Introduction
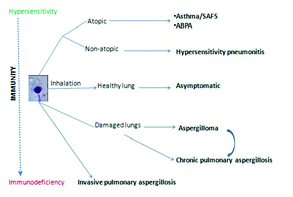
The genus Aspergillus comprises of hundreds of fungal species ubiquitously present in nature; predominantly in the soil and decaying vegetation. Nearly, 60 species of Aspergillus are medically significant, owing to their ability to cause infections in human beings affecting multiple organ systems, chiefly the lungs, paranasal sinuses, central nervous system, ears and skin. Aspergillus fumigatus is the most common variety affecting human beings. The spectrum of the disease caused is highly variable and varies from asymptomatic colonization to fulminant life threatening event depending upon the immune status of the host and the virulence of the agent [1]. [Table/Fig-1] summarizes the spectrum of clinical disorders that can be attributed to Aspergillus.
Schematic diagram showing spectrum of pulmonary aspergillosis with respect to host immune status.
The increasing incidence of chronic lung disorders with impaired airway clearance like Chronic Obstructive Pulmonary Diseases (COPD), asthma, pulmonary fibrosis, etc. and advances in other frontiers of medicine like solid organ/bone marrow/stem cell transplant and newer immunosuppressive therapies are leading to an increase in incidence of fungal disorders [2]. Early non-invasive diagnosis becomes crucial to initiate timely life saving therapies, given the invasive nature of the fungus and the mortality associated with it. The Computed Tomogram (CT) offers a quick non-invasive clue and plays a crucial role, especially in invasive aspergillosis as most of these patients are critical where a tissue diagnosis would be difficult to obtain and fungal cultures may be time consuming and unpredictable. This article aims to review the various radiological patterns, the differential diagnosis and the diagnostic pitfalls one encounters and also addresses the crucial issue as to when to order for the CT.
The spectrum of disease that results from the Aspergilla becoming a resident in the lung is known as ‘Pulmonary Aspergillosis’. An inert colonization of pulmonary cavities like in cases of tuberculosis and Sarcoidosis, where cavity formation is quite common, makes it aspergilloma or fungal ball. Hypersensitive response to fungal antigens manifests as allergic bronchopulmonary aspergillosis in an atopic individual and hypersensitivity pneumonitis in a non-atopic person. These all being non invasive forms of the disease. Nevertheless, these fungi have the propensity to breach tissue barriers. Tissue invasion in the form of angioinvasive variety or air way invasion, both seen commonly in patients with systemic and/or local immunosuppression represents the most severe variety of the spectrum known as Invasive Aspergillosis. A less severe, more insidious locally invasive form seen in lesser degree of immunocompromise known as semi-invasive or chronic pulmonary aspergillosis. The radiological spectrum is also different in each variety and the pattern correlates closely with the underlying immune derangement [3].
Pattern recognition remains the key in any radiological diagnosis and the knowledge as to how these patterns correlate with the underlying immune derangement would provide a useful framework to understand this complex spectrum of illness.
Invasive aspergillosis: It can be angioinvasive or airway invasive form. Traditional teaching is that Invasive Pulmonary Aspergillosis (IPA) is always seen in immunosuppressed and neutropenic patients, like those infected with the Human Immunodeficiency Virus (HIV), patients undergoing cancer chemotherapy, bone marrow or any other solid organ transplant, suffering from hematogenous malignancies, or consuming high doses of steroids. However, it is important to keep in mind that less commonly, invasive aspergillosis can also be seen in patients with less severe form of immunocompromise, such as patients with obstructive lung disease and interstitial fibrosis [4]. Rarely invasive aspergillosis may develop in patients with normal immune status following massive inhalation of spores, a condition known as primary invasive aspergillosis [1,5]. IPA manifests within 10-14 days of the trigger of immunosuppression (point of most profound neutropenia), which is a very crucial clue [5]. In these patients, fungal hyphae invade the pulmonary vessels leading to thrombosis, pulmonary infarction and haemorrhage. In such cases the chest radiographic findings like patchy airspace opacities, areas of consolidation and vague nodular infiltrates are quite nonspecific and can be found in various other pulmonary conditions [6]. Thus in an immunocompromised patient presenting with symptoms suggestive of chest diseases, CT should not be delayed. CT provides more clear and timely diagnosis or can at least provide more logical differentials. Signs on CT scans constituting clinical evidence for invasive pulmonary disease by the 2008 criteria proposed by the EORTC/MSG include dense, well-circumscribed lesion(s) with or without a surrounding “halo” of ground-glass gray attenuation, air-crescent sign, and cavity formation [7]. [Table/Fig-2] depicts the case of a patient with invasive aspergillosis showing the above mentioned features. A paper published by Greene et al., found that patients with invasive aspergillosis most commonly presented with one or more micronodules in 94% while halo sign was present in 61%. Other features at presentation were consolidation in 30%, infarct shaped nodules in 27%, cavitary lesion in 20% and air crescent sign in 10% patients [8].
