Bowel Herniation Through 5mm Port Site: An Unusual Complication
Shibumon Mundunadackal Madhavan1, Vamsi Krishna Potunru2, Alfred Joseph Augustine3
1 Associate Professor, Department of General Surgery, Kasturba Medical College Hospital, Mangalore, Manipal University, Karnataka, India.
2 Assistant Professor, Department of General Surgery, Kasturba Medical College Hospital, Mangalore, Manipal University, Karnataka, India.
3 Professor, Department of General Surgery, Kasturba Medical College Hospital, Mangalore, Manipal University, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shibumon Mundunadackal Madhavan, Associate Professor Department of General Surgery, Kasturba Medical College, Mangalore, Karnataka-575001, India.
E-mail: drshibumon@yahoo.com
Trocar site herniation is a rare complication following laparoscopic surgery. We report a case of small bowel herniation through 5mm port site following laparoscopic myomectomy. A 36-year-old lady underwent laparoscopic myomectomy. On the fourth postoperative day she developed features of intestinal obstruction. Further evaluation with CT scan showed herniation of a loop of small bowel through the 5mm port site in right iliac fossa. Surgical exploration of the port site revealed a herniated loop of viable small bowel. The enlarged facial defect was closed after reduction of the bowel. Patient recovered uneventfully. Bowel herniation through 5mm port site is a rare complication which requires prompt diagnosis and immediate treatment to avoid morbidity.
Port site herniation, Intestinal obstruction, Laparoscopy
Case Report
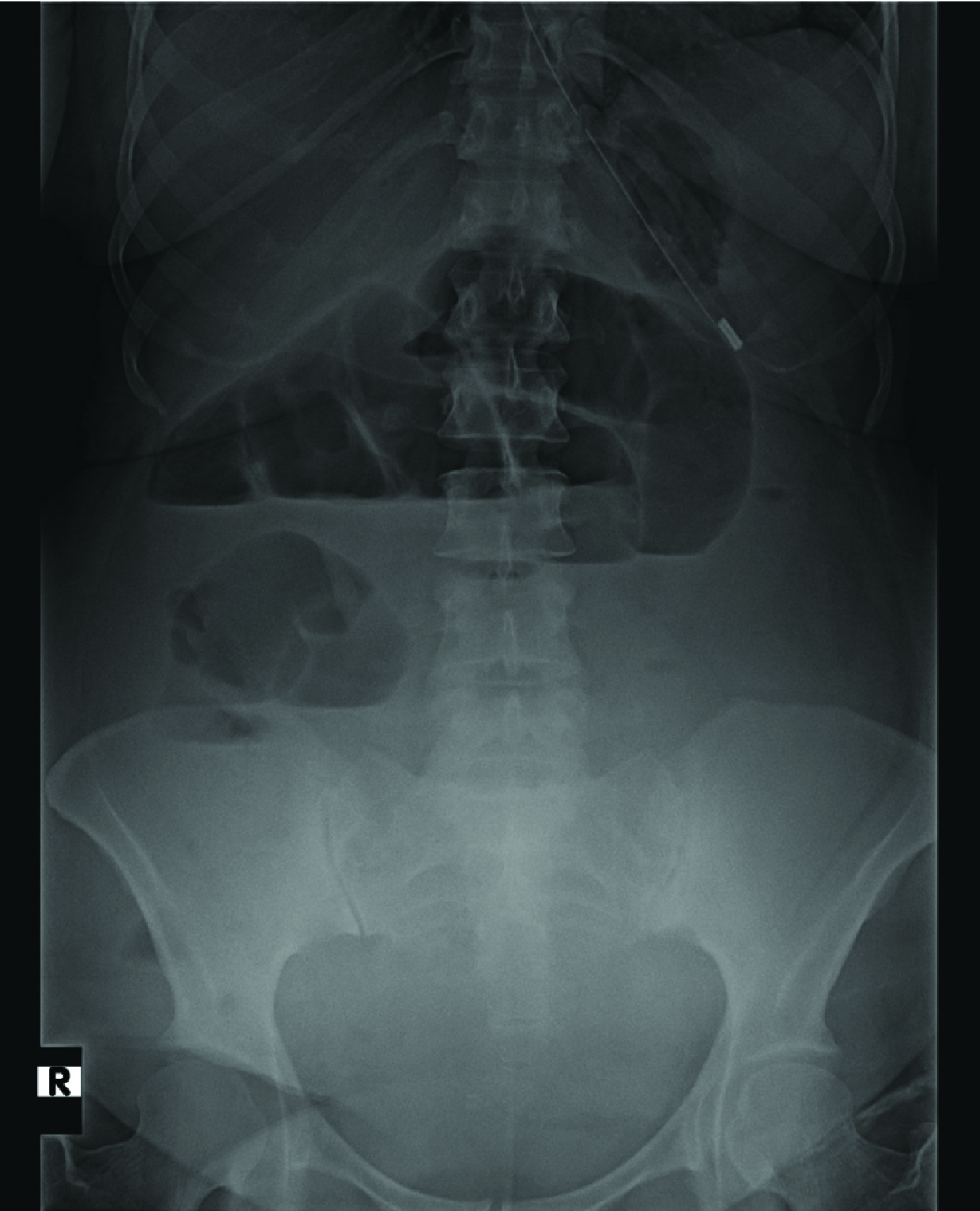
