In the present study we compare biofilm production, phospholipase and haemolytic activity of C. albicans and non-albicans species of Candida isolated from dental caries lesions of children. Here biofilm formation is a necessary prerequisite to caries formation while, haemolysin and phospholipase promote invasiveness [8–14]. The present study is an effort to know whether (or not) along with C. albicans, non-albicans species of Candida also have a role in dental caries.
Materials and Methods
Ethical aspects: The approval of the Institutional Ethics Committee of Kasturba Medical College, Mangalore, Manipal University, India has been obtained for this study. Written consent was obtained from all participants and their parents/guardians. Written permission was also obtained from school authorities to interview and obtain samples from school children during school hours.
Study design, study population, sample size: It is an in vitro cross-sectional study. With 95% confidence level and 80% power and with reference to previous studies where the prevalence of Candida in caries lesions of children was found to be around 60% [4,5], the minimum sample size comes out to be 64. So we have included in our study 100 school children with dental caries and belonging to age group 5 to 10 years. We have examined 300 school children from 4 nearby schools (2 government and 2 private) over a period of 2 months (1st July to 30th August 2012) in order to obtain 100 with dental caries and convenient sampling method was used. Children below 5 years and above 10 years of age were excluded from the study. Children without dental caries and also children with any disease other than dental caries were excluded from the study. As our study is on Candida which is a fungus, children on antibiotic prophylaxis but healthy at the time of sample collection were included in the study. A questionnaire with participant details, especially oral hygiene which included brushing and flossing habit was entered by the investigator after interviewing the children.
Cultivation and identification: All the laboratory procedures were performed in the Department of Microbiology, Kasturba Medical College, Mangalore. Oral swab samples were obtained from caries lesion by passing a sterile cotton swab. Swabs were inoculated on Sabouraud Dextrose Agar (SDA) (Hi Media, India) supplemented with 1% chloramphenicol [1]. Plates were incubated at 37°C for 48 h. After incubation, the isolates were identified by standard procedures such as gram staining, colony morphology, germ tube test, chlamydospore production and Hi-Chrome agar (Hi-Media, India) [1].
Determination of biofilm formation: Biofilm production was determined by visual methods [9,11]. Colonies from the surface of SDA plate were inoculated into a polystyrene tube (Falcon conical tube with screw cap) containing 10ml of Sabouraud-dextrose broth (SDB) supplemented with 8%+(w/v) glucose. After incubation at 37°C for 48 h, the broth in the tubes was gently aspirated. The tubes were washed with distilled water twice and then stained with 2% safranin for 10 min, then examined for the presence of an adherent layer [9,11]. Biofilm production were scored as negative (no biofilm), weak (very thin layer, just visible at the bottom), moderate (thin layer at the bottom and sides of the tube) or strong (a thick layer all over the bottom and sides of the tube) [9,11].
Assessment of haemolytic activity:Candida isolates were streaked onto SDA and incubated at 37°C for 18 h. Fungal suspension equal to McFarland 2 turbidity was prepared. 10 microliters of this suspension was spotted on human blood SDA (with 3% glucose). Plates were incubated at 37°C for 48 h [11–13]. The isolates showing a clear zone of haemolysis around the colonies were considered to be positive for haemolytic activity.
Phospholipase detection: Procedure was followed as given by Samaranayake et al., [14]. Candida isolates were grown on SDA for 18h. The growth was harvested and suspended in 0.9% NaCl and adjusted to OD 5200.5 using spectrophotometer and stored in vials. 10 microlitre of the suspension was inoculated into wells punched on the surface of egg yolk agar. Plates were incubated at 37°C for 48h. The diameter of the colonies and the diameter of the zone of opacity were measured and phospholipase activity (Pz) was calculated as follows [14]:

Statistical Analysis
Statistical analysis was performed using SPSS version 11.5. The data was analysed by Chi-Square test and Mann-Whitney U test wherever appropriate.
