A Study on the Correlation of Pertrochanteric Osteoporotic Fracture Severity with the Severity of Osteoporosis
Prabhnoor Singh Hayer1, Anit Kumar Samuel Deane2, Atul Agrawal3, Rajesh Maheshwari4, Anil Juyal5
1 Resident, Department of Orthopaedics, Swami Rama Himalayan University, Dehradun, Uttarakhand, India.
2 Associate Professor, Department of Orthopaedics, Swami Rama Himalayan University, Dehradun, Uttarakhand, India.
3 Associate Professor, Department of Orthopaedics, Swami Rama Himalayan University, Dehradun, Uttarakhand, India.
4 Professor and Head, Department of Orthopaedics, Swami Rama Himalayan University, Dehradun, Uttarakhand, India.
5 Professor, Department of Orthopaedics, Swami Rama Himalayan University, Dehradun, Uttarakhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prabhnoor Singh Hayer, Hayer Farms, Ladwa Road, Shahabad Markanda, Kurukshetra, Haryana-136135, India.
E-mail: prabhnoor11@yahoo.com
Introduction
Osteoporosis is a metabolic bone disease caused by progressive bone loss. It is characterized by low Bone Mineral Density (BMD) and structural deterioration of bone tissue leading to bone fragility and increased risk of fractures. When classifying a fracture, high reliability and validity are crucial for successful treatment. Furthermore, a classification system should include severity, method of treatment, and prognosis for any given fracture. Since it is known that treatment significantly influences prognosis, a classification system claiming to include both would be desirable. Since there is no such classification system, which includes both the fracture type and the osteoporosis severity, we tried to find a correlation between fracture severity and osteoporosis severity.
Aim
The aim of the study was to evaluate whether the AO/ASIF fracture classification system, which indicates the severity of fractures, has any relationship with the bone mineral status in patients with primary osteoporosis. We hypothesized that fracture severity and severity of osteoporosis should show some correlation.
Materials and Methods
An observational analytical study was conducted over a period of one year during which 49 patients were included in the study at HIMS, SRH University, Dehradun. The osteoporosis status of all the included patients with a pertrochanteric fracture was documented using a DEXA scan and T-Score (BMD) was calculated. All patients had a trivial trauma. All the fractures were classified as per AO/ASIF classification. Pearson Correlation between BMD and fracture type was calculated.
Statistical Analysis used
Data was entered on Microsoft Office Excel version 2007 and Interpretation and analysis of obtained data was done using summary statistics. Pearson Correlation between BMD and fracture type was calculated using the SPSS software version 22.0.
Results
The average age of the patients included in the study was 71.2 years and the average bone mineral density was -4.9. The correlation between BMD and fracture type was calculated and the r–values obtained was 0.180, which showed low a correlation and p-value was 0.215, which was insignificant.
Conclusion
Statistically the pertrochanteric fracture configuration as per AO Classification does not correlate with the osteoporosis severity of the patient.
AO/ASIF, Bone disease, Pertrochanteric fractures
Introduction
Osteoporosis is a metabolic bone disease caused by progressive bone loss. It is characterized by low Bone Mineral Density (BMD) and structural deterioration of bone tissue leading to bone fragility and increased risk of fractures. It is considered as a “silent thief” that generally does not become clinically apparent until a fracture occurs. The most common fractures in people with osteoporosis occur in bones that are subject to weight bearing strain (such as the spine, pelvis and hips) or that take the stress when a person braces himself or herself when falling (such as the wrists, forearms and upper arms) [1].
The symptoms of osteoporosis are from the fractures it causes. These can be micro-fractures or fragility fractures from trivial trauma. Multiple vertebral fractures lead to a stooped posture, loss of height, and chronic pain with resultant reduction in mobility of the patient. Hip fracture usually requires prompt surgery, as serious risks such as DVT and pulmonary embolism, and increased mortality are associated with it [2].
Annually osteoporosis causes more than 8.9 million fractures worldwide [1]. In a study on Indian women aged 30-60 years from low income groups, BMD at all the skeletal sites were much lower with a high prevalence of osteopenia (52%) and osteoporosis (29%) when compared with values of developed countries and it was attributed to inadequate nutrition [2].