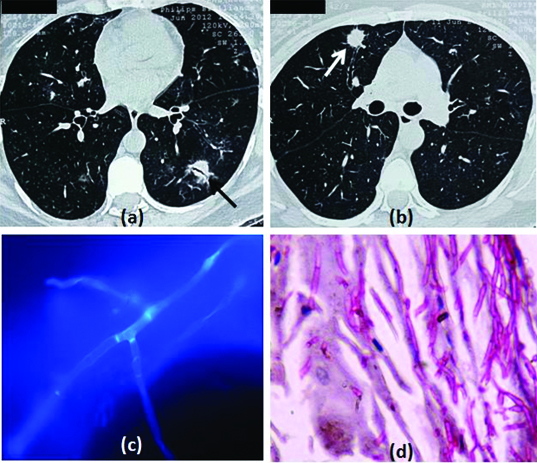
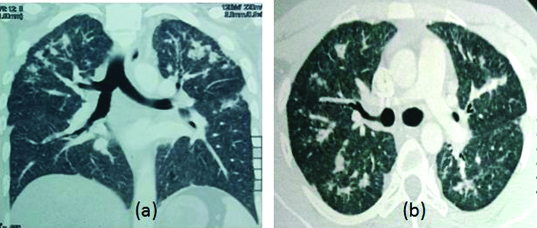
CECT thorax of a 42-year-old asthmatic female on chronic steroid therapy showing: (a) Left lower lobe nodule with air-bronchogram surrounded by the halo sign and centrilobular nodules (black arrow), (b) One nodule (while arrow) in the right upper lobe associated with an ectatic bronchus and another smaller nodule adjacent to the wall of the bronchus; Hyphae of A. fumigatus obtained through a bronchoalveolar lavage of the same patient seen in (c) Calcofluor white stain; and (d) PAS stain showing acute angled branching, hyaline, septate hyphae.
Signs and patterns that are seen in invasive aspergillosis are discussed below:
Halo sign: The halo represents pulmonary haemorrhage, coagulative necrosis surrounding the central necrotic nodule containing Aspergillus hyphae. Such lesions progressively coalesce with confluent consolidation. But this sign is transient and is seen only in the first 10 days of angioinvasion after which it disappears, thus it signifies the need of early CT scan in appropriate clinical settings [8]. However, a note of caution is required in interpreting halo sign. The halo represents the surrounding pulmonary haemorrhage and so it can be seen in any condition which causes such insult like any other infection, Bronchioloitis Obliterans with Organizing Pneumonia (BOOP), granulomatosis with polyangiitis, metastatic angiosarcoma and focal lung injury. [Table/Fig-3] demonstrates the chronological development of the halo sign and air crescent sign.
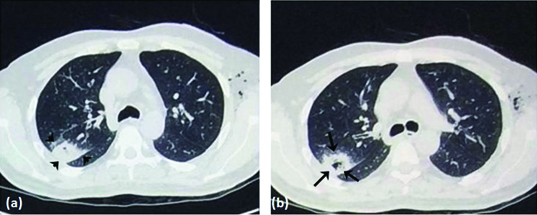
Angioinvasive aspergillosis in a 35-year-old male patient who underwent bone marrow transplant whose sputum examination demonstrated actively multiplying colonies of Aspergillus fumigatus Serum was also positive for galactomannan. CT thorax done (a) at presentation showing patchy consolidation with surrounding ground glass opacity (Halo sign, depicted by arrowheads) in right lower lobe and (b) after 14 days showing breakdown with air-crescent formation (arrows) within the consolidation.
