Anastomotic Leakage in a Patient with Acute Intestinal Obstruction Secondary to Appendiceal and Ileal Endometriosis: A Case Report
Ilker Murat Arer1, Hakan Yabanoglu2, Bermal Hasbay3
1 Department of General Surgery, Baskent University Adana Teaching and Research Center, Adana, Turkey.
2 Assistant Professor, Department of General Surgery, Baskent University Adana Teaching and Research Center, Adana, Turkey.
3 Department of Pathology, Baskent University Adana Teaching and Research Center, Adana, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ilker Murat Arer, Department of General Surgery, Baskent University Adana Teaching and Research Center, Dadaloglu District-2591, Street No:4/A 01250 Yuregir, Adana / Turkey.
E-mail: igy1981@yahoo.com
Endometriosis is a commonly encountered problem in women of reproductive age. It usually causes chronic abdominal pain. However, it rarely causes complications such as intestinal obstruction. The most commonly performed procedure for these patients is bowel resection and anastomosis. Unless it is complicated with anastomotic leakage. We present a 39-year-old woman presented with intestinal obstruction due to appendiceal and ileal endometriosis complicated with anastomotic leakage after surgery.
Abdominol, Bowel, Gastrointestinal Endomertiosis, Ileostomy, leak
Case Report
A 39-year-old female patient was admitted to the Emergency Department with a complaint of abdominal pain, abdominal distention and constipation. Abdominal distention was present for 3 days accompanied with nausea and vomiting for over a day. The patient had a history of cyclic gastrointestinal problems like abdominal pain, constipation and nausea. She was admitted to the same hospital with these symptoms 3 months ago and the abdominal Computerized Tomography (CT) yielded no pathological findings.
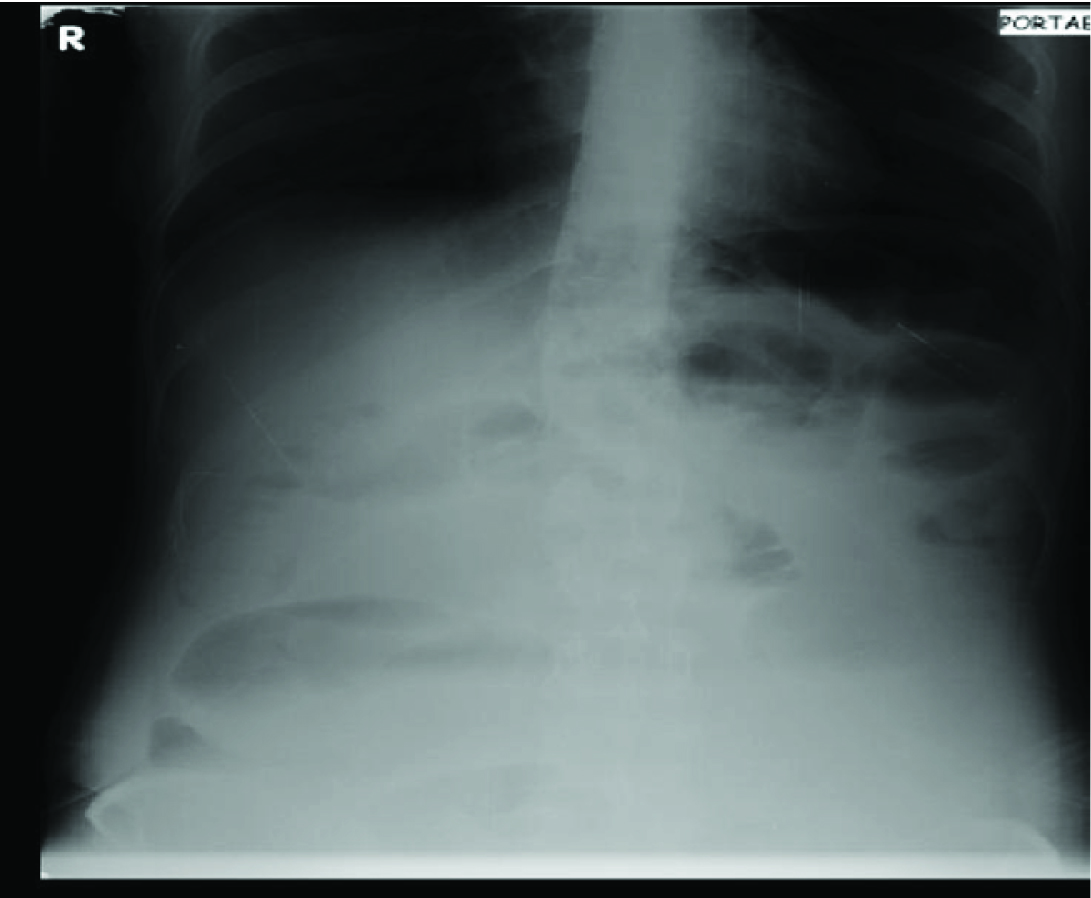
