Brucellosis remains the most widespread zoonosis globally and in endemic regions it has great impact on human and animal health, economic development, agricultural trade and tourism [1,2]. Brucellosis in humans is acquired by direct contact with infected tissues, blood or lymph through conjunctiva or broken skin; ingestion of contaminated meat or dairy products and or inhalation of infectious aerosols especially in occupationally exposed persons [2–5]. Though brucellosis in India was reported long back in the year 1942 and all the conditions conducive for the spread of human brucellosis exist like close contact with animals, unhygienic conditions, poverty, illiteracy, lack of awareness among population and physicians it still remains neglected [6,7]. In this point of view high incidence of brucellosis may be expected in Indian population especially among occupationally exposed groups. However, very limited studies have been undertaken on brucellosis in occupationally-exposed groups and the studies done have focused mainly on seroprevalence and majority of them have studied a single occupational group [8–11]. Risk factors and knowledge, attitude and practice (KAP) levels have not been evaluated.
The purpose of this study was to investigate the prevalence of anti-brucellar antibodies among occupationally exposed groups and to evaluate the clinical features, epidemiological data, and possible risk factors and to assess the KAP levels.
Materials and Methods
This cross-sectional study was conducted in the Department of Microbiology, BLDE University’s Shri BM Patil Medical College, Vijapur, Karnataka, over a period of four years and two months (Oct 2008-Dec 2012). During this period brucella antibody screening camps were organized for occupationally exposed individuals. Totally 17 camps were conducted and 2337 individuals were screened. The study was approved by the institutional ethical committee.
First, the rationale behind the study was explained to all the study subjects and consent to participate was obtained from adults and from parents in paediatric age group (1-14 years) before collecting the sample.
Inclusion criteria: Individuals who had contact with animals/animal products/Brucella cultures in their daily routine like veterinarians, shepherds, milk vendors/dairy workers, abattoirs, farmers and laboratory workers who gave consent to participate were included in the study .
Exclusion criteria: Individuals who had no contact with animal/animal products/brucella cultures were excluded from the study and individuals who did not give consent were excluded from the study.
About three ml of blood sample was collected from each individual, allowed to clot; serum was separated and used for serological study. All the participants were interviewed with a pre-designed questionnaire regarding age, sex, nature of work, duration of contact with animal/animal products/brucella culture, educational level, food habits, residential area, and clinical features in local language by a trained person.
Serological study was done using the Rose Bengal Plate test (RBPT), Serum Agglutination Test (SAT) and 2- Mercaptoethanol test (2-ME). Antigens for RBPT and SAT tests were procured from Indian Veterinary Research Institute, Izatnagar, UP. The tests were performed according to manufacturer’s guidelines. For 2-ME test, the dilution of serum was made in 0.85% saline containing 0.1M 2-ME in place of phenol saline. Test results were noted after 20±2h of incubation at 370C in the water bath. For each serum, sample titres were noted after comparing the tubes in the test series with the antigen control tubes for the degree of opacity of the supernatant fluid. The results were analysed using GraphPad InStat designed by GraphPad Software Inc.
Results
Of the 2337 high-risk group subjects screened, 222 showed positive reaction by RBPT. Titres between 40-5120 IU and 40-2560 IU could be demonstrated in 219 and 121 subjects by SAT and 2-ME tests. The mean SAT and 2-ME titres were 280.58 ± 469.55 and 106.79 ± 193.95. Significant SAT (≥160 IU) and 2-ME (≥80 IU) titres were demonstrated in 106 (4.5%) and 87 (3.72%) individuals [Table/Fig-1]. When compared to SAT, 2-ME test had positive and negative predictive values of 100% and 99.16% respectively.
Anti-brucellar antibody test results in various occupational groups.
| High-risk group | No.Screened | PositiveRBPT | Significant titers |
|---|
| SAT (≥160 IU) | 2ME test (≥ 80 IU) |
|---|
| Veterinarians | 1086 | 103 (9.4) | 49 (4.5) | 42 (3.8) |
| Farm workers | 467 | 31 (6.6) | 09 (1.9) | 07 (1.4) |
| Dairy workers | 400 | 30 (7.5) | 14 (3.5) | 09 (2.2) |
| Abattoirs | 186 | 27 (14.5) | 16 (8.6) | 15 (8) |
| Shepherds | 146 | 31 (21.2) | 17 (11.4) | 14 (9.5) |
| Lab workers | 52 | 0 1(1.9) | 01 (1.9) | 00 |
| Total | 2337 | 223(9.5) | 106 (4.4) | 87 (3.6) |
| Test applied - χ2Test | χ2 =30.06,p< 0.0001 | χ2 =29.36,p< 0.0001 | χ2= 31.41,p< 0.0001 |
* Figures in parenthesis indicate percentage.
