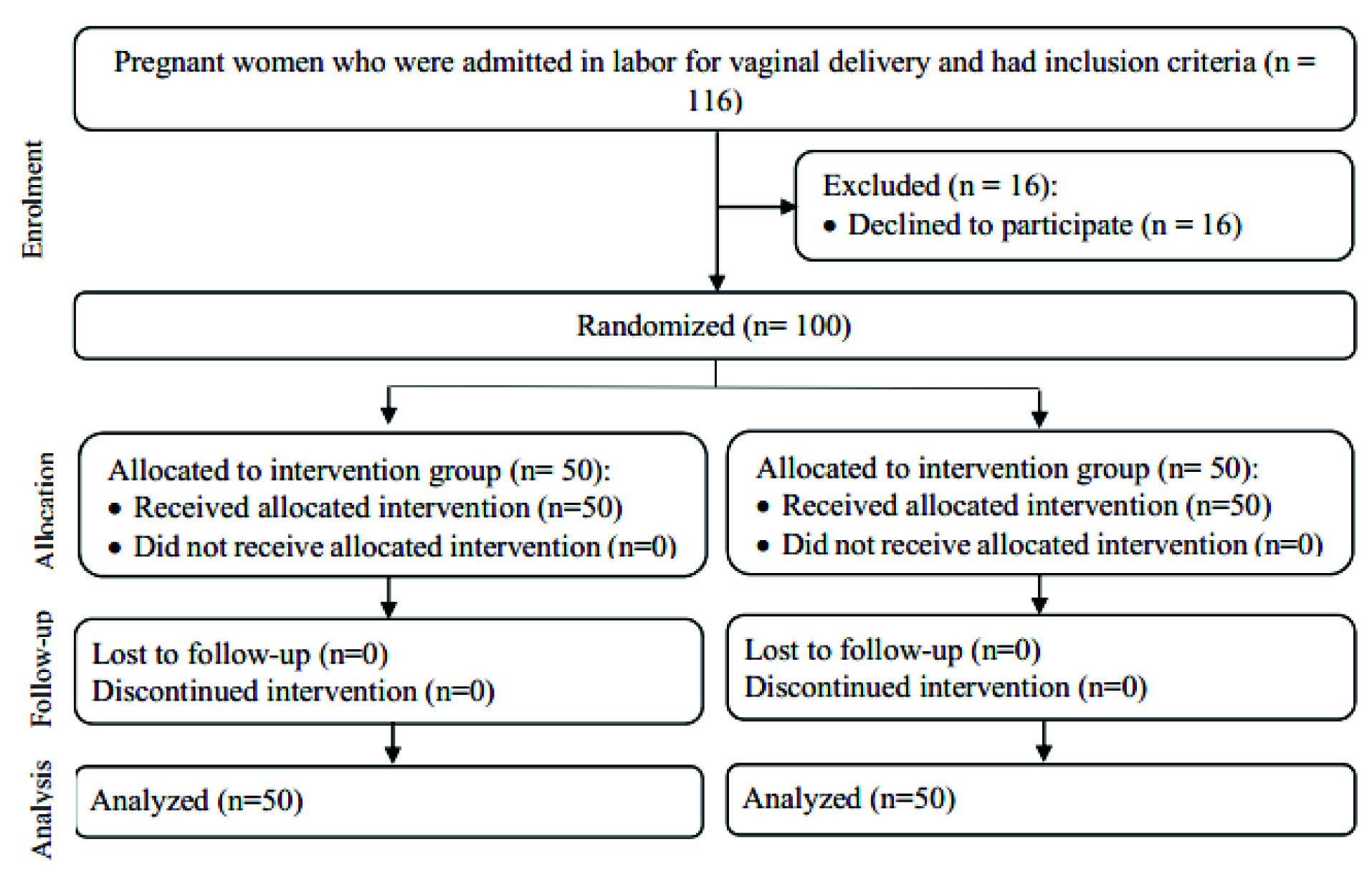
This randomized controlled clinical trial was conducted from October 2013 to June 2015 in Fatemieh Hospital, Shahroud. Sample size was calculated based on criteria for a medium effect size that was employed in a previous similar study [16]. The primary outcome was the length of labour, and the study was powered so that a meaningful difference in length of labour (at least 30 minutes) could be observed if such a difference actually existed. To achieve power = 80 and level of significance = 0.05, 50 women were needed for each group. First adequate explanations about study were given to the pregnant women and written introduction letter was received from them. The number of 100 pregnant women (50 per group) aged 18-45 years with the singleton live fetus and reactive NST were selected at the time of admission. The exclusion criteria were development of any adverse medical disease, psychological depression, pregnancy complications such as preeclampsia, placental abruption and placenta previa, any possibility of fetal anomaly and the record of previous surgery on the uterus.
