Blue Cell Tumour at Unusual Site: Retropritoneal Ewings Sarcoma
Anita P Javalgi1, Mahesh H Karigoudar2, Katyayani Palur3
1 Assistant Professor, Department of Pathology, Shri B M Patil Medical College, Sholapur Road Bijapur, Karnataka, India.
2 Professor, Department of Pathology, Shri B M Patil Medical College, Sholapur Road Bijapur, Karnataka, India.
3 Post Graduate, Department of Pathology, Shri B M Patil Medical College, Sholapur Road Bijapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anita P Javalgi, Assistant Professor, Department of Pathology, Bldeu’s Shri B M Patil Medical College, Sholapur Road Bijapur, Karnataka-586103, India.
E-mail: anitajawalgi@gmail.com
Ewing’s sarcoma is a highly malignant tumour of osseous or non-osseous origin, tremed as extra-skeletal Ewings sarcoma if arising from soft tissue. It is rare occurrence tumor most commonly occurring in paravertebral area, chest wall, head & neck and retroperitoneum. Reporting an interesting case of retroperitoneal Ewing’s sarcoma in 39 years old female. Patient had complains of abdominal discomfort & vague pain since 2 months, following weakness in lower limb and loss of weight. On detail history and examination she was further referred to detail pathological and radiological investigations. Haematological profile, renal function test and liver function test were in normal limits. USG abdomen was normal, MRI showed a mass in pelvis retroperitoneum measuring 10x10cms, bilateral ovaries and tubes were normal. Because of retroperitoneal nature of tumor and suspicion of uterine sarcoma, laparotomy was performed. The large retroperitoneal mass adherent to posterior of uterus was excised and send for histopathological diagnosis. On gross and microscopy examination the diagnosis of blue cell tumor with PAS positivity, possibility of extraskeletal Ewing’s sarcoma/primitive neuro-ectodermal tumor was made which was further confirmed by immunohistochemistry, positive for S100, Vementin and CD99 and negative for desmin and CK. Confirmed diagnosis help in accurate management and improves survival rate.
Ewings sarcoma, Retroperitoneum, CD99
Case Report
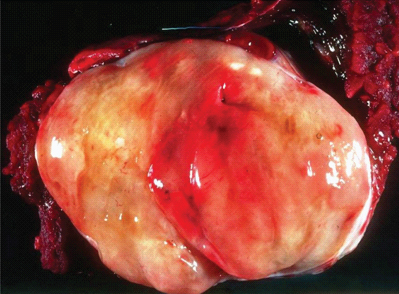
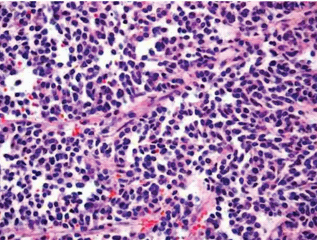
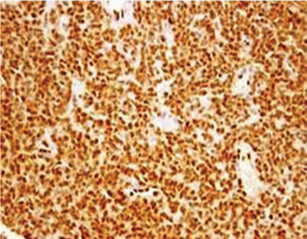
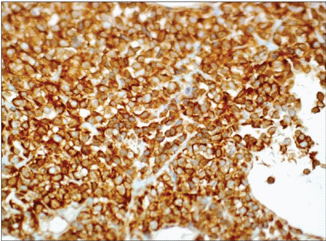
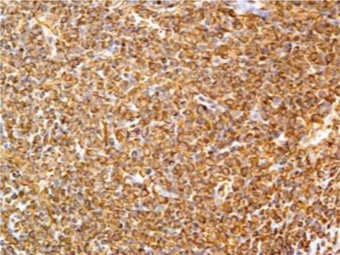
A 39-year-old female patient presented with complaints of abdominal discomfort & vague pain since 2 months, following weakness in lower limb and loss of weight. On investigation, the haematological profile, renal function test and liver function test were within normal limits. USG abdomen showed no abnormalities. MRI abdomen and pelvis, however, revealed a mass in the pelvic retroperitoneum measuring 10x10 cm. Bilateral ovaries and tubes were normal. As the mass was retroperitoneal and clinically suspected to be uterine sarcoma, laparotomy was performed. Intraoperatively, the mass was adherent to the posterior surface of the uterus. The mass was excised and send for histopathology. On gross [Table/Fig-1] and microscopic examination [Table/Fig-2], the diagnosis of small round blue cell tumour, with a possibility of extraskeletal Ewing’s sarcoma/ primitive neuro-ectodermal tumour with PAS positivity was made. The diagnosis was further confirmed by immunohistochemistry. The tumour was positive for S100 [Table/Fig-3], Vimentin [Table/Fig-4] and CD99 [Table/Fig-5] and negative for desmin and CK. Post surgery patient was on Chemotherapy and doing alright in first cycle later we lost patient as she didnot turn up for further follow-up.
