Strangulated Groin Hernia Repair: A New Approach for All
Bapurapu Raja Ram1, Vallabhdas Srinivas Goud2, Dodda Ramesh Kumar3, Bande Karunakar Reddy4, Kumara Swamy Boda5, Venkanna Madipeddi6
1 Associate Professor, Deparment of General Surgery, Mahathma Gandhi Memorial Hospital, Kakatiya Medical College, Warangal, Talangana, India.
2 Associate Professor, Deparment of General Surgery, Mahathma Gandhi Memorial Hospital, Kakatiya Medical College, Warangal, Talangana, India.
3 Professor, Deparment of General Surgery, Mahathma Gandhi Memorial Hospital, Kakatiya Medical College, Warangal, Talangana, India.
4 Professor, Deparment of General Surgery, Mahathma Gandhi Memorial Hospital, Kakatiya Medical College, Warangal, Talangana, India.
5 Assistant Professor, Deparment of General Surgery, Mahathma Gandhi Memorial Hospital, Kakatiya Medical College, Warangal, Talangana, India.
6 Assistant Professor, Deparment of General Surgery, Mahathma Gandhi Memorial Hospital, Kakatiya Medical College, Warangal, Talangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bapurapu Raja Ram, H.No: 2-2-23/B2 Heritage Residensy, Behind Rang restaurent, Naim nagar, Vidyaranyapuri, Hanamkonda, Warangal-506001, Talangana State, India.
E-mail: paulrajaram@yahoo.com
Introduction
The available classical approaches for Groin hernia are multiple. The change of approach with change of incision is needed with these approaches when the bowel is gangrenous.
Aim
To evaluate the efficacy and safety of a new approach for all strangulated groin hernias (inguinal, femoral and obturator), in terms of change of approach/complications.
Materials and Methods
It was conducted in surgical unit-2 of MGM Hospital, Kakatiya Medical College Warangal, Telangana State, India, from Nov 2000 to Oct 2010. Total 52 patients operated with classical approach were compared with 52 patients operated present new approach. All the cases (52+52) were with gangrenous bowel which required resection and end to end anastomosis of bowel. All the cases (52+52) were managed with mesh repair and the results were analysed.
Results
In classical approach: Three cases required laparotomy (5.7%). Twelve cases required change of approach with change of incision (23%). Eight cases developed wound infection after mesh repair (15%). Four cases required removal of mesh (7.6%). Two Cases developed recurrence (3.8%). In present new approach: No laparotomy (0%), no change of incision (0%), no removal of mesh (0%) and no recurrence(0%). Only 2 cases (3.8%) developed wound infection at lateral part of incision ie. p<0.05.
Conclusion
This new approach for all - gives a best approach for strangulated groin hernias as it is easy to follow. It obviates the change of incision and need for a laparotomy. It further retains normal anatomy, prevents contamination of the inguinal canal and permits a mesh repair leading to decreasing the chances of recurrence.
Femoral hernia, Gangrenous bowel, Inguinal hernia, One skin incision, Strangulation, Window
Introduction
Groin hernias are the most common type of external hernias. Groin hernias include the direct and indirect inguinal, femoral and obturator hernias. While inguinal hernias are the commonest of the groin hernias, obturator hernia is the most uncommon type. Femoral hernias are relatively less common, but present frequently with strangulation. Strangulated inguinal hernia can be managed in a routine fashion. Three Classical approaches are described for an open repair of femoral hernia [1]. Low (Lockwood’s), inguinal (Lotheissen’s) and high (Mc Evedy’s). Each approach describes a separate incision and dissection to access the femoral sac.
Lockwood’s infra-inguinal approach is the preferred method for elective repair of uncomplicated femoral hernia. The approach is through an oblique incision 1cm below and parallel to the inguinal ligament. This approach offers little scope for resection and anastomosis of gangrenous bowel, and a separate laparotomy is indicated for the procedure [2].
Lotheissen’s trans-inguinal approach gives ample room for resection anastomosis of the gangrenous bowel, but the disadvantage is that the posterior wall of the inguinal canal is disrupted, which has to be repaired. In view of the contamination with the gangrenous bowel, a mesh repair is not possible. Hence the recurrence rate is high [3]. Also, the incidence of false recurrence in the form of a direct hernia is high with this procedure [4,5].
Mc Evedy’s high approach is a pararectal approach through a vertical incision. It gives a good exposure of the abdominal contents and the femoral hernias as well [6], but it weakens the abdominal musculature leading to a direct hernia as a complication. A modification of Mc Evedy’s procedure using a skin crease incision instead of a vertical incision was proposed by Mouzas/Diggory [2]. An alternative, a unilateral Pfannensteil incision which can be extended to make it a complete Pfannensteil. The advantage of this procedure is that, if resection of bowel is required, there will be ample space to do so. The disadvantage with this procedure is that if infection occurs, an incisional hernia may develop later, which is very difficult to repair.