Pregnant women who fulfilled inclusion criteria were randomly located in the test and control groups. Before the study, the allocation sequence was determined by one of the members of the research team not involved in the samples selection using a randomized blocking and table of the computer random numbers and the participants were located randomly and with a ratio of 1:1 in the intervention and control groups. The codes related to each participant were located in opaque envelopes for hiding the allocation. Thus, the subjects were in A and B groups according to the specified sequence [Table/Fig-1]. Before the study, 40 midwifery students were randomly divided into two groups. The first group students received the necessary instructions about massage techniques and also drawing partogram (20 students) and the second group students was only instructed to draw partogram (20 students). Finally, the sequence of students in both groups was prepared randomly to be present beside the parturient in the specified order.
Flow diagram of the participants.
Data collection tool was a four-section check list that included demographic and obstetric characteristics, the evaluation form, first and second stage of childbirth, infant information and partogram forms. To determine the content validity, the questionnaire was given to ten members of the Shahroud Faculty of Nursing and Midwifery academic staff and their opinions were applied. Test-retest was used in order to determine the stability and correlation coefficient of 0.92 was obtained.
Pregnant women in the intervention group received massage of under belly, upper thighs, sacral region, shoulders and legs for at least 30 minutes and the control group women only received routine care. The partogram diagram was drawn for both groups and duration of labour first and second stage was determined. Finally, infant information was completed after the delivery. During the labour, one of the midwife personnel in the shift was monitoring the labour process and the childbirth was performed by the person not involved in the parturient control process.
Because the type of delivery was obvious, therefore, it was not possible to blind the parturient and the service provider but the data analyser was not aware of the interventions provided to the groups.
Statistical Analysis
Data were analysed using SPSS-21. For normalized examination of data, the Kolmogorov-Smirnov test was used. To describe the personal characteristics of the participants, the descriptive statistics (number, percentage, mean and standard deviation) was used. To compare the studied variables in both groups, the chi-square test, Fisher’s-exact test, independent t-test and Mann-Whitney test were used. Also, for controlling the possible intervening factors on the test results, the multivariate linear regression was used. In the data analysis, p<0.05 was considered significant. This research project was approved by the Ethics Committee of Research Deputy of Shahroud University and has been registered in IRCT system with ID: IRCT2013111815443N1.
Results
Some of the demographic and obstetric characteristics of participants in research have been shown in two separate groups in [Table/Fig-2]. As observed, the participants in the study were homogeneous in terms of all studied variables, except for age and instruction. The average age of participants in test group was significantly higher than the control group (p= 0.001). Also, the number of people with high school diploma and upper education in test group was significantly higher than the control group (p <0.0001).