On her second admission to the Emergency Department severe abdominal distention, hyperactive bowel sounds, abdominal tenderness and rebound in all four quadrants were observed on physical examination. Digital rectal examination was normal. Laboratory tests revealed a normal white cell count of 7900/mm3 and a normal haemoglobin of 12.8 g/dL. Plain abdominal X-ray was consistent with a few small bowel loops [Table/Fig-1]. Patient was hospitalized and transfered to operating room. Laparatomy was done via midline incision. On exploration all ileal segments were dilated and obstruction was observed 5cm proximal to terminal ileum. Stricture-like intraluminal growth pattern of the tumour was observed. Proximal to the tumour 2 serosal implants were seen macroscopically. A 25cm of ileal segment was resected together with terminal ileum and ileocolic end-to-side anastomosis was done by 2-layered vicryl sutures. Drainage catheters were placed at right paracolic gutter and pelvis. Postoperatively patient was followed in General Surgery Ward. Anastomosis leakage was observed on postoperative day 5 and relaparatomy was performed urgently. Anterior side of the anastomosis was seperated completely. Resection of cecum and maturation of double barrel ileostomy on right lower quadrant of the abdomen was done. Patient received wide-spectrum antibiotic treatment postoperatively and was discharged on postoperative day 10 with no other complication.
Plain abdominal X-Ray of the patient showing small bowel loop.
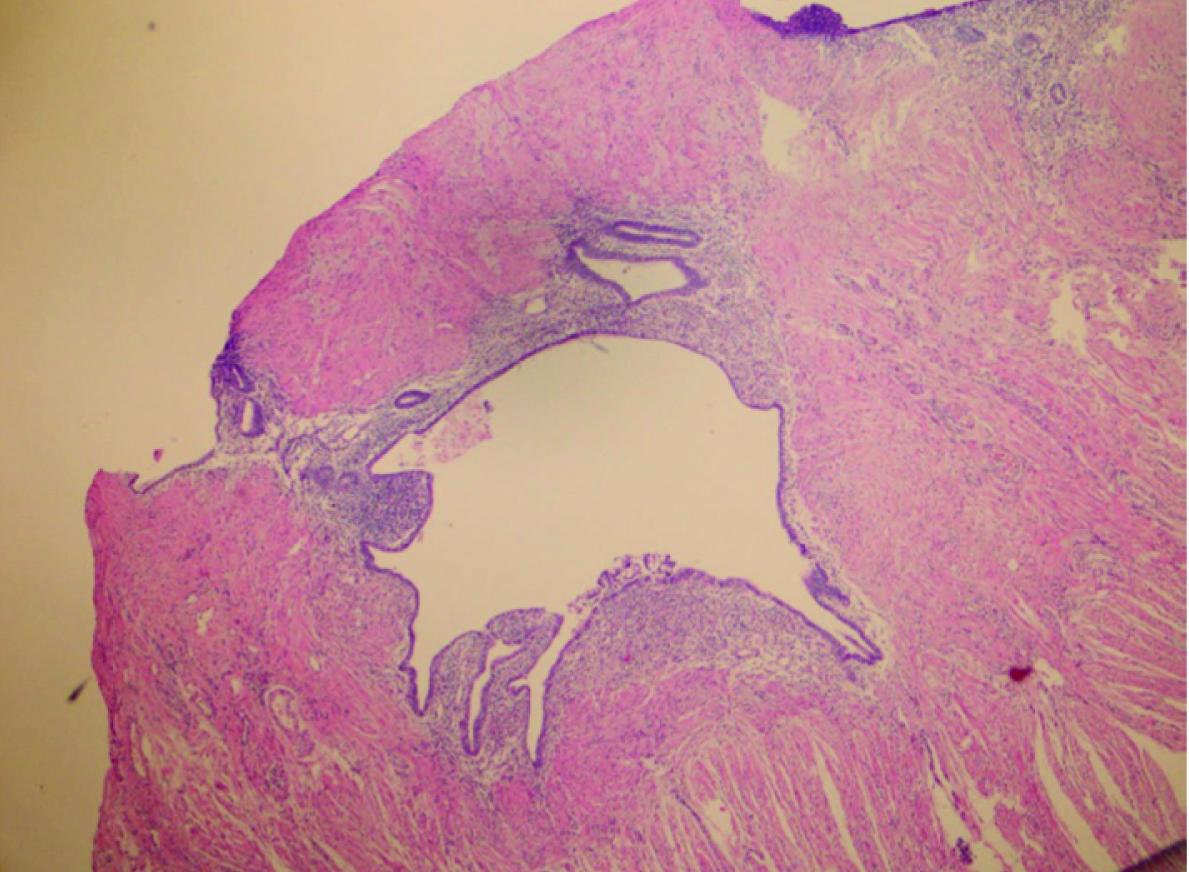
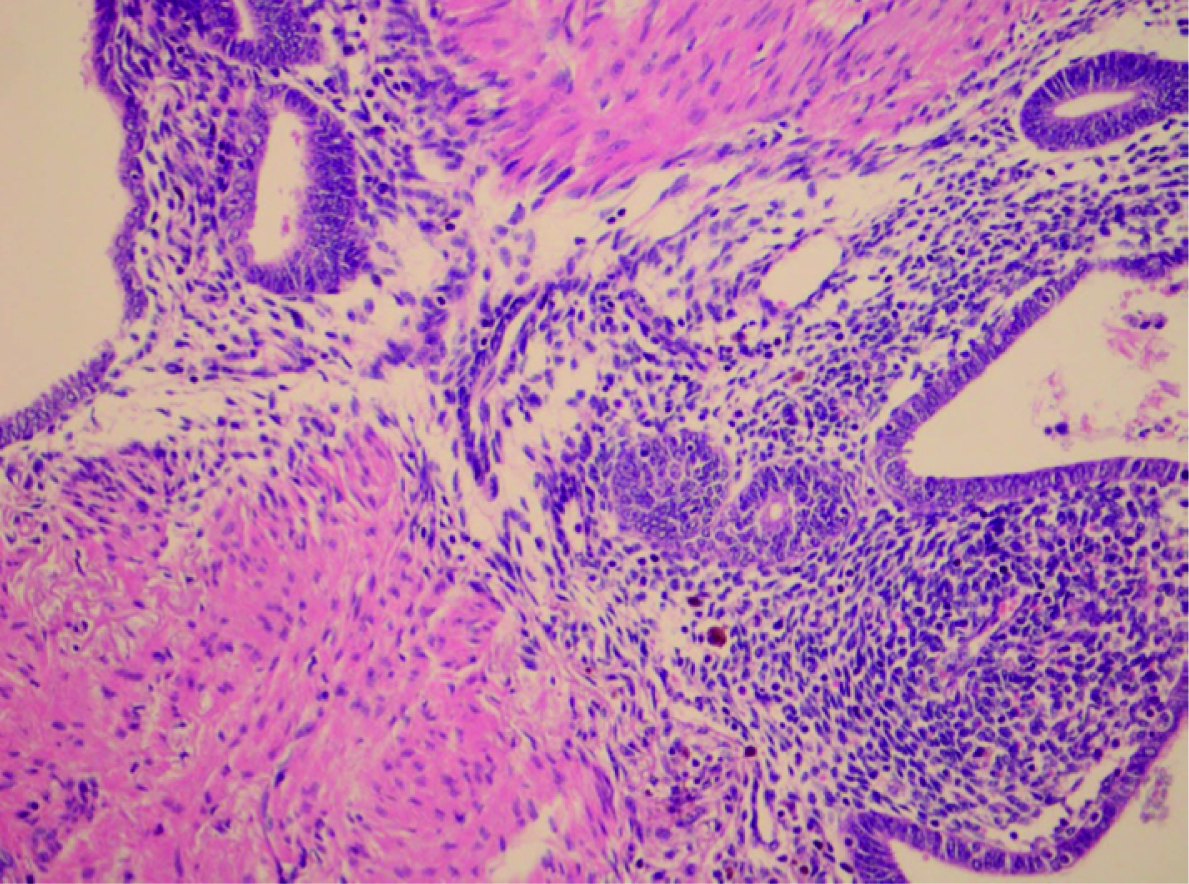
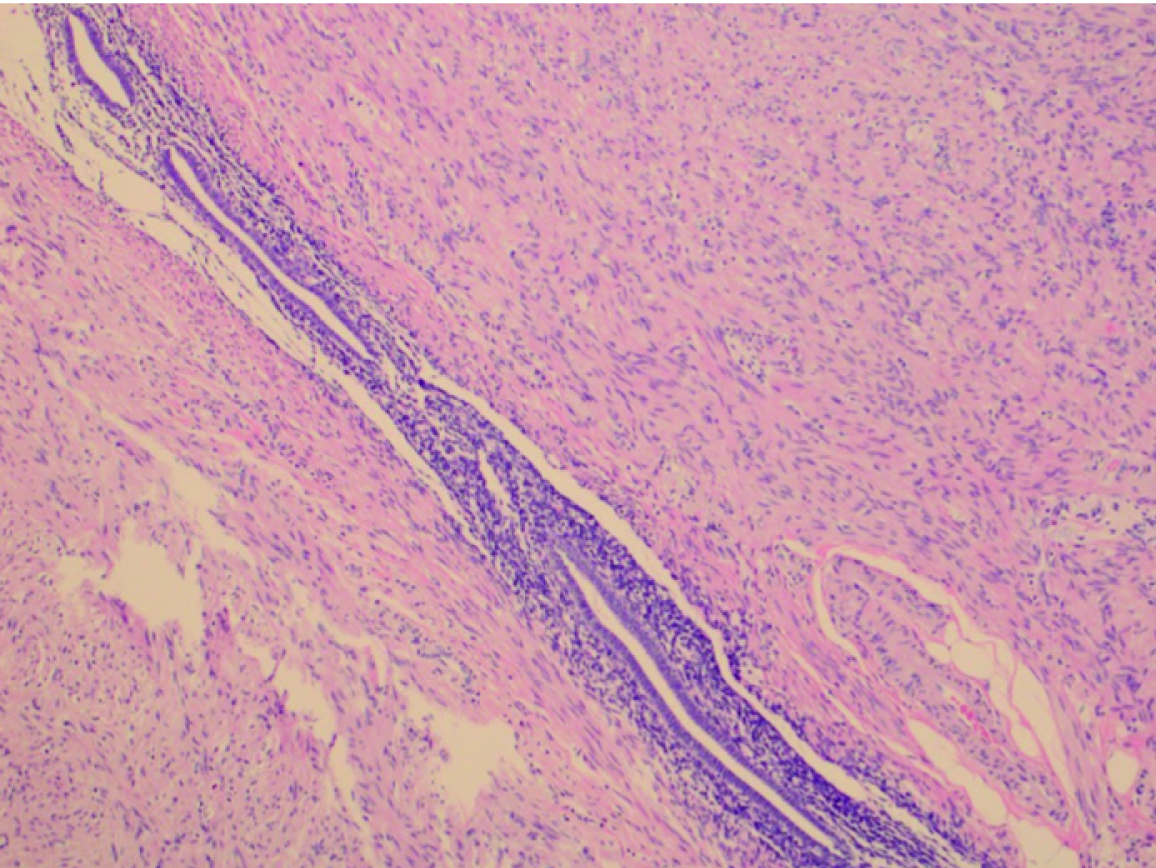
The microscopic findings were; endometrial gland and stroma in a focal field of ileum mucosa causing desquamation, erosion and obstruction [Table/Fig-2,3]. Endometrial gland and stroma was also found in the appendix [Table/Fig-4]. Hence the pathological diagnosis was endometriosis in appendix and ileum.