Among various occupational groups screened seropositivity was found to be highest in shepherds followed by abattoirs. Clinical history at the time of blood collection revealed 98 subjects (49 veterinarians, 11 farm workers, 9 dairy workers, 15 abattoirs and 14 shepherds) with symptoms that could be co-related with brucellosis. The commonest clinical symptoms were joint pain, fever, low backache, myalgia [Table/Fig-2].
Clinical manifestations in occupationally exposed individuals.
| Symptoms | Number |
|---|
| Fever | 69 |
| Joint Pain | 73 |
| Low backache | 49 |
| Myalgia | 15 |
| Night Sweating | 112 |
| Fatigue, | 11 |
| Headache | 07 |
| Weight Loss | 04 |
| Orchitis | 03 |
| Cough | 02 |
Of these 98 symptomatic cases significant 2-ME titres were demonstrated in 87. Remaining 11 (7 veterinarians+2 farmers+2 abattoirs) symptomatic individuals though showed positive RBPT and significant SAT titres, their 2-ME titres were insignificant. Amongst the 2239 asymptomatic individuals, 116 showed positive RBPT and significant SAT titres were noted in 13 (6 veterinarians+2 farmers+4 abattoirs+1shepherd) individuals, but none had significant 2-ME titres. Repeat serology in 11 symptomatic and 13 asymptomatic individuals with significant SAT titres but insignificant 2-ME titres did not show any rise on twice fortnightly follow up, hence were considered as inactive brucellosis cases.
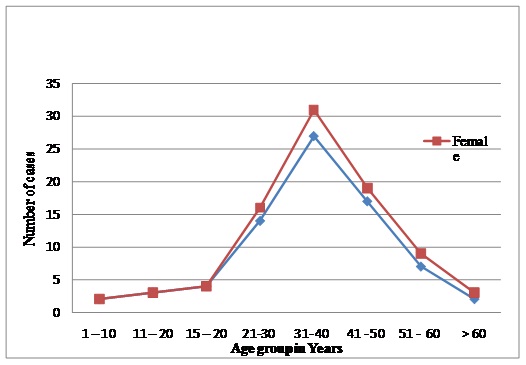
Age range of the cases with significant 2-ME titres was 3-74 years with mean ± SD being 37.00±13.04 years. The most commonly affected age group was 31-40 years and five patients (3 shepherds, 2 abattoirs) were in the paediatric age. Male preponderance was found in the study with 69 males and 11 females [Table/Fig-3]. The risk factors for brucellosis are depicted in [Table/Fig-4].
Age & sex distribution of Brucellosis cases with significant 2-ME titres.
Risk factors for brucellosis in occupationally exposed group individuals.
| Risk factors | No.screened | AE* | RMI† | AE + RMI ‡ | AE+RMPI § | LE || |
|---|
| Veterinarians | 1086 | 995 (91.78) | 0 | 91 (8.37) | 0 | - |
| Farmers | 467 | 216 (46.25) | 0 | 251 (53.74) | 0 | - |
| Dairy workers | 400 | - | 281 (70.25) | 119 (29.75) | 0 | - |
| Abattoirs | 186 | 105 (56.45) | 0 | 73(39.24) | 8 (4.3) | - |
| Shepherds | 146 | 0 | 0 | 146 (100) | 0 | 0 |
| Lab workers | 52 | 0 | 0 | 0 | 0 | 52 (100) |
| Total | 2337 | 1316 (56.31) | 281(12.02) | 680 (29.09) | 8 (0.34) | 52 (2.22) |
Figures in parenthesis indicate percentage
*Animal exposure, †Raw milk ingestion, ‡AE+RMI-Animal exposure & Raw milk ingestion, §Animal exposure & Raw meat product ingestion, || Laboratory exposure
Duration of contact with probable source of infection was found to be highest in shepherds followed by abattoirs and farmers. Knowledge and attitude regarding brucellosis and preventive practices followed are given in [Table/Fig-5,6]. Except in veterinarians, no relation could be established between educational qualification and KAP levels regarding brucellosis. Also no significant association was found between brucella seropositivity and residential status (urban/rural).