Air crescent sign: It is seen in 50% cases [1,6] usually after two weeks of disease onset i.e. when the patient’s immune response recovers. Air crescent represents the nodular opacity with retracted infracted lung with crescentric and circular cavitations and can be appreciated on chest radiographs in some cases as a crescent-shaped/circumferential area of radiolucency within a parenchymal consolidation or nodular opacity. It is a non-specific sign and can be seen in a number of conditions like bacterial pneumonias, cavitating neoplasms or metastasis, focal lung injury, interstitial lung diseases like BOOP and immunological disorders like granulomatosis with polyangiitis. However, when considered along with the appropriate clinical settings, it is very characteristic and has a prognostic significance as well because it suggests improvement in the immune response of the host and thus spells greater survival rate [1,6]. Needless to mention that the time at which to pick up IA in CT is that of the early appearing halo sign and not the air crescent sign which appears 2 weeks later.
Hypodense sign: It is appreciated in mediastinal window settings in CT. It is a precursor of air crescent sign and appears as relative hypodensity within the nodular lesion. It is less sensitive sign but highly specific sign for fungal infection [9]. [Table/Fig-4] depicts respectively the X-ray and CT of patients with IA showing the air-crescent sign in the right upper lobe and the development of the hypodensity that precedes the former.
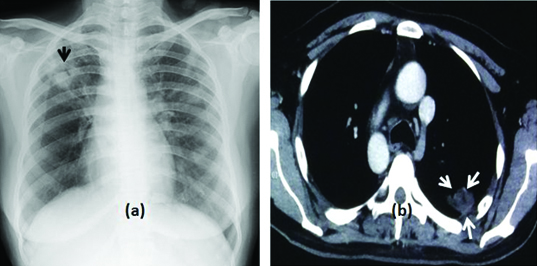
(a) Plain radiograph posteroanterior view chest of a 56-year-old female patient on cancer chemotherapy showing consolidation-cavitation with air crescent in right upper lobe suggestive of fungal ball with possibly invasion. (b) CT thorax of another 29-year-old male patient with angioinvasive aspergillosis who underwent a renal transplant showing a nodular lesion in left lung with central hypodensity (arrows). The “Hypodense sign” preceding the formation of air crescent is a less sensitive but highly specific sign for fungal infection.
Another variety of invasive aspergillosis is the relatively rare, airway invasive form which has been reported in approximately seven percent of all the cases of pulmonary aspergillosis [10]. It can present as an acute upper or lower respiratory tract infection like trancheobronchitis or bronchioloitis and bronchopneumonia. The fungal hyphaes owing to their property of tissue invasion invade the airway basement membranes and can present as intraluminal pseudo membranes of dead and necrotic tissue, fibrin strands and tangled fungal hyphaes leading to severe airway obstruction. Alternatively, the fungi may cause nodular plaque like thickening of the tracheal and bronchial walls and can even lead to broncho-esophageal and broncho-arterial fistulae, conditions having dire consequences. Plain chest radiographs may reveal non specific airspace nodules or patchy consolidation in such cases. CT in such cases [Table/Fig-5] may demonstrate thickened nodular tracheal and bronchial wall with multiple centrilobular nodules and areas showing these centrilobular nodules arranged in “V” and “Y” shaped branching patterns known as the ‘tree-in bud’ pattern on the High Resolution Computed Tomography (HRCT). Tree in bud can be seen in numerous infective as well as non infective conditions and specifically represents endobronchial spread. It is commonly seen in infections like tuberculosis, fungal and bacterial infections, aspiration pneumonitis and many more. However in patients of immunosuppression specific importance should be given to such findings on CT and possibility of fungal infection must be considered. Rarely patchy peribronchial consolidations are seen in cases of bronchopneumonia [11,12].