Osteoporosis can be classified as primary and secondary. Primary osteoporosis is defined as osteoporosis in which there is no underlying cause. Secondary osteoporosis is one in which there is definitive underlying cause [2].
Diagnosis of osteoporosis can be suspected on the strength of a plain X-Ray evaluation but the objective and internationally accepted method of diagnosing is measurement of BMD by Double Energy X-Ray Absorbtiometry (DEXA) [3]. Irrespective of fracture type and bone density measurement site, the prognostic implications of diminished BMD are well characterized and there is a consistent doubling of fracture risk for each SD reduction of BMD [4].
BMD is a surrogate biomarker for bone strength; a decrease in BMD is associated with increase in fracture risk, while, conversely an increase in BMD is associated with a reduction in fracture risk.
The classification of fractures represents a mainstay in orthopaedic trauma surgery. Numerous classification systems (e.g. Boyd and Griffin, Evans, AO/ASIF) have been proposed so far and are more or less successfully used in clinical settings [5,6]. When classifying a fracture, high reliability and validity are crucial for successful treatment. Furthermore, a classification system should include severity, method of treatment, and prognosis for any given fracture [7,8]. The treatment of a fracture should include the management of the fracture and also the cause of the fracture, which is osteoporosis in most of the pertrochanteric fractures. Since it is known that treatment significantly influences prognosis, a classification system claiming to include both would be desirable.
However, none of the classification systems currently used takes the patient’s bone status into account. In this study we analysed fractures of proximal femur in patients with osteoporosis.
Aim
The aim of the study was to evaluate whether the AO/ASIF fracture classification system, which indicates the severity of fractures, has any relationship with the bone mineral status in patients with primary osteoporosis.
Materials and Methods
The present study was conducted in the Department of Orthopaedics at Himalayan Institute of Medical Sciences, Swami Ram Nagar, Dehradun from January 2014 to December 2014 after taking clearance from the ethical committee. Patients above 45 years of age presenting in Orthopaedic OPD and Emergency of HIMS having pertrochanteric fracture of femur with underlying primary osteoporosis, were included in the study.
Selection of Subject
Inclusion Criteria: 1) Men and women above 45 year of age; 2) BMD documented osteoporosis (T-score < or = -2.5 at femoral neck or at AP Spine); 3) Patients presenting within 3 weeks of a pertrochanteric fracture.
Exclusion Criteria: 1) Non-Osteoporotic pathological fractures; 2) Chronic use of glucocorticoids; 3) Conditions associated with low bone density (e.g., Diabetes Mellitus, Rheumatoid arthritis, Cystic fibrosis, Parkinson’s disease etc.)
Study Protocol: 1) Radiographic diagnosis of a pertrochanteric fracture was made on Plain x-ray films in AP and Lateral views of the affected hip with proximal femur; 2) Diagnosis of Osteoporosis was made on WHO criteria through BMD by means of a DEXA scan using the Lunar Prodigy Advance DXA System manufactured by GE Healthcare; 3) All the fractures were classified as per the AO/ASIF Classification and all the data was recorded in an excel file [9].
Results
A total number of 63 patients presented to our hospital with hip fracture out of which 49 met the inclusion criteria and results were calculated on 49 patients.