Endometrial gland and stroma in ileal muscular layer (H&E x40).
Endometrial gland and stroma and haemosiderin-laden macrophages (H&E x200).
Endometrial gland and stroma in appendiceal muscular layer (H&E x100)
Discussion
Endometriosis (EM) is the presence of benign functional endometrial tissue outside uterine cavity and is one of the most common cause of chronic pelvic pain in women of reproductive age. It is usually located in the pelvis but extrapelvic sites such as colon, intestines, inguinal hernia sac and abdominal scars after gynecological surgery have been reported [1]. Intestinal involvement of EM is reported to be 3-37% and appendiceal involvement <1% of all cases [2,3]. The most common sites in gastrointestinal system is sigmoid colon, rectum and distal ileum. Patients with gastrointestinal EM may present with symptoms such as chronic abdominal pain, abdominal distention, constipation and diarrhea. It may cause strictures, obstruction or even perforation of bowel [4,5]. Although the exact incidence of EM causing intestinal obstruction remains unclear, complete obstruction is seen <1% of all cases [6]. We present a case of both intestinal and appendiceal endometriosis in the same patient presenting with acute intestinal obstruction.
There are many theories about EM but the exact aetiology still remains unknown. Although clinical presentation is non-specific, patients usually have a complaint of cyclic abdominal pain. Bowel endometriosisis most commonly (70%) found on the rectosigmoid colon and distal ileum is affected in 1-7% of patients [7]. It is usually difficult to establish accurate diagnosis because similar symptoms are seen in diseases such as irritable bowel syndrome, infectious and inflammatory bowel disease. Our patient also had gradual onset of symptoms terminating with total obstruction of small bowel. Diagnostic work-up for these patients include; ultrasound or Magnetic Resonance Imaging (MRI). They have high sensitivity and specificity rates in pelvic endometriosis unless fail to diagnose extrapelvic EM [8]. If there is bowel obstruction, these preoperative diagnostic methods become unnecessary and explorating the abdominal cavity makes both diagnosis and treatment. Although gold standard of endometriosis is laparoscopy [2], in case of bowel obstruction urgent laparotomy and resection of the affected segment is indicated. But in literature most commonly performed procedure is right hemicolectomy [1,9]. One of the reason is that EM is usually located in terminal ileum and authors tend to accept and treat this lesion as malignant according to macroscopic appearance. We performed segmental small bowel resection and anastomosis but unfortunately leakage of anastomosis lead us to perform end ileostomy. But as a result of the second operation, pathology specimen yielded another focus of EM, appendiceal endometriosis which was undetectable in the first operation. Thandassery et al., performed ileum resection and end ileostomy in a patient with endometriosis in terminal ileum causing small bowel obstruction thus ileostomy is an alternative surgical method in patients with EM presenting with bowel obstruction [10]. Right hemicolectomy seems radical surgery for these patients. Karaman et al., also performed ileum resection and end ileostomy and avoided anastomosis because of the excessive dilatation of the proximal part of the ileum and high risk for anastomotic leakage [11]. Ridha et al., performed small bowel resection, end-to-end anastomosis and appendectomy [12]. Slesser et al., were also found the lesion suspicious with malignancy and performed right hemicolectomy [13]. Although resection of the affected segment with anastomosis seems a good option for the treatment, in cases with total obstruction of bowel lumen or suspicion of anastomotic leakage ileostomy can be performed safely.
The incidence of anastomotic leakage is between 1.8-8.4% [14,15]. Multiple factors may affect leakage after ileocolic anastomosis however mechanical bowel preparation is one of the most important factors among them [16] which is found to be significantly different from non-bowel preparation group (p<0.0001). We believe inability to perform mechanical bowel preparation is the reason anastomotic leakage in our patient.
Our case is unique in literature with anastomotic leakage after resection of the distal ileum and end-to-side anastomosis with implants of endometriosis causing bowel obstruction.
Conclusion
Although acute intestinal obstruction due to endometriosis is an uncommon condition, it should be suspected in reproductive age women with a history of chronic abdominal pain. Bowel resection and enterostomy is the optimal surgical treatment for these kind of patients.