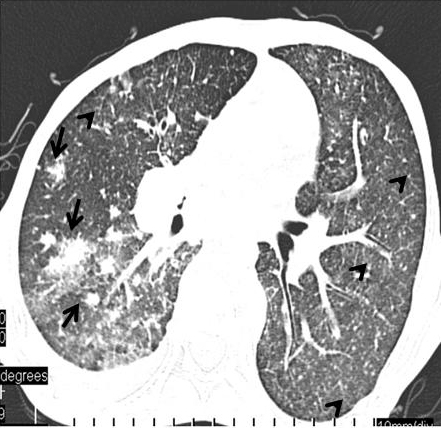
Fungal bronchopneumonia of the airway, invasive variety in a 38 years old patient with AIDS. CT thorax demonstrates multifocal areas of nodular consolidation and surrounding ground glass opacities (arrows). Diffuse centrilobular nodules with branching linear and nodular areas (arrowheads) distributed throughout the lungs.
In nutshell, in such serious patients when a tissue diagnosis is rather difficult to achieve in many cases and sputum cultures take significantly long time and may even be unreliable, imaging findings become crucial in diagnosis. CT definitely enjoys an upper hand in early detection than chest radiographs and plays a crucial role for critical decision making and rapid onset of treatment and follow up of such patients.
1. Chronic Pulmonary Aspergillosis: Known by a host of fancy names such as pulmonary aspergillosis with cavitation, Aspergillus pseudo tuberculosis, complex aspergilloma etc., Chronic Pulmonary Aspergillosis (CPA) is a more localized and relatively less severe form of pulmonary aspergillosis than the invasive varieties. It is more often seen in people with mild immunosuppression such as in diabetes mellitus, malnutrition, alcoholism prolonged systemic steroid therapy, HIV infection and in the setting of pre-existing lung damage as seen in preexisting tubercular or sarcoid cavities, emphysematous bullae etc., [13–15]. In such cases a localized form of tissue invasion is caused by fungus and ultimately there is tissue breakdown and cavity formation. The process is relatively slower than the invasive counterparts. Three forms of patterns are recognized under the gamut of CPA namely, Chronic Cavitating Pulmonary Aspergillosis (CCPA), Chronic Necrotizing Pulmonary Aspergillosis (CNPA) and Chronic Fibrosing Pulmonary Aspergillosis (CFPA). It is imperative to note, that the aforementioned clinical entities offer not just a varied radiological spectrum but also differ from each other in terms of the clinical presentation, histopathology and clinical outcome. On one hand, CCPA is characterized by multiple, usually upper-lobe predominant cavities with enlarging radii, with or without a fungal ball [Table/Fig-6a&b] while CNPA represents a mildly invasive aspergillosis of the parenchyma characterized by cavitating nodules, consolidation with breakdown, peri-lesional infiltrates and occasionally even the much-haloed air-crescent sign and is thus also called semi-invasive pulmonary aspergillosis [Table/Fig-6c]. On the other hand, CFPA characterized by areas of consolidation, cavitation, parenchymal fibrosis, traction bronchiectasis and pleural fibrosis probably represents a burnt-out form of the disease [Table/Fig-6d]. In general, CPA has a predilection for upper lobes of lungs and appears on CT as lobar consolidation with breakdown areas as well as calcifications and cavity formation which are difficult to distinguish from tuberculosis, actinomycosis and histoplasmosis. It is also not uncommon to have an unyielding histopathology in this disorder. The diagnosis of CPA is therefore complex and relies on a clinic-radio-mycoserological approach.