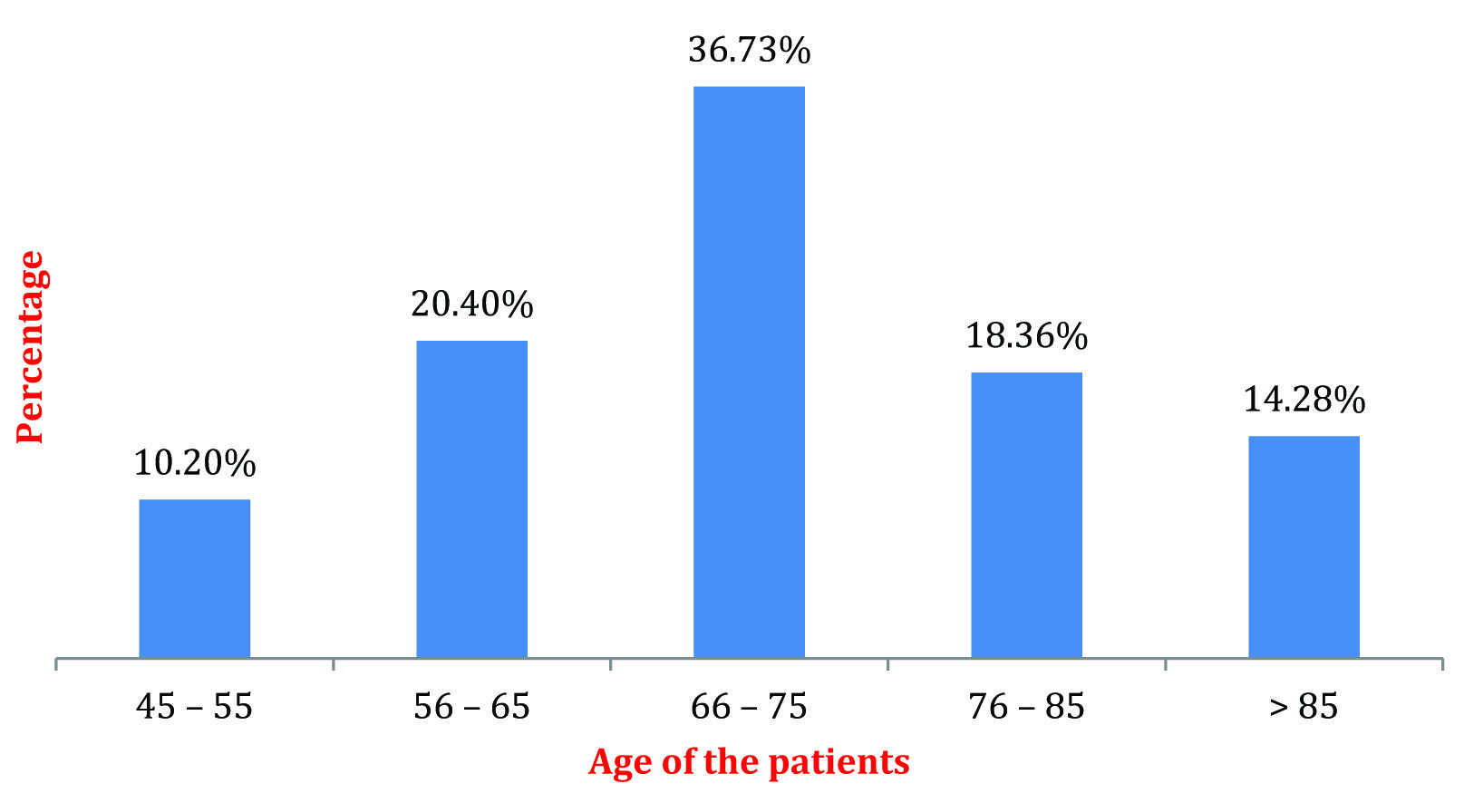
Age Distribution: The average age of the patients included in the study was 71.2 years and the maximum patients i.e., 36.73% were between 66 to 75 years of age as depicted in [Table/Fig-1].
Age-wise distribution of subjects.
Gender: Out of 49 patients, 22 (44.89%) were males and 27 (55.10%) were females.