Demographic and obstetric characteristics of participants.
| massage group*n= 50 | Control group*n= 50 | Total*n= 100 | p-Value |
|---|
| Mother age, year | 25.84 ± 5.22 | 23.42 ± 4.51 | 24.63 ± 5.02 | 0.001† |
| BMI | 25.56 ± 5.00 | 25.07 ± 3.91 | 25.31± 4.48 | 0.44† |
| Occupation | | | | 0.38** |
| Housewife | 43 (86) | 45 (90) | 88 (88) | |
| Employed | 7 (14) | 5 (10) | 12 (12) | |
| Education | | | | <0.0001** |
| < Diploma | 16 (32) | 36 (72) | 52 (52) | |
| ≥ Diploma | 34 (68) | 14 (28) | 48 (48) | |
| Gestational age, week | 39.15 ± 1.01 | 39.42 ± 1.02 | 39.28 ± 1.02 | 0.21‡ |
| Parity | 0.66 ± 0.94 | 0.65 ± 0.90 | 0.65 ± 0.92 | 0.82‡ |
| Cervical dilation at admission time, cm | 2.73 ± 1.43 | 2.56 ± 0.74 | 2.64 ± 1.14 | 0.96‡ |
* Mean ± SD, number (percent), † independent T-test, ‡ Mann-Whitney test, ** chi-square test.
According to the information shown in [Table/Fig-3], duration of labour first stage and also the duration of labour second stage in test group was significantly shorter than the control group (p <0.0001 and p = 0.003) and massage was able to decrease the duration of labour first and second stage. Comparison of Apgar score in the first and fifth minutes in test and control groups showed that the subjects in test group obtained better Apgar scores compared to the control group and the result was statistically significant (p<0.0001). Delivery by Caesarean section due to abnormal events, such as decrease in fetal heart rate or dystocia, in the massage therapy group was lower than the control group. Although the difference was not statistically significant.
Comparing the groups in terms of labour and delivery outcomes.
| massage group*n= 50 | Control group*n= 50 | Statistic | p-Value |
|---|