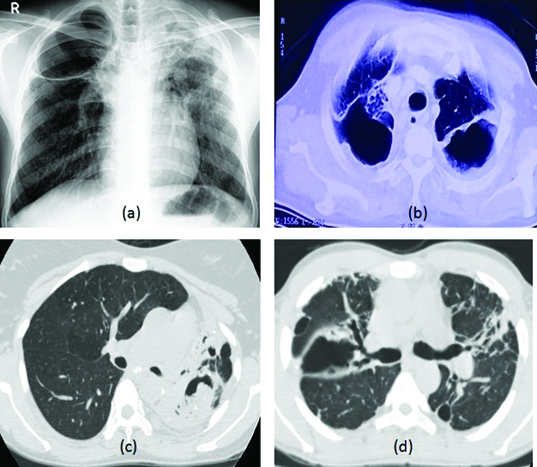
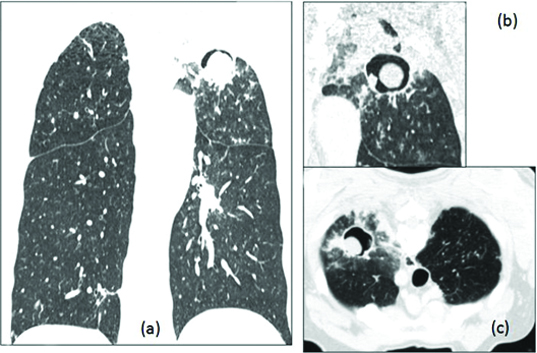
(a,b) Chronic cavitating pulmonary aspergillosis in a 28-year-old alcoholic patient with past history of tuberculosis now presenting with low grade fever and cough for more than 2 months. The bronchial washings showed Aspergillus and the serum immunoglobulin IgG antibodies to Aspergillus fumigate was positive. CT chest shows consolidation with breakdown and cavity formation in bilateral upper lobes. Few calcific foci are also noted within; (c) HRCT thorax of a 52-year-old diabetic female showing left upper lobe cavitating consolidation with a fungal ball. She fulfilled the criteria for CPA and was diagnosed with chronic necrotizing pulmonary aspergillosis; (d) HRCT thorax of a 43-year-old diabetic male showing bilateral cavitation, fibrosis and traction bronchiectasis suggestive of chronic fibrosing pulmonary aspergillosis.
Allergic Bronchopulmonary Aspergillosis (ABPA): It is an allergic response or hypersensitivity to the antigens of inhaled spores and germinating hyphaes of the Aspergilli manifesting in the lungs of an atopic individual. Opposed to what is seen in the previously discussed forms of aspergillosis, ABPA is a disorder of an ‘over competent’ immune system that results in bronchiectasis and other associated changes in the lungs. A 1-2.5% of patients who suffer from chronic asthma have underlying ABPA [3]. Although, sporadic cases have been reported wherein ABPA has developed on the background of COPD, aspergilloma etc, bronchial asthma remains the soil on which ABPA would develop [16]. Clinical clues to the diagnosis include asthma that is ‘not controlled anymore’ and expectoration of golden-brown mucus plugs. The main challenge posed by ABPA is to differentiate between patients of steroid responsive asthma and ABPA [3]. Chest radiographs may be normal or show transient and fleeting airspace opacities. Major findings on CT include central cystic or varicose bronchiectasis with mucoid impaction of the dilated bronchi giving thick branching parahilar densities also known as gloved finger appearance. Presence of high attenuating mucus plug within the dilated bronchi is very specific finding on CT and signifies more severe ABPA & associated with an increased recurrence rate [17]. Three main imaging features are identified to help differentiate between asthma and ABPA. Bronchiectasis is present in 95% patients with ABPA while it is seen in less than 30% diagnosed with asthma. Another differentiating feature is mucoid impaction that is seen in 67% patients with ABPA but in 4% of asthmatics. Centrilobular nodules representing small airway obstruction is reported to be seen in 93% patients of ABPA, while it is reported in 28% asthmatics in a study [18]. [Table/Fig-7,8] demonstrate the radiological manifestations of ABPA such as central bronchiectasis and mucus impaction. A similar clinico-radiological picture can be incited by a host of other non-Aspergillus fungi, a syndrome called allergic bronchopulmonary mycosis (ABPM) and in the presence of suggestive findings where Aspergillus-specific work-up is negative; these fungi should be investigated for [19].