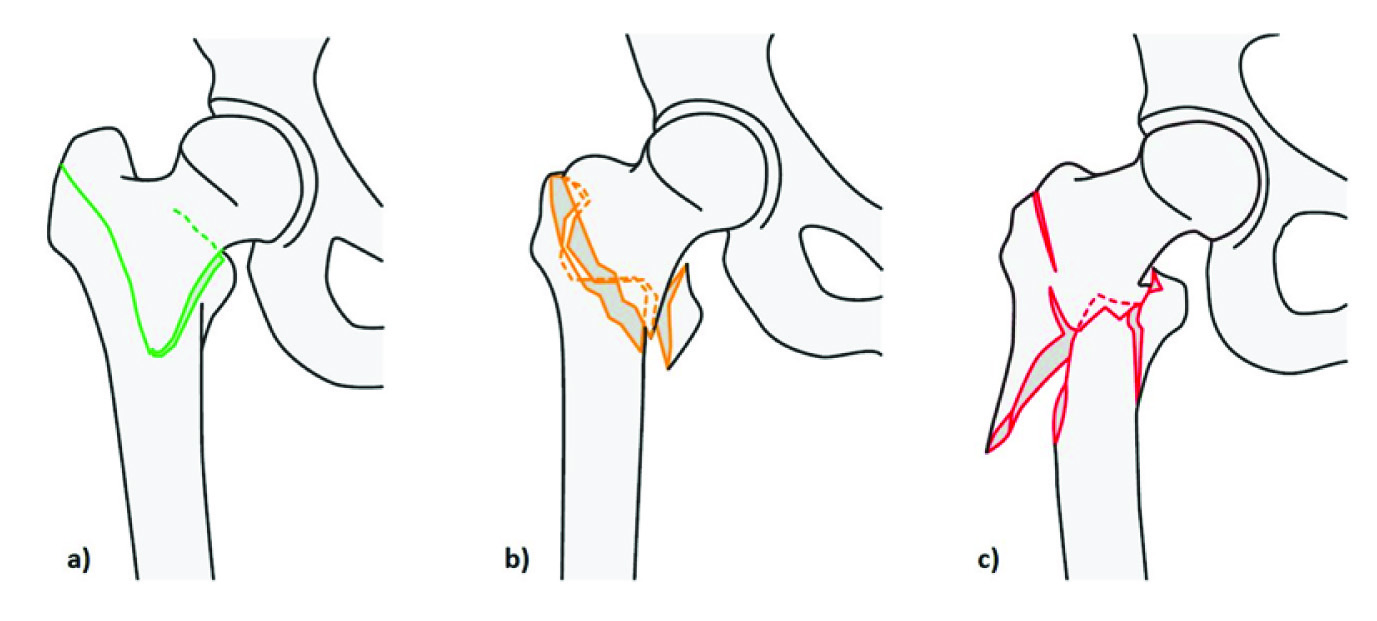
Fracture Type (AO/ASIF Classification): [Table/Fig-2] shows the AO/ASIF classification of pertrochanteric fracture: a) AO 31-A1; b) AO 31-A2; and c) AO 31-A3 [9]. The maximum number of patients had an AO 31-A2 type of a fracture i.e., 51.02%.
AO/ASIF Classification [9] a) AO 31 – A1, b) AO 31 – A2 and c) AO 31 – A3.
Bone Mineral Densitometry: The T-Score i.e. the number of standard deviations above or below the mean for a healthy 30-year-old adult of the same sex and ethnicity as the patient was calculated by means of a DEXA scan. The average BMD of the patients included in the study was -4.9.
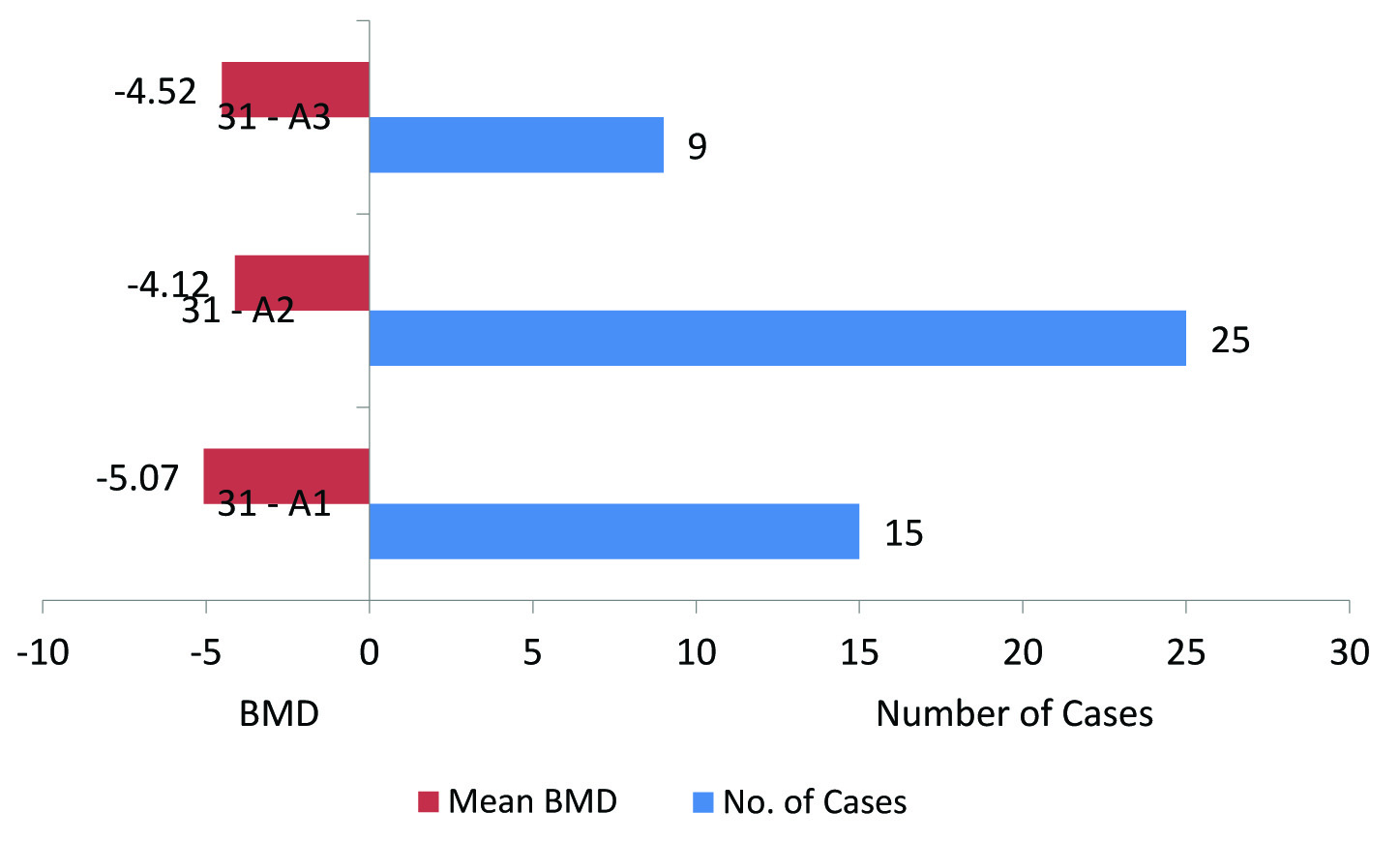
[Table/Fig-3] depicts the number of cases in each group according to the AO classification, 15 patients were having an AO 31-A1 type of fracture and the mean BMD of patients in this group was -5.07. The mean BMD of patients with AO 31-A2 type of fracture was -4.12 and total patients in this group were 25 and the third group with AO 31-A3 type of fracture had 9 patients with an average BMD of -4.52 [Table/Fig-4].