A 36-year-old female underwent laparoscopic myomectomy for symptomatic uterine fibroids of 18 week size. An 11-mm umbilical trocar was placed by open technique, followed by 3 additional 5-mm ports in the right, left, and suprapubic regions under direct visualization. The suprapubic port site was expanded to 14-mm for morcellation. Umbilical and suprapubic the fascia was later closed with 2 interrupted 0 polyglactin sutures. The 5-mm fascial incisions were not closed. Patient had uneventful surgery except for longer duration due to technical difficulty in dissecting out the large fibroid and removal of the specimen by morcellation. Patient had uneventful postoperative course, was on orals, ambulant and had bowel movements for two days, on 3rd day patient developed fever, abdominal pain and vomiting. Abdominal examination was essentially within normal limits. Urine examination showed numerous pus cells. She was treated as urinary tract infection and had symptomatic improvement. Blood culture and urine culture sent subsequently grown Pseudomonas and Klebsiella On 4th post op day patient continued to have vomiting and there was distension of abdomen. Clinical examination and abdominal X ray showed features of small bowel obstruction [Table/Fig-1]. CT scan of the abdomen showed herniation of a loop small bowel through the 5mm port site in the right iliac fossa [Table/Fig-2]. Patient was immediately taken for surgery. Local exploration of the 5mm port site was done under general anaesthesia. Intraoperatively there was a herniated loop of ileum lying in the deep subcutaneous plane [Table/Fig-3]. The 5mm musculo- facial defect had enlarged to more than 2cm. The bowel which was viable was reduced and musculo-facial defect was closed with interrupted 1-0 Polypropylene sutures. Patient had an uneventful recovery and was discharged after two days.
Abdominal X ray showed features of small bowel obstruction.
CT scan of the abdomen showed herniation of a loop small bowel through the 5mm port site in the right iliac fossa.

Intra operative view showing there was a herniated loop of ileum lying in the deep subcutaneous plain.