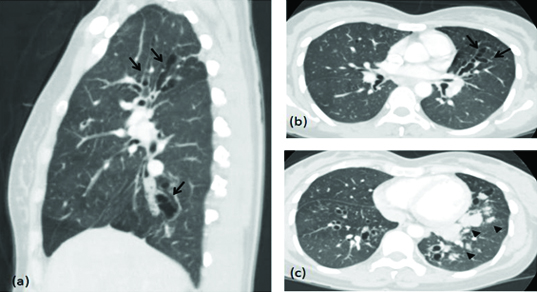
CT thorax of a 40-year-old asthmatic female: (a) Sagittal; and (b) axial images show central varicose bronchiectasis (arrows). ABPA was diagnosed through the Greenberger-Patterson criteria and she had achieved remission after steroid therapy was initiated; (c) CT thorax of the same patient done 2 years later when she returned with recurring symptoms shows dilated, mucus-filled dilated bronchi (gloved finger appearance; represented by arerows).
Chest Radiograph Posteroanterior view of another patient with ABPA (allergic bronchopulmonary aspergillosis) shows V shaped tubular opacities in the right parahilar location (arrowheads).

2. Aspergilloma or fungal ball: It is an indolent colonization of preexisting cavities like in cases of old tuberculosis, sarcoidosis etc. Other conditions may include bronchogenic cyst, pulmonary sequestrations & pneumatocoeles secondary to Pneumocystis jiroveci infection in patients with AIDS [1,20]. Such patients usually have normal immune status and there is no tissue invasion. Patients may be asymptomatic or may have mild cough and haemoptysis. Chest radiograph shows round oval mass, the fungal ball partially occupying the pre existing cavity producing the air crescent. This air crescent has to be differentiated from the air crescent seen in invasive aspergillosis. CT demonstrates cavity with fungal ball within it which changes its position and becomes dependent on prone scan. Fungal ball has entangled fungal hyphaes mixed with air and minerals giving it high attenuation on CT. Fungal strands bridging the fungal ball and the cavity wall is quite specific of aspergilloma [1,3]. Differentials for a fungal ball is blood clot in pre existing cavity, necrotic carcinoma, lung abscess with necrosis and a hydatid cyst. Hallmark of simple aspergilloma is that there is no radiological change of appearance over a long period of time. Occasionally, such long standing indolent looking cavities with fungal ball within, begin to enlarge with surrounding consolidation and may show new cavitations and breakdown areas and associated pleural thickening, particularly when host immunity is lowered due to certain predisposing factors. It would be associated with constitutional symptoms [1,3,21] Such complicated aspergilloma needs to be differentiated from the simple variety because of its aggressive nature which may even lead to severe haemoptysis owing to vascular invasion which may require urgent bronchial artery embolization. CT again plays a significant role in differentiating the simple aspergilloma with the complex one. CT also differentiates aspergilloma from other conditions like Wegner’s granulomatosis and cavitating lung carcinoma. In a cavitating carcinoma, the cavity is thick walled and is not pre existing. The mass would be non mobile. No fungal strands/air filled mycelial network would be there and no paracystic lung opacities [20,21] Thus imaging helps in avoiding such diagnostic pitfalls and also in follow up of such patients. [Table/Fig-9] demonstrates the impact of gravity on a simple intra-cavitary aspergilloma.
Fungal ball: Cavitary tuberculosis with fungal ball (aspergilloma): 32-year-old male patient presented with cough and chest pain (a) Coronal HRCT scan (b) Magnified view of the lesion (c) Prone scan reveals an area of consolidation with cavitations involving left apical region with a well defined nodular opacity with air crescent within the cavity. Prone scan shows the nodular opacity is mobile and settled in the dependent position.
3. Hypersensitivity pneumonitis: Hypersensitivity Pneumonitis (HP) is a spectrum of interstitial, alveolar, and bronchiolar lung diseases resulting from immunologically mediated inflammation in response to a wide variety of inhaled organic or low-molecular-weight chemical antigens (or haptens), which may lead to irreversible lung damage, usually in a non-atopic individual. Among the aspergilli, Aspergillusfumigatus and A. clavatus are the most commonly implicated in the causation of HP [22]. Clinically, HP manifests in three, albeit ill-defined, forms namely acute, sub-acute and chronic, implying therefore that the disorder has a varied presentation. While the former two manifest shortly after antigen inhalation, presenting with fever, cough, dyspnoea, myalgia amd hypoxaemia, the latter is more indolent in its presentation with gradual onset of cough, dyspnoea, and fatigue and weight loss. The radiology of HP differs according to the manifestation of the illness.