| Duration of first stage of labour (from admission time to 10 cm cervical dilatation), hours | 8.96 ± 5.31 | 11.46 ± 3.71 | t= 3.86 | <0.0001† |
| Duration of second stage of labour, minute | 49.29 ± 27.86 | 64.14 ± 34.67 | z= -2.97 | 0.003‡ |
| The need for oxytocin | | | χ2= 1.22 | 0.26 ** |
| Yes | 11 (22) | 8 (16) | | |
| No | 39 (78) | 42 (84) | | |
| Type of delivery | | | χ2= 2.90 | 0.17†† |
| Normal vaginal delivery | 49 (98) | 47 (94) | | |
| Cesarean section / vacuum | 1 (2) | 3 (6) | | |
| Apgar score in the first minute | 8.55 ±0.74 | 7.82 ± 0.93 | z= -5.88 | <0.0001‡ |
| Apgar score in the fifth minute | 9.36 ± 0.71 | 8.92 ± 0.90 | z= -3.50 | <0.0001‡ |
* Mean ± SD, number (percent), † independent T-test, ‡ Mann-Whitney test, **
chi-square test, ††Fisher’s exact test
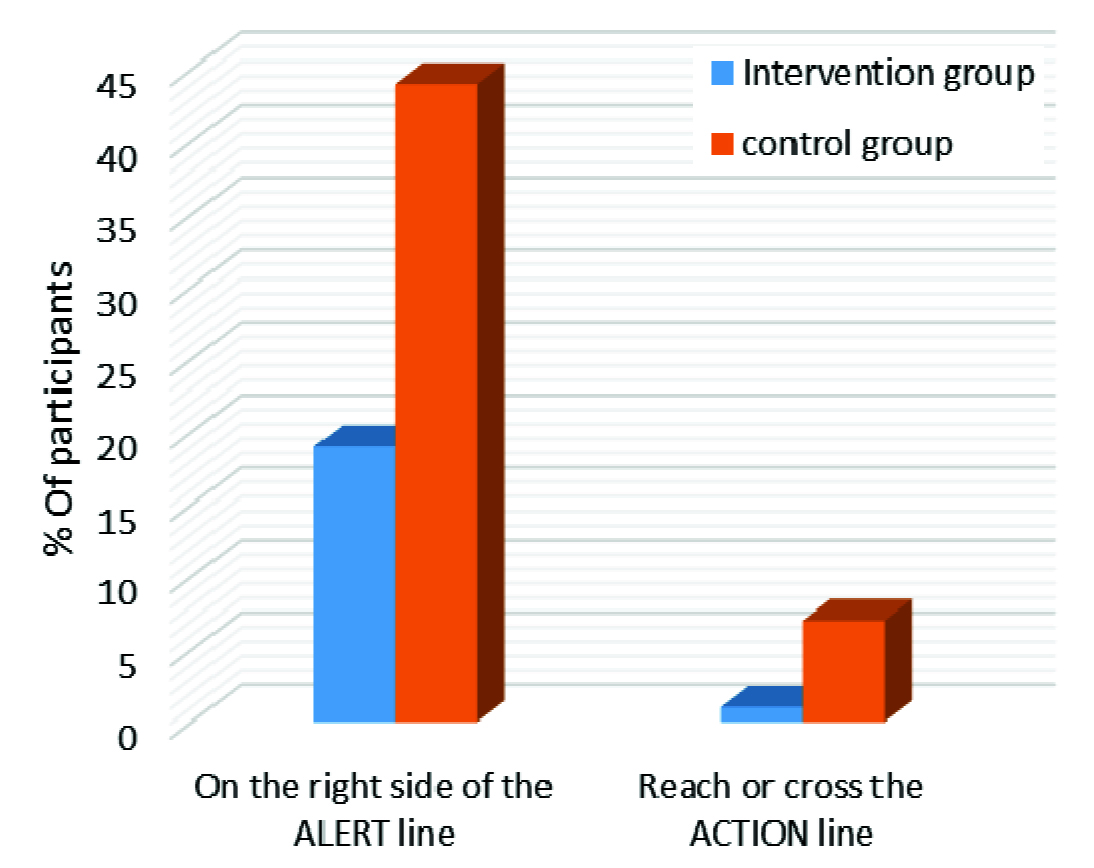
Evaluation of effect of massage on labour progress using the chi-square test showed that 19% of test group subjects have passed the alert line in labour process in the partogram against 44% of control group subjects and the difference was significant (p<0.0001). On the other hand, in evaluation of partogram diagram with Fisher’s-exact test, only 1% of test group and 7% of subjects in control group reached the action line but the difference was not significant (p = 0.06) [Table/Fig-4].
Comparison of partogram curve in the two groups.
Due to the non-homogeneity of study groups in terms of some studied variables and possible effect of intervening factors on the test result, the multivariate linear regression was used. The results showed that by controlling other variables, the massage decreased the duration of labour during first stage (OR = -0.21 and p = 0.004) and second stage (OR = -0.17and p = 0.02) significantly [Table/Fig-5].
Predictive factors of duration of the first and second stages of labour (multivariate linear regression).