Discussion
Laparoscopic surgery has been refined over last two decades and become the standard of care for many surgical conditions. Trocar-site hernias are a rare but known complication of laparoscopic surgery. Incidence of port site hernias range from 0.2%- 3.1% [1,2]. Trocar site hernias have been classified by Hitoshi et al into three groups based on the pathology [3]. Most of the port site hernias occur through the ports of 10mm size or more and through umbilical or midline site. There are very few reported cases of hernias through 5mm port site [4–7]. Risks factors for developing a trocar-site hernia like increased BMI, midline insertion, size, number and type of trocar tips, excessive manipulation of the trocar site etc. have already been identified [3,7]. Usage of larger size trocars of 10mm diameter or more carries an increased risk of herniation [1]. The current practice is to close the fascial defects of 10mm or more. Smaller trocars are not routinely closed. Existing literature support non closure of blunt, radially expanding trocars and also laterally placed trocars [1]. Even though few authors suggest fascial closure of 5 mm trocars following excessive trocar manipulation, the literature does not support routine closure [2,7]. Very few cases of herniation of bowel through 5mm port site have been reported in the literature [1,2,4–7]. Bowel herniation is unlikely through 5mm fascial defects unless they are enlarged to considerable size. The most important factor which predisposes to herniation in 5mm port site is probably excessive trocar manipulation. Available literature about 5mm port site herniation also supports excessive trocar manipulation as the major cause [1,2,6]. Moreaux G et al., reported two cases of bowel herniation following removal of drains inserted through 5mm port sites and suggested insertion of drains through the port site as potential cause for herniation [5]. These patients also probably had excessive trocar manipulation for prolonged surgery (hysterectomy bilateral salpingo-oophorectomy and pelvic lymphadenectomy). Excessive trocar manipulations in the form of multiple reinsertions, difficult dissection requiring more force and torque on the fascia and prolonged operative time cause stretching of fascial and peritoneal defect. Nezhat C et al., who has reported maximum number of hernias through 5mm port site also recommends closure of fascia of 5mm port when there is excessive manipulation [2]. Hitoshi et al., analysed the factors related to trocar site hernia and no independent risk factor was identified [3].
Conclusion
Bowel herniation through 5mm port site is a rare complication. Most important predisposing factor for 5mm port site herniation is probably excessive trocar manipulation, which enlarges the fascial defect to considerable size where the skin opening remain 5mm. Currently there is no evidence in literature for recommending routine fascial closure of 5mm trocar site; however it is advisable to close the fascia of 5mm trocar site following prolonged and difficult surgeries where there is excessive trocar manipulation. Removal of the trocars under vision inspection and closure of the defect if enlarged will prevent this complication.
[1]. Yamamoto M, Minikel L, Zaritsky E, Laparoscopic 5-mm Trocar Site Herniation and Literature ReviewJSLS 2011 15(1):122-26. [Google Scholar]
[2]. Nezhat C, Nezhat F, Seidman DS, Nezhat C, Incisional hernias after operative laparoscopyJ Laparo endosc Adv Surg Tech 1997 7(2):111-15. [Google Scholar]
[3]. Tonouchi H, Ohmori Y, Kobayashi M, Kusunoki M, Trocar Site HerniaArch Surg 2004 139(11):1248-56. [Google Scholar]
[4]. Dulskas A, Lunevicius R, Stanaitis J, A case report of incisional hernia through a 5 mm lateral port site following laparoscopic cholecystectomyJ Min Access Surg 2011 7:187-89. [Google Scholar]
[5]. Moreaux G, Estrade-Huchon S, Bader G, Gyot B, Heitz D, Fauconnier A, Five-millimeter trocar site small bowel eviscerations after gynecologic laparoscopic surgeryJ Minim Invasive Gynecol 2009 16(5):643-45. [Google Scholar]
[6]. Reardon PR, Preciado A, Scarborough T, Matthews S, Marti JL, Hernia at 5-mm Laparoscopic Port Site Presenting as Early Postoperative Small Bowel ObstructionJournal of Laparoendoscopic & Advanced Surgical Techniques 1999 9(6):523-25. [Google Scholar]
[7]. Khurshid N, Chung M, Horrigan T, Manahan K, Geisler JP, 5 Millimeter Trocar-Site Bowel Herniation Following Laparoscopic SurgeryJSLS 2012 16(2):306-10. [Google Scholar]