Acute HP is seen on the chest radiograph as a lower zone predominant disease with non-specific findings such as diffuse, poorly-defined nodular radiodensities, with areas of ground glass radiodensities or occasionally even consolidation. The HRCT is better at delineating these findings wherein one can appreciate relative upper-lobe sparing and a more peripheral distribution of the nodules. Frequently, these findings normalize after cessation of antigen exposure and resolution of the illness [22,23]. Similarly, sub-acute HP is seen radiologically as reticulonodular appearance with fine linear shadows and small nodules while the HRCT of the thorax demonstrates centrilobular nodules associated with larger areas of ground-glass opacity, as well as air trapping and mosaic perfusion [Table/Fig-10] [24]. On the other hand, chronic HP is seen as an upper to mid-zone predominant disease which manifests as linear densities representative of fibrosis and fluffy shadows representing active disease on the X-ray. HRCT findings include intralobular and interlobular septal thickening, traction bronchiectasis, emphysema and honeycombing [25]. Therefore, it is likely to mistake HP in its chronic form for Idiopathic Pulmonary Fibrosis (IPF) or Non-Specific Interstitial Pneumonia (NSIP). Although mediastinal lymphadenopathy is unusual in HP, the presence of the same would likely prompt a diagnosis of sarcoidosis. Imaging features that favour HP over IPF and idiopathic NSIP include an upper or mid zone predominance, extensive ground-glassing, centrilobular nodules, and conspicuous air trapping [26,27]. Therefore, the diagnosis of HP should be made after careful consideration of the clinical, radiological and immunological characteristics of the patient.
HRCT thorax of a 24-year-old farmer with chronic hypersensitivity pneumonitis due to A. fumigatus. (a) coronal section showing upper lobe predominance of the disease in the form of (b) parenchymal fibrosis, interlobular and intralobular interstitial thickening and centrilobular nodules.
Conclusion
Aspergillosis though caused by a ubiquitous fungus which almost everyone inhales, but in the susceptible, it can take a nasty turn. The type of pulmonary aspergillosis that a patient will develop depends on his immune status and existing lung disease. Radiology especially CT plays a crucial role in recognizing and managing this potential serious condition and for follow-up. The various distinctive imaging patterns in the spectrum of pulmonary aspergillosis especially in relevant clinical settings, providing an early diagnosis can be life saving and result in better patient care.
[1]. Gefter WB, The spectrum of pulmonary aspergillosisJ Thorac Imaging 1992 7:56-74. [Google Scholar]
[2]. Brown MJ, Miller RR, Müller NL, Acute lung disease in the immunocompromised host: CT and pathologic findingsRadiology 1994 190:247-54. [Google Scholar]
[3]. Greene R, The radiological spectrum of pulmonary aspergillosisMed Mycol 2005 43S:5147-54. [Google Scholar]
[4]. Bulpa P, Dive A, Sibille Y, Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary diseaseEur Respir J 2007 30:782-800. [Google Scholar]
[5]. Thompson BH, Stanford W, Galvin JR, Kurihara Y, Varied radiological appearances of pulmonary aspergillosisRadiographics 1995 15:1273-84. [Google Scholar]
[6]. Gotway MB, Dawn SK, Caolli EM, Reddy GP, Araoz PA, Webb WR, The radiological spectrum of pulmonary Aspergillus infectionsJ Comput Assist Tomogr: JCAT 2002 26(2):159-173. [Google Scholar]
[7]. De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group; National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus GroupClin Infect Dis 2008 46(12):1813-21. [Google Scholar]