Gross, mass 10x10cms smooth surfaced pale yellow tumor.
H&E 100X small round cells arranged in trabecule and roisettes.
Discussion
The Ewing Family of Tumours (EFT) is a group of sarcomas that share a rearrangement of the EWSR1 gene on 22q12. Ewing’s sarcoma (EWS)/ Peripheral Neuro-Ectodermal Tumour (PNET) is among the better known entities in the EFTs. It is a malignant small round blue cell tumour with varying degrees of neuro-ectodermal differentiation [1,2]. EWS predominantly presents in the paediatric age group and is uncommon in adults older than 30 years [3]. It commonly occurs in the bone and soft tissue. EWS arising from structures other than bone is quite rare and is termed as extra-skeletal EWS (ES-EWS) [4]. ES-EWS can occur in the paravertebral area, chest wall, head & neck and retroperitoneum [1,4,5]. Ewing’s sarcoma (EWS) occurs more commonly in the paediatric population compared to adults. Majority of the cases of EWS in the paediatric population arise from the bone while >50% of the cases in adults arise from soft tissue. EWS arising from the trunk account for 14% of the cases, 14% in intraabdominal tissues or retroperitoneum, 8% in the viscera and 21% from other sites. Extra-skeletal Ewing’s sarcoma (ES-EWS) is a rare entity and presents as a soft tissue mass. Overall the occurrence of ES-EWS is uncommon [2,6].
Patients with abdominal/retroperitoneal ES-EWS present with variable clinical manifestations depending on the size and site of the tumour and the extent of invasion into adjacent structures. These tumours are rapidly enlarging masses most commonly presenting with compression symptoms and abdominal pain or discomfort. On examination, a mass may be palpable per abdomen [1,3].
Routinely, the diagnosis is based on imaging modalities and MRI is often the preferred imaging study to assess the extent of involvement of the soft tissue [3]. Early detection is difficult as the retroperitoneal space is expandable and can obscure the details of these masses. There are no specific findings to differentiate abdominal/retroperitoneal EWS from other abdominal or retroperitoneal tumours [2]. Histomorphology, however, is essential for the definitive diagnosis of these tumours [4,7].
Grossly these are lobulated soft tissue tumours with incomplete capsule and infiltrative margins ranging from 3 cm to 40 cm in size. Sections are yellow - gray in colour, soft with fish-like haemorrhagic necrosis of the tumour tissue which maybe be mistaken for pus by surgeons [1].
On histopathology, ES-EWS appears similar to the classical EWS. It shows a uniform population of closely packed small round cells, arranged in sheets with round nuclei, indistinct nucleoli, high nuclear-cytoplasmic ratio and scant vacuolated cytoplasm due to the presence of glycogen which is responsible for the Periodic Acid Schiff (PAS) positivity [2,4]. Homer-Wright rosettes may or may not be present depending on the degree of neuroectodermal differentiation [1].
Small round blue cell tumours are a group of malignant neoplasms characterised by the presence of sheets of small round blue malignant cells with scant cytoplasm giving the appearance of a blue tumour. As the histopathological appearance of small round blue cells has an ever expanding list of differentials, immunohistochemistry (IHC) is often mandatory to arrive at the final diagnosis. The common differential diagnosis to be considered in the case of retroperitoneal EWS can be categorised into the following based on the cell lineage:
1. Epithelial tumours including small cell carcinomas;
2. Mesenchymal tumours including Desmoplastic Small Round Cell Tumours (DSRCT) and Rhabdomyosarcomas (RMS) and
3. Other tumours such as malignant melanomas and lymphomas [4].
Small cell carcinomas are usually keratin positive, CD 99 negative and positive for neuroendocrine markers. DSRCTs are positive for desmin, keratin and EMA. RMS is positive for desmin and myoG and negative for keratin. Lymphomas are positive for CD45 with keratin and desmin negativity. Melanomas are also negative for keratin and desmin but positive for S100 and HMB45 [4,8,9].