| Duration of the first stage of labour (hours) | Duration of the second stage of labour (minute) |
|---|
| Factors | B | OR* | p | B | OR* | p |
|---|
| Group |
| Control group | | 1 | | | 1 | |
| Massage group | -2.02 | -0.21 | 0.004 | -10.98 | -0.17 | 0.02 |
| Mother age, year | -0.02 | -0.02 | 0.80 | -0.86 | -0.13 | -0.12 |
| BMI | 0.13 | 0.13 | 0.055 | 0.19 | 0.02 | 0.69 |
| Education |
| < Diploma | | 1 | | | 1 | |
| ≥ Diploma | -0.46 | -0.04 | 0.54 | -3.20 | -0.05 | 0.54 |
| Gestational age, week | 0.66 | 0.14 | 0.03 | -0.62 | -0.02 | 0.76 |
| Parity | -0.72 | -0.14 | 0.08 | -9.48 | -0.27 | 0.001 |
| Cervical dilation at admission time, cm | -0.98 | -0.23 | 0.001 | -0.02 | -0.001 | 0.99 |
| Baby gender |
| Girl | | 1 | | | 1 | |
| Boy | -0.60 | -0.06 | 0.33 | 2.47 | 0.03 | 0.56 |
| Birth weight, g | 5.99 | 0.03 | 0.55 | -0.001 | -0.07 | 0.26 |
| Constant | -14.39 | 112.30 |
*Odds Ratio
Discussion
The results showed that supporting the parturient in labour with massage therapy decreased the duration of labour first and second stage significantly. The results of other studies in this area have been consistent with our results. Abbasi et al., have found that average duration of labour first and second stage in massage receivers was significantly lower than the subjects of control group [13]. Field et al., in their study on the effect of massage on pain and childbirth duration have found that massage lead to reduction of pain and childbirth duration [14]. In contrast, Chang et al., in a study about the effect of massage on pain and anxiety during childbirth have reported no significant difference during childbirth in massage therapy and control groups. Even a slight increase was reported in the first stage of labour in massage therapy group [15]. The reason for this contradiction might be due to the fact that only women with first pregnancy were chosen for investigation but in the present study there was no limitation in terms of number of deliveries. Also, in this study the massage techniques were performed by the trained midwifery students while in Chang’s study the massage techniques were performed by the husband. Field stated the effects of massage by doula (supporter) are higher than the husband and the reason is unknown [14].
Other findings of this study were improving Apgar scores at minutes 1 and 5 in massage therapy group compared to control group. In study by Keshavarz et al., and Khavandi Zadeh et al., the supportive treatment had increased the first minute Apgar significantly [17,18]. Considering the shortening of labour in first and second stages, it is reasonable that Apgar scores in the massage therapy group were significantly higher than the control group. In fact, the effect of supportive person in labour decreases the utilization of analgesics, epidural anaesthesia, infant low Apgar score and childbirth with cesarean and instruments [19].
Another highlight of the present study was the use of partogram in evaluation of labour progress. Students in both test and control groups were trained how to use partogram before the study. Findings showed that the number of people whose partogram diagram has passed the alert line was significantly lower in the test group than the control group which represents the fact that normal labour process in the massage therapy group subjects was higher than another group subjects. In addition, 7% of subjects in control group had prolonged labour (partogram curve passed the action line) and this amount was 1% for the supportive group, although the difference was not significant. Kamali Fard et al., showed in their study that partogram curve in 2.5% of subjects in the control group who do not receive massage therapy during labour (compared to 0% of the test group) has passed the action line [20]. The results show that massage during labour can decrease the labour duration and shorten the childbirth process.
In relation to the type of childbirth, the results show no significant difference between two study groups. In support of this finding, American College of Obstetricians and Gynecologists also have found that active management of childbirth may decrease the labour duration but cannot reduce the cesarean rates in all cases [4]. The lack of significant difference in terms of childbirth type in two study groups can be due to the use of partogram and preventive measures. Sizer et al., have suggested in their study that increased childbirth interventions such as cesarean can be due to the use of partogram. The reason for this increase could be due to the stricter monitoring of labour, faster decision-making and preventive measures in order to decrease the labour duration [21].
Considering the duration of the first and second stages of labour is reduced with massage therapy, we recommend that further studies are conducted in order to find the other effects of massage therapy in delivery and this method can be used for enhancing normal vaginal delivery. One of the limitations of current study is the small sample size. Thus, studies with larger sample size are recommended.
Conclusion
The findings of this study showed that massage therapy during labour led to shortening of labour first stage duration, improvement of labour progress and Apgar scores at first and fifth minutes and as a noninvasive, safe, accessible and low cost method can decrease the complications related to the prolonged labour and at the end promote the normal childbirth.
* Mean ± SD, number (percent), † independent T-test, ‡ Mann-Whitney test, ** chi-square test.
* Mean ± SD, number (percent), † independent T-test, ‡ Mann-Whitney test, **
chi-square test, ††Fisher’s exact test
*Odds Ratio