[8]. Greene RE, Schlamm HT, Oestmann JW, Stark P, Durand C, Lortholary O, Imaging findings in acute invasive pulmonary aspergillosis: clinical signifi cance of the halo signClin Infect Dis 2007 44(3):373-79. [Google Scholar]
[9]. Horger M, Einsele H, Schumacher U, Wehrman M, Hebart H, Invasive pulmonary aspergillosis: Frequency and meaning of the hypodense sign” on enhanced CTBr J Radiol 2005 78:697-703. [Google Scholar]
[10]. Drury AE, Allan RA, Underhill H, Ball S, Joseph AE, Calcification in invasive tracheal aspergillosis demonstrated on ultrasound: a new findingBr J Radiol 2001 74(886):955-58. [Google Scholar]
[11]. Logan PM, Primack SL, Miller RR, Muller NL, Invasive aspergillosis of the airways: Radiographic, CT & pathological findingsRadiology 1994 193:383-88. [Google Scholar]
[12]. Brown MJ, Worthy SA, Flint JDA, Muller NL, Invasive aspergillosis in immunocompromised host: utility of CT and bronchoalveolar lavageClin Radiol 1998 53:255-57. [Google Scholar]
[13]. Collins J, Stern EJ, Chest radiology, the essentials 2007 Lippincott Williams & WilkinsISBN:0781763142 [Google Scholar]
[14]. Müller NL, Franquet T, Lee KS, Imaging of pulmonary infections 2007 Lippincott Williams & WilkinsISBN:078177232X [Google Scholar]
[15]. Saraceno JL, Phelps DT, Ferro TJ, Futerfas R, Schwartz DB, Chronic necrotizing pulmonary aspergillosis: approach to managementChest 1997 112(2):541-48. [Google Scholar]
[16]. Agarwal K, Chowdhary A, Gaur SN, A rare case of allergic bronchopulmonary aspergillosis in a patient with chronic obstructive pulmonary diseaseIndian J Allergy Asthma Immunol 2012 26:20-24. [Google Scholar]
[17]. Agarwal R, High attenuation mucoid impaction in allergic bronchopulmonary aspergillosisWorld J Radiol 2010 2(1):41-43. [Google Scholar]
[18]. Ward S, Heynemn L, Lee MI, Leung AN, Hansell DM, Müller NL, Accuracy of CT in the diagnosis of allergic bronchopulmonary aspergillosis in asthmatic patientsAJR Am J Roentgenol 1999 173:937-42. [Google Scholar]
[19]. Chowdhary A, Agarwal K, Kathuria S, Gaur SN, Randhawa HS, Meis JF, Allergic bronchopulmonary mycosis due to fungi other than Aspergillus: a global overviewCrit Rev Microbiol 2014 40(1):30-48. [Google Scholar]
[20]. Aquino SL, Lee ST, Warnock ML, Gamsu G, Pulmonary aspergillosis: imaging findings with pathologic correlationAJR Am J Roentgenol 1994 163:811-15. [Google Scholar]
[21]. Franquet T, Müller NL, Giméne A, Guembe P, de la Torre J, Bagué S, Spectrum of pulmonary aspergillosis: histologic, clinical, and radiologic findingsRadiographics 2001 21:825-37. [Google Scholar]
[22]. Enelow RI, Hypersensitivity pneumonitis. In: Fishman AP, Elias JA, Fishman JA, Grippi MA, Senior RM, Pack AI (eds)Fishman’s Pulmonary Diseases and Disorders 2008 4th edUSATata McGraw Hill:1161-72. [Google Scholar]
[23]. Patel A, Ryu J, Reed C, Hypersensitivity pneumonitis: current concepts and future questionsJ Allergy Clin Immunol 2001 108:661-70. [Google Scholar]
[24]. Kurup VP, Zacharisen MC, Fink JN, Hypersensitivity pneumonitisIndian J Chest Dis Allied Sci 2006 48:115-28. [Google Scholar]
[25]. Spagnolo P, Rossi G, Cavazza A, Bonifazi M, Paladini I, Bonella F, Hypersensitivity Pneumonitis: A Comprehensive ReviewJ Investig Allergol Clin Immunol 2015 25(4):237-50. [Google Scholar]
[26]. Souza CA, Müller NL, Flint J, Wright JL, Churg A, Idiopathic pulmonary fibrosis: spectrum of high-resolution CT findingsAJR Am J Roentgenol 2005 185:1531-39. [Google Scholar]
[27]. Lynch DA, Newell JD, Logan PM, King TE, Müller NL, Can CT distinguish hypersensitivity pneumonitis from idiopathic pulmonary fibrosis?AJR Am J Roentgenol 1995 165:807-11. [Google Scholar]