Knowledge and attitude regarding brucellosis among occupationally exposed individuals.
| Category | No.screened | Knowledge regarding | Attitude |
|---|
| Disease Existence | Routes of transmission | ClinicalFeatures | PreventiveMeasures |
|---|
| Skin | Ingestion | Inhalation | Conjunctiva |
|---|
| Veterinarians | 1086 | 1086 (100) | 1086 (100) | 631 (58.1) | 242 (22.28) | 181 (16.66) | 536 (49.35) | 593 (54.6) | 548 (50.46) |
| Farmers | 467 | 00 | 00 | 00 | 00 | 00 | 00 | 00 | – |
| Dairy workers | 400 | 62 (15.5) | 62 (15.5) | 62 (15.5) | 00 | 00 | 00 | 00 | — |
| Abattoirs | 186 | 00 | 00 | 00 | 00 | 00 | 00 | 00 | — |
| Shepherds | 146 | 00 | 00 | 00 | 00 | 00 | 00 | 00 | — |
| Lab workers | 52 | 52 (100) | 52 (100) | 52 (100) | 52 (100) | 52 (100) | 52 (100) | 52 (100) | 52 (100) |
| Total | 2337 | 1200 (51.34) | 1200 (51.34) | 745 (31.87) | 294 (12.58) | 233 (9.97) | 588 (25.16) | 645 (27.59) | 600 (25.67) |
| χ2 Test | p < 0.0001 |
Figures in parenthesis indicate percentage
Preventive practices followed by occupationally exposed individuals.
| Category | No. Screened | Use of personal protective Equipment | ProperHand washing | ProperWaste disposal |
|---|
| Gowns | Gloves | Eye wear | Mask |
|---|
| Veterinarians | 1086 | 276(25.4) | 31(2.8) | 45(4.1) | 00 | 1086(100) | 158(14.5) |
| Farmers | 467 | 00 | 00 | 00 | 00 | 329(70.4) | 00 |
| Dairy workers | 400 | 00 | 00 | 00 | 00 | 400(100) | 00 |
| Abattoir workers | 186 | 00 | 00 | 00 | 00 | 186(100) | 00 |
| Shepherds | 146 | 00 | 00 | 00 | 00 | 39(26.7) | 00 |
| Lab workers | 52 | 52(100) | 52(100) | 52(100) | 52(100) | 52(100) | 49(94.2) |
| Total | 2337 | 49(94.2) | 83(3.5) | 97(4.1) | 52(2.2) | 2092(89.5) | 207(8.8) |
| χ2 Test | p<0.0001 | p<0.0001 | p< 0.0001 |
Figures in parenthesis indicate percentage
Discussion
In this study the prevalence rate of brucellosis by RBPT was 9.5%. Agasthya et al., from Karnataka and Kumar Arvind et al., from Kerala have reported lesser prevalence rate (2.74% and 2.26%) [11,12]. Whereas studies from Iran and Jordan have reported nearing rates [13–15].
Statistically significant difference in seropositivity was seen in various categories of occupationally exposed groups and highest positivity was observed in shepherds followed by abattoirs [Table/Fig-1].
Symptoms that could be associated with brucellosis were noted in 91 (4.37%) individuals [Table/Fig-2]. Joint pain, fever, low backache, myalgia, night sweats, fatigue were the common symptoms experienced which have also been noted by other authors [11,13]. These individuals were diagnosed as cases of pulmonary tuberculosis/ malaria/ typhoid /TB spine etc. and were treated for respective diseases with no much relief and hence many of them changed the doctors frequently. Similar findings of misdiagnosis of brucellosis have been reported in the literature [3,16]. Of the 91 symptomatic individuals 11 has significant SAT titres but their 2-ME titres were insignificant.
Amongst the asymptomatic group, 13 (0.65%) individuals though showed significant SAT titres (≥160IU), their 2-ME titres were insignificant (<80IU). Presence of antibodies to Brucella species in asymptomatic high-risk group individuals ranging from 14-81% has been reported in various studies [11,17,18]. The significant SAT titers among the asymptomatic group might be due to inactive brucellosis or repeated exposure to antigenic stimuli, as has been reported by some authors [18–21].