Mesothelioma may also be considered as a differential diagnosis for abdominal EWS in which case a strong positivity for mesothelial markers is seen; mesothelin and calretinin. Markers useful to distinguish ES-EWS from angiomyolipoma include HMB45, CD31, CD34, AFP and Factor VIIIRA which are all negative in case of EWS [9].
In case of EWS, IHC reveals a strong, diffuse, membranous positivity with CD99. Vimentin, NSE and S-100 are also frequently expressed [1]. Our case was also positive for PAS, CD99, Vimentin and S-100.
Molecular analysis of these tumours by RT-PCR and FISH demonstrate chromosomal rearrangements involving t(11; 22) (q24; q12). These rearrangements involve fusion of the EWS gene on chromosome 22 to FLI, ERG or ETV1 gene members of the ETS transcription factor family. This results in EWS/FLI21, EWS/ ERG or EWS/ETV1 fusion genes [1].
Conclusion
Ewing’s sarcoma arising from the abdominal cavity/retroperitoneum is relatively rare. These tumours often grow rapidly compressing adjacent structures with widespread metastasis by the time the patients present leading to poorer prognosis. Imaging is the primary means of early detection of these tumours and histopathology is crucial for confirmation of the diagnosis. A definitive diagnosis by means of histopathology aids in the appropriate management and improves survival rate.
[1]. Zhang Z, Yu H, Shi Y, Shi H, A case report on retroperitoneal PNET/EWSCase Reports in Clinical Medicine 2013 2:366-69. [Google Scholar]
[2]. Ulusan S, Koc Z, Canpolat ET, Colakoglu T, Radiological Findings of Primary Retroperitoneal Ewing SarcomaActa Radiol 2007 7:814-18. [Google Scholar]
[3]. Naru T, Nawaz FH, Rizvi J, Juvenile Ewing Sarcoma Presenting as a Pelvic MassJCPSP 2007 17:53-54. [Google Scholar]
[4]. Gill M, Gupta P, Pawar P, Sen R, Malignant small round cell tumour masquerading as mesothelioma of peritoneum: diagnosed on immunohistochemistryInternational J. of Healthcare and Biomedical Research 2014 2:83-86. [Google Scholar]
[5]. Liaqat N, Dar SH, Iqbal A, Khan FA, Sultan N, Extraskeletal Ewing Sarcoma involving abdominal wall in a neonateJ Ped Surg Case Reports 2014 2:23-4. [Google Scholar]
[6]. Ozaki Y, Miura Y, Koganemaru S, Suyama K, Inoshita N, Fujii T, Ewing sarcoma of the liver with multilocular cystic mass formation: a case reportBMC Cancer 2015 15:16 [Google Scholar]
[7]. Sofi AA, Thekdi AD, Nawras A, EUS-FNA for the Diagnosis of Retroperitoneal Primitive Neuroectodermal TumourHindawi Publishing Corporation Diagnostic and Therapeutic Endoscopy 2011 2011:198029:3pages [Google Scholar]
[8]. Bahrami A, Truong LD, Ro JY, Undifferentiated Tumour - True Identity by ImmunohistochemistryArch Pathol Lab Med 2008 132:326-48. [Google Scholar]
[9]. Tulunay O, Beduk Y, Yalcinkaya A, Karaboga R, A Retroperitoneal/omental tumour with characteristics of Ewing’s sarcoma/peripheral primitive neuroectodermal tumour (EWS/pPNET) and desmoplastic small round cell tumour (DSRCT) with unique pathologic and immunohistochemical features, presented as a renal tumourThe Internet Journal of Pathology 2008 8(1):1-3. [Google Scholar]