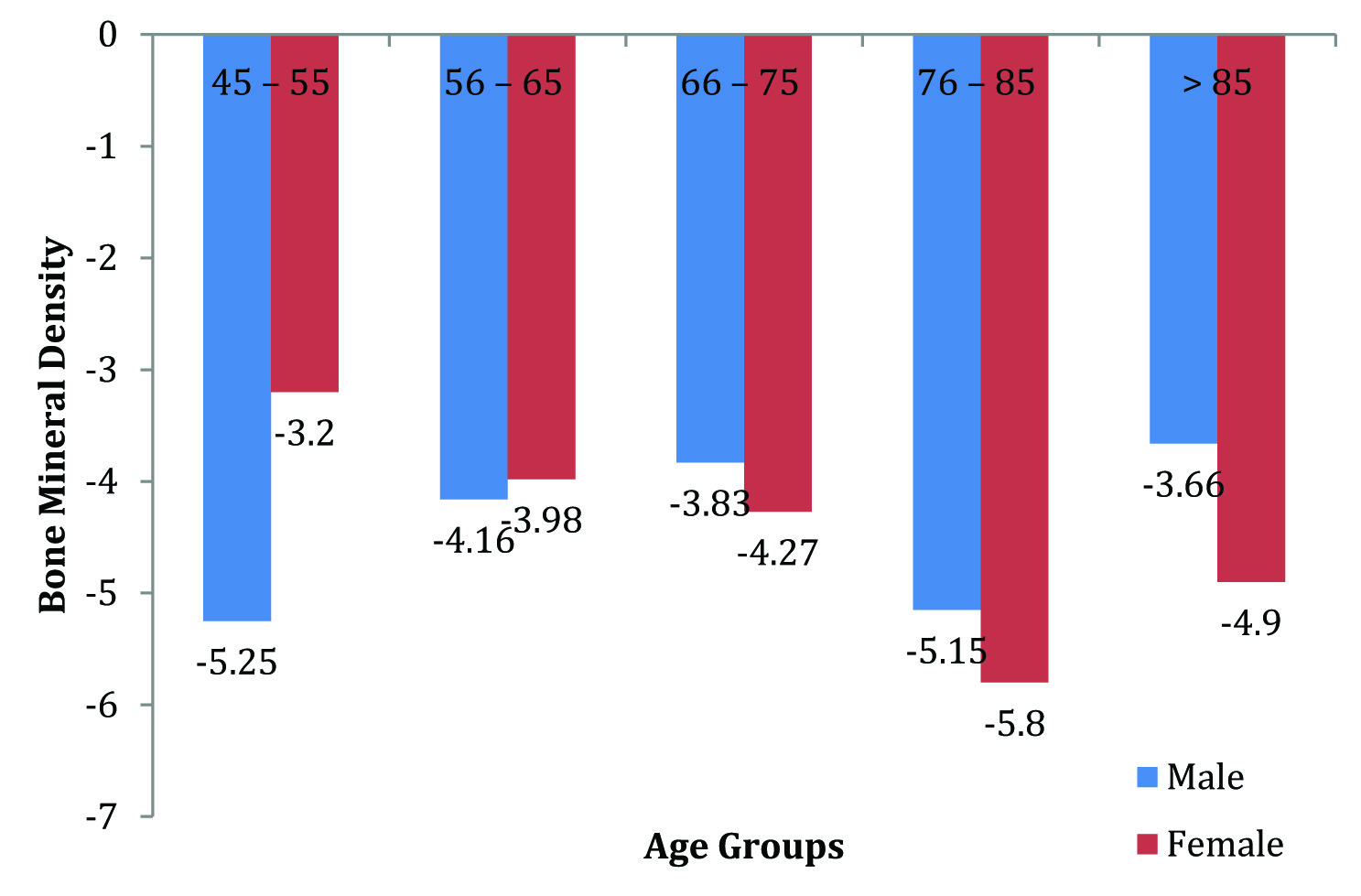
Graph showing average bone mineral density in different age groups in males and females.
Graph showing average bone mineral density in different type of fracture pattern and number of patients in each fracture pattern group.
The correlation between bone mineral densitometry and fracture type was calculated using the Pearson Correlation. The r-value obtained was. 180, which shows very low correlation, and the p-value was. 215, which was insignificant [Table/Fig-5].
Correlations between BMD and Fracture Type.
| | BMD | Fracture Type |
|---|
| BMD | Pearson Correlation | 1 | 0.180 |
| Sig. (2-tailed) | | 0.215 |
| N | 49 | 49 |
| Fracture Type | Pearson Correlation | 0.180 | 1 |
| Sig. (2-tailed) | 0.215 | |
| N | 49 | 49 |
Discussion
Fracture classification in orthopaedic trauma surgery is fundamental for successful treatment of patients. However, not only the fracture pattern should be analysed when a fracture is classified, but also the bone tissue itself as the main matrix for fracture repair and bone healing. Therefore we hypothesized that classification should have a relationship with the fracture severity. AO/OTA classification is the most widely and internationally accepted classification system used for all the fractures of the body. It’s alphanumerical value of fracture types can be very well understood by any orthopaedic surgeon and one can have an idea about the configuration of a fracture and the treatment can be planned accordingly. The classification system just gives the details about the configuration of the fracture and does not include the bone matrix status. The AO classification is based on the severity/complexity of a fracture i.e. Type 1 fractures are simple fractures and type 3 are complex/severe fractures [9].