Results
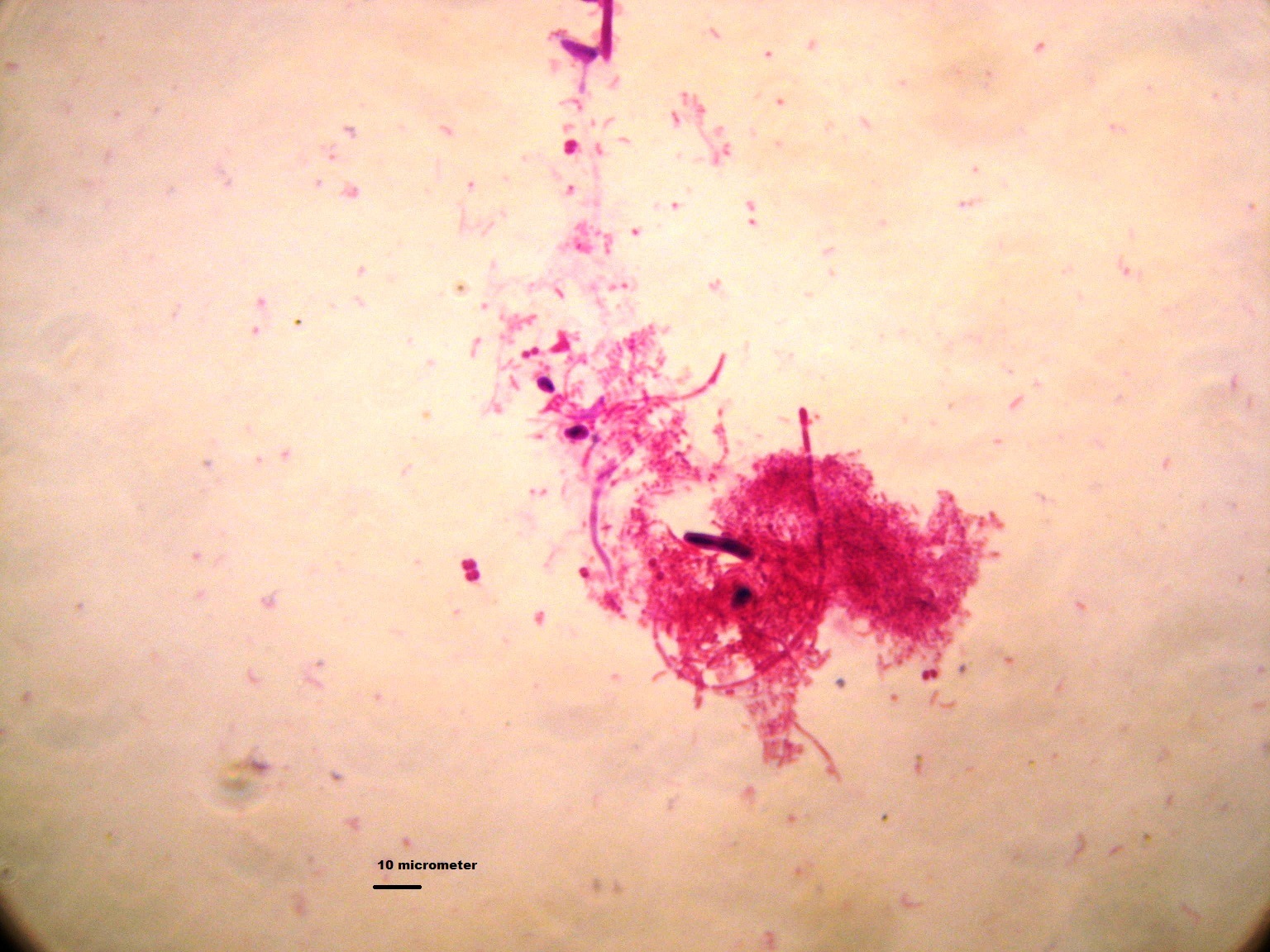
Rate of isolation: Of the 100 children, 37 (37%) were positive for Candida by smear or culture. Of these, 31 were positive by culture and 6 were positive by smear alone. Of the 31 isolates, C. albicans 21(67.74%) was most prevalent followed by C. krusei 6(19.35%), C.tropicalis 3(9.68%) and C.glabrata 1(3.23%). Gram stained smear of the oral swab from caries lesion showed that Candida produced a biofilm along with gram negative fusiform bacilli, gram negative bacilli and gram positive coccii the caries lesions as shown in [Table/Fig-1]. Of the 100 school children, 44 were female and 56 male. 56 of the 100 children under study, had the habit of brushing 2 times a day, 29 in addition brushed once more during the day and only 15 children brushed once in the morning. None of the children had the habit of flossing. Cases positive for Candida did not correlate with brushing habit (p = 0.6) or gender (p = 0.83).
Gram’s stain smear of material taken from dental caries lesion showing gram positive yeast like budding cells with pseudohyphae forming a biofilm with gram negative fusiform bacilli and gram positive cocci (1000X).
Biofilm formation: A total of 24(77.42%) out of 31 Candida isolates produced biofilm. Of these, 18(85.71%) out of 21 isolates of C.albicans, 4(66.67%) out of 6 strains of C. krusei, 2 (66.67%) out of 3 isolates of C. tropicalis produced biofilm. Of the 24 biofilm producers, 11 (45.83%) were strong or moderate biofilm producers and 13 (54.16%) were weak biofilm producers. Ten of these isolates which showed moderate or strong biofilm production were C. albicans and one was C. tropicalis. Otherwise, all the other non-albicansCandida was weak biofilm producers as shown in [Table/Fig-2].
Biofilm production and phospholipase production by various species of Candida isolated from the caries lesion in school children.
| Different species of CandidaTotal = 31 strains | Biofilm production | PhospholipaseProduction (%) |
|---|
| Weak (%) | Moderate/Strong (%) |
|---|
| C. albicans n = 21 | 8 (38) | 10 (47.6) | 10 (47.6) |
| C. krusei n = 06 | 4 (66.7) | 0 | 2 (33.4) |
| C. tropicalis n = 03 | 1 (33.4) | 1 (33.4) | 2 (66.7) |
| C. glabrata n = 01 | 0 | 0 | 1 (100) |
Haemolytic activity: Haemolytic activity was detected in all the isolates of Candida both C. albicans and non-albicans species (100%) grown on SDA human blood agar.