In this study 11 symptomatic and 13 asymptomatic individuals with significant SAT and insignificant 2-ME titres did not show any rise on follow-up, indicating inactive brucellosis. These cases would have been unnecessarily treated if only RBPT and SAT titres were taken into consideration. Hence more weightage should be given to 2-ME titre as it is a better correlate of an active brucellosis requiring treatment which has been reported by Buchanan et al., [22].
Major age group affected was 31-40 years (30%) followed by 41-50 years (23.75%) [Table/Fig-3] Mukhtar F. has reported similar findings [23]. Five subjects in our study (6.25%) were in the paediatric group and the youngest was 3 years. The eldest patient in the study was 74-year-old. Increase in prevalence of Brucella antibodies with age in high-risk group individuals has been reported by Abo-Shehada et al., Ramos et al., and Nikokar et al., [15,19,24]. No such correlation could be established between age and seroprevalence in our study.
Though difference in seropositivity was noted between males and females, it was of no statistical relevance due to less number of female participants and does not depict the true picture.
Regarding risk factors, in veterinarians brucellosis was strongly associated with handling of animals especially manipulation of foetus and placenta [Table/Fig-4]. Similar findings have been reported by Ramos et al [19]. Apart from handling, the animals at work place, 8.1% of veterinarians had kept milking animals at home and had consumed raw milk. Majority of farm workers in this study invariably reared small ruminants (especially goats) along with cow and buffalo. The major risk factors noted were both animal exposure as well as raw milk ingestion, 53.7% of farmers consumed raw milk regularly; either directly or with warm tea. In 46.2% of subjects, animal exposure alone was noted as the risk factor. In the dairy workers group, raw milk ingestion and contact with raw milk (70.25%) were the major risk factors. History of both animal exposure either at work place or at home along with raw milk contact and consumption was seen in 29.75% of individuals. Omer et al., have reported contact with animal especially sheep, as a risk factor among dairy farm workers [25]. In this study, dairy workers were exposed to cows and/or buffaloes/goat but not to sheep. Exposure to animal viscera and blood splashes was the major risk factor in abattoir workers. There was no demarcation in the type of work carried out by abattoirs as reported by Mukhtar F, depending upon the need all had performed all the types of work [23]. Apart from above mentioned risk factors 18.2% abattoirs had kept goats at home and consumed raw milk. Consumption of bone marrow was noted in 4.3% subjects. Risk factors in shepherds were both animal exposure and raw milk ingestion (sheep, goat). All of them had close contact with animals and consumed raw milk, conducted deliveries, dystocia, abortion cases in the fields. Most of them also practiced cutting of umbilical cords with their teeth after parturition of animals. Adel Shehata et al., have reported similar findings from Kuwait [26]. Exposure to brucella cultures was the major risk factor amongst the laboratory workers. These individuals worked in the laboratories where brucella culture was carried out regularly.
All the veterinarians had heard about the disease, but only 20.67% (171/827) were aware about all the routes of transmission and precautionary measures to be followed [Table/Fig-5]. None of them had used personal protective equipment while handling the animals [Table/Fig-6]. Amongst the 400 dairy workers 62 (15.5%) knew about the disease and its routes of transmission. All of them were working in organized dairies where awareness programmes were being conducted. Few individuals engaged in milking of animals in unorganized dairy farms consumed raw milk directly from udders before they collected it in the containers. Farm workers, shepherds, abattoirs and 84.5% of dairy workers had never heard about brucellosis and hence did not follow any preventive practices. KAP levels regarding brucellosis were 100% in the laboratory workers.
Conclusion
KAP levels regarding brucellosis in high-risk group were very poor. Most of the high risk group individuals (shepherds, abattoirs, and farmers) had never heard about brucellosis. Regular periodic brucellosis screening and awareness programmes are needed to control brucellosis in high-risk subjects. Due to protean clinical manifestations of human brucellosis and ignorance among the physicians about its existence, it is often missed or misdiagnosed. Hence awareness among local doctors about the disease is also necessary to avoid delay in the treatment. Furthermore availability of basic laboratory testing facility for brucellosis in rural as well as urban areas is required to differentiate active and inactive brucellosis, to support the clinical diagnosis and treatment.
* Figures in parenthesis indicate percentage.
Figures in parenthesis indicate percentage
*Animal exposure, †Raw milk ingestion, ‡AE+RMI-Animal exposure & Raw milk ingestion, §Animal exposure & Raw meat product ingestion, || Laboratory exposure
Figures in parenthesis indicate percentage
Figures in parenthesis indicate percentage