The mean age of the patients included in the study was 71.2 years, which was similar to study by Kim TY et al., they had 3 groups of patients with an intertrochanteric fracture with a mean age of 75 years in Group A, 75.3 in Group B and 78.1 in Group C. They included all the patients with a T-score of less then -2.5, The mean BMD in Group A of their study was -3.2, in Group B -2.8 and -3.3 in Group C. In our study the average T-score at femoral neck of the non-fractured side was -4.9, which showed that Osteoporosis was markedly more in our patients [10].
Various studies have stated that the severity of Osteoporosis increases with age, but in our study the most osteoporotic patient was a male of 48 years with a BMD of -8.2. Female preponderance was found probably due to postmenopausal osteoporosis [1].
Hoesel LM et al., studied the impact of osteoporosis on the classification of hip and wrist fractures and had stated the need of an osteoporosis-adapted fracture classification. They also found that patients with osteoporosis sustain more severe and complex fractures, however our study could not show any correlation between the osteoporosis and the fracture type at the hip region [11].
Pertrochanteric fractures, vertebral fractures and distal radius fractures are the most common fractures caused due to osteoporosis, However, there are no studies which show that the severity of a fracture depends upon the severity of the osteoporosis but it is assumed by all the Orthopaedic surgeons that a weak bone i.e., with severe Osteoporosis will have a more severe fracture pattern. We tried to find a statistical correlation between the Osteoporotic severity and fracture type but our results were not similar to the assumptions which all the Orthopaedic surgeons have about Osteoporotic fractures.
Conclusion
We were not able to demonstrate any correlation in cases of pertrochanteric fractures between the fracture type and BMD of an osteoporotic patient statistically. We had hypothesized that the severity of the fracture increases with increasing osteoporosis severity, however we were not able to affirm our hypothesis statistically. We therefore suggest that a study incorporating more osteoporotic fracture regions, as done by Hoesel LM, and with a larger sample size be conducted to better assess the correlation between the severity of osteoporotic fractures and the severity of osteoporosis.
[1]. Johnell O, Kanis JA, An estimate of the worldwide prevalence and disability associated with osteoporotic fracturesOsteoporos Int 2006 17:1726-32. [Google Scholar]
[2]. Shatrugna V, Kulkarni B, Kumar PA, Bone status of Indian women from a low-income group and its relationship to the nutritional statusOsteoporos Int 2005 16:1827-35. [Google Scholar]
[3]. Salamat MR, Rostampour N, Zofaghari J, Hoseyni-Panah H, Javdan M, Comparison of Singh index accuracy and dual energy X-ray absorptiometry bone mineral density measurement for evaluating osteoporosisIran J Radiat Res 2010 8(2):123-28. [Google Scholar]
[4]. Lewiecki ME, Intravenous Zoledronic acid for the treatment of osteoporosis: The evidence of its therapeutic effectCore Evidence 2009 4:13-23. [Google Scholar]
[5]. Bernstein J, Monaghan BA, Silber JS, DeLong WG, Taxonomy and treatment – a classification of fracture classificationsJ Bone Joint Surg Br 1997 79:706-07. [Google Scholar]
[6]. Audige L, Bhandari M, Kellam J, How reliable are reliability studies of fracture classifications? A systematic review of their methodologiesActa Orthop Scand 2004 75:184-94. [Google Scholar]
[7]. Burstein AH, Fracture classification systems: do they work and are they useful?J Bone Joint Surg Am 1993 75:1743-44. [Google Scholar]
[8]. Martin JS, Marsh JL, Current classification of fractures. Rationale and utilityRadiol Clin North Am 1997 35:491-506. [Google Scholar]
[9]. Rüedi TP, Buckley RE, Moran CG, “Fracture Classification.” AO Principles of Fracture Management 2007 StuttgartThieme [Google Scholar]
[10]. Kim TY, Ha YC, Kang BJ, Lee YK, Koo KH, Does early administration of bisphosphonate affect fracture healing in patients with intertrochantric fracture?J Bone Joint Surg (Br) 2012 94B:956-60. [Google Scholar]
[11]. Hoesel LM, Pausch M, Schnettler R, Heiss C, The impact of osteoporosis on the classification of hip and wrist fracturesMed Sci Monit 2008 14(3):HY1-8. [Google Scholar]