[1]. De Ceglie A, Bilardi C, Blanchi S, Picasso M, Di Muzio M, Trimarchi A, Acute small bowel obstruction caused by endometriosis: a case report and review of the literatureWorld J Gastroenterol 2008 14(21):3430-34. [Google Scholar]
[2]. Revised American Society for Reproductive Medicine classificationof endometriosis: 1996Fertil Steril 1997 67:817-21. [Google Scholar]
[3]. Tumay V, Ozturk E, Ozturk H, Yilmazlar T, Appendiceal endometriosis mimickingacute appendicitisActa Chirurgica Belgica 2006 106(6):712-13. [Google Scholar]
[4]. Lin YH, Kuo LJ, Chuang AY, Cheng TI, Hung CF, Extrapelvic endometriosis complicated with colonic obstructionJ Chin Med Assoc 2006 69:47-50. [Google Scholar]
[5]. Varras M, Kostopanagiotou E, Katis K, Farantos CH, Angelidou-Manika Z, Antoniou S, Endometriosis causing extensive intestinal obstruction simulating carcinoma of the sigmoid colon: a case report and review of the literatureEur J Gynaecol Oncol 2002 23:353-57. [Google Scholar]
[6]. de Bree E, Schoretsanitis G, Melissas J, Christodoulakis M, Tsiftsis D, Acute intestinal obstruction caused by endometriosis mimicking sigmoid carcinomaActa Gastroenterol Belg 1998 61:376-78. [Google Scholar]
[7]. Macafee CH, Greer HL, Intestinal endometriosis. A reportof 29 cases and a survey of the literatureJ Obstet Gynaecol Br Emp 1960 67:539-55. [Google Scholar]
[8]. Takeuchi H, Kuwatsuru R, Kitade M, Sakurai A, Kikuchi I, Shimanuki H, A novel technique using magnetic resonance imaging jelly for evaluation of rectovaginal endometriosisFertil Steril 2005 83:442-47. [Google Scholar]
[9]. Khwaja SA, Zakaria R, Carneiro HA, Khwaja HA, Endometriosis: a rare cause of small bowel obstructionBMJ Case Rep 2012 2012:piibcr0320125988. doi: 10.1136/bcr.03.2012.5988 [Google Scholar]
[10]. Thandassery RB, Sinha SK, Yadav TD, Galle AD, Vaiphei K, Singh K, Endometriosis causing small bowel obstructionTrop Gastroenterol 2013 34(3):188-91.No abstract available [Google Scholar]
[11]. Karaman K, Pala EE, Bayol U, Akman O, Olmez M, Unluoglu S, Endometriosis of the terminal ileum: a diagnostic dilemmaCase Rep Pathol 2012 2012:742035Epub 2012 Sep 11 [Google Scholar]
[12]. Ridha JR, Cassaro S, Acute small bowel obstruction secondary to ileal endometriosis: report of a caseSurg Today 2003 33(12):944-47. [Google Scholar]
[13]. Slesser AA, Sultan S, Kubba F, Sellu DP, Acute small bowel obstruction secondary to intestinal endometriosis, an elusive condition: a case reportWorld J Emerg Surg 2010 5:27doi: 10.1186/1749-7922-5-27 [Google Scholar]
[14]. Choi HK, Law WL, Ho JW, Leakage after resection and intraperitoneal anastomosis for colorectal malignancy: analysis of risk factorsDis Colon Rectum 2006 49:1719-25. [Google Scholar]
[15]. Frasson M, Granero-Castro P, Ramos Rodríguez JL, Flor-Lorente B, Braithwaite M, Martí Martínez E, ANACO Study Group. Risk factors for anastomotic leak and postoperative morbidity and mortality after elective right colectomy for cancer: results from a prospective, multicentric study of 1102 patientsInt J Colorectal Dis 2016 31(1):105-14.doi: 10.1007/s00384-015-2376-6 [Google Scholar]
[16]. Kiran RP, Murray AC, Chiuzan C, Estrada D, Forde K, Combined preoperative mechanical bowel preparation with oral antibiotics significantly reduces surgical site infection, anastomotic leak, and ileus after colorectal surgeryAnn Surg 2015 262(3):416-25.discussion 423-5. doi: 10.1097/SLA.0000000000001416 [Google Scholar]