Phospholipase activity: Phospholipase activity was detected in 15 (48.38%) isolates of Candida. 10 (47.6%) out of 21 strains of C. albicans, 2 (33.33%) out of 6 strains of C. krusei, 2 (66.67%) out of 3 strains of C. tropicalis and 1(100%) out of 1 strain of C. glabrata showed phospholipase activity as shown in [Table/Fig-3]. We got an average Pz value of 0.77 among the strains which produced phospholipase. There was no difference in the Pz value between C. albicans and non-albicans strains. Out of 21 C. albicans isolates, 10 (47.6%) showed phospholipase activity and 18 (85.71%) produced biofilm. Of the 10 non-albicans strains, 5 (50%) showed phospholipase activity and 6 (60%) produced biofilm as shown in [Table/Fig-3].
Comparison between the various virulence factors expressed by Candida albicans and non-albicans stains of Candida isolated from the caries lesion in school children.
| Virulence factors | C. albicansn = 21 (%) | Non-albicansn = 10 (%) | *p-value |
|---|
| Biofilm production | Weak | 8 (38) | 5 (50) | 0.28 |
| Moderate/strong | 10 (47.6) | 1 (10) |
| Haemolysis | 21 (100) | 10 (100) | |
| Phospholipase | 10 (47.6) | 5 (50) | 0.73 |
* There was no statistically relevant difference between the virulence factor production by the C.albicans and non-albicans species of Candida.
Discussion
Children between 5-10 years of age were chosen because these children can definitely brush by themselves but are not old enough to brush properly or seriously, so there are more incidence of dental caries in them. As was observed, the children with dental caries did brush twice a day. As in previous studies C. albicans is the predominant isolate [3–7]. Some studies have shown a high rate of isolation 55-96% [4,5]. As we have collected samples from school children and not from patients with caries coming to the clinic with tooth ache as is usually the case in many studies, we got only 31 cases of Candida. Previous studies have shown that 63.2%-88.23% of the isolates produced biofilm [8–11]. We also have got good number of biofilm producers (77.42%). Gram stained smear of the oral swab from caries lesion showed that Candida produced a biofilm along with gram negative fusiform bacilli and gram positive cocci in the caries lesions. Past studies have shown increased adherence of C. albicans cells to epithelial cells in those isolated from patients with chronic periodontitis than in the control group [10]. Past studies show that more strains of C. albicans produce biofilm in comparison with non-albicans strains [11,15]. Another study shows that more strains of C. krusei isolated from urine samples produce biofilms in comparison with C. albicans [16]. It is a well-known fact that biofilm production by microbes predispose to dental plaque and caries formation [11]. Our study does not show much difference between the biofilm formation by C. albicans and non-albicans strains of Candida. Past studies have shown that more strains of C. albicans produce haemolysinin comparison with non-albicans strains [11,15]. In our study, all isolates showed beta haemolysis on SDA human blood agar. It is certain that numerous pathogenic microorganisms grow in the host by using haemin or haemoglobin as a source of iron [11–13]. In several studies phospholipases have been implicated in the invasion and destruction of host tissue by C. albicans [14–17]. A past study showed more strains of C. albicans produce phospholipase in comparison with non-albicans strains [15]. In a study all isolates of Candida from urine and vaginal samples producing phospholipase [17]. It is known that dental procedures like tooth extraction and restoration of caries teeth results in transient bacteraemia [18]. To prevent this dentists put their patients on antibiotic prophylaxis [18]. Cases of blood stream infection by Candida are increasing and especially the non-albicans are implicated in such cases [19,20]. In the present study, phospholipase activity was detected in 15 (48.38%) isolates of Candida from dental caries lesions. Our study does not show much difference in phospholipase production of C. albicans and non-albicans strains. In other words, our study shows that both C. albicans and non-albicans species of Candida produce these virulence factors. So, we can say that non-albicans species of Candida also are involved in caries formation.
Further studies are required with an equal number of non-albicans strains to get a statistically significant correlation between the virulence of C. albicans and non-albicans strains of Candida. Further studies are needed with a control group containing caries free children. The production of virulence factors by the various isolates of Candida from oral cavity shows that even non-albicans species of Candida probably play a role in the caries formation.
Conclusion
There was no statistically relevant difference between the virulence factor production by C. albicans and non-albicans species of Candida. In other words, our study shows that both C. albicans and non-albicans species of Candida isolated from caries lesions of the children, produce these virulence factors. So we can say that non-albicans species of Candida also are involved in caries formation.
* There was no statistically relevant difference between the virulence factor production by the C.albicans and non-albicans species of Candida.