Many times, the femoral hernia is wrongly diagnosed preoperatively as an inguinal hernia, because the tendency of femoral hernias to move upwards to a position above the inguinal ligament. The correct diagnosis often made only at the time of operation. The decision as to which approach is to be adopted depends upon the viability of the bowel. Hence it is very difficult to decide particular approach before surgery. To avoid all these uncertainties, we adopted an easy approach to deal all the strangulated groin hernias.
Materials and Methods
This study was conducted at Mahathma Gandhi Memorial Hospital, Kakatiya Medical College Warangal, Telangana State, India from November 2000 to October 2010, After taking the Institutional ethical committee approval. The present study was conducted to compare the Classical approach (Multiple) with the present new approach (Single). In both the groups, 52 patients were included after taking patient consent. A retrospective data of 52 patients which were operated with classical approach [1] were included in one group and it was compared with 52 patients operated with present new approach with right sided obstructed groin hernias (Inguinal and femoral). Inclusion criteria for this study were the patients with obstructed groin hernia managed with either of the approaches. Exclusion criteria were the patients without obstructed hernia and without mesh repair. Usually in a case of strangulated hernia mesh repair is avoided after resection anastomosis of bowel. Here we repaired with mesh after saline wash in both the groups. All the cases were followed up for six months.
Present New Approach (Window to Window One Skin Incision Approach)
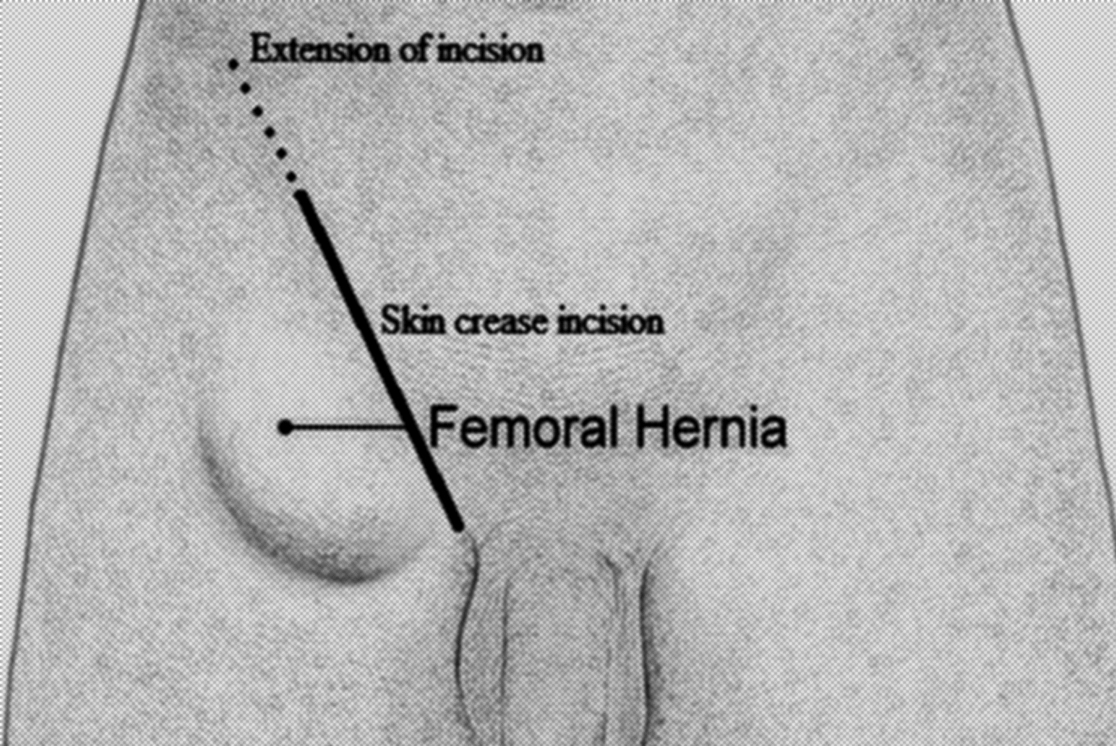
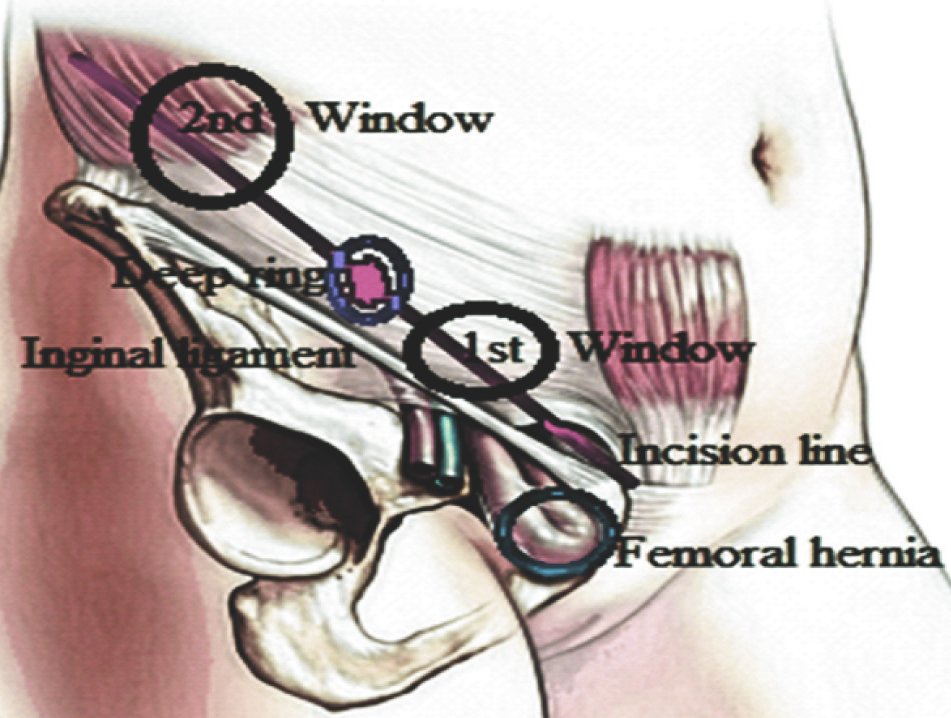
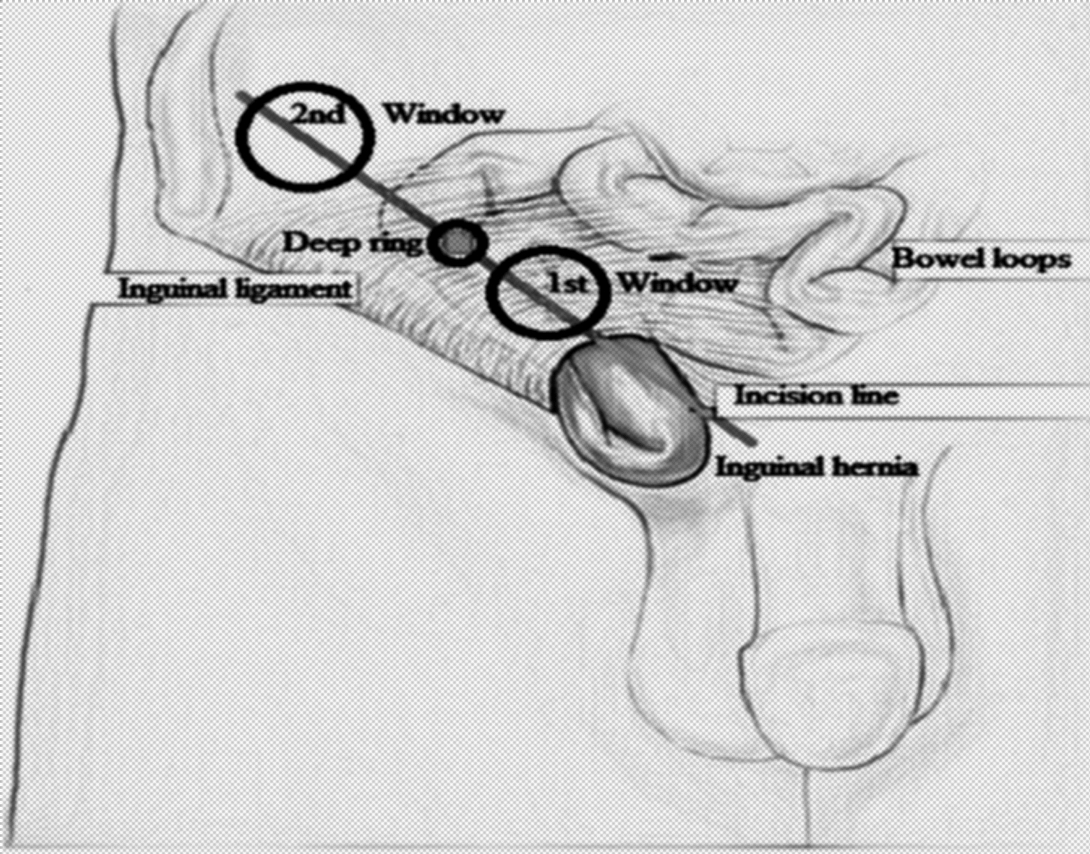
An inguinal skin crease groin incision was taken and the inguinal canal opened [Table/Fig-1]. The intraoperative diagnosis of groin hernia was confirmed. If it happens to be inguinal, the sac of the inguinal hernia is identified, dissected and traced upto defect of herniation (first window) [Table/Fig-2]. If it happened to be femoral hernia, the sac with contents were delivered from femoral canal and traced upto the defect of herniation in posterior wall of inguinal canal (first window) [Table/Fig-3]. If the bowel was found to be gangrenous and requires resection and anastomosis in either of the case, the elective inguinal incision can be extended laterally little beyond the Mc Burney’s point. The extension of incision was done by dividing only skin and external oblique. The internal oblique and transversus abdominis are split open as that of gridiron incison (Second Window) [Table/Fig-2,3]. The gangrenous bowel can be reduced from the first window and delivered through the second window. Here, through the second window, the resection and anastomosis of the bowel can be done comfortably, and the bowel is placed back in the peritoneal cavity. Finally, the mesh repair of the inguinal hernia can be done with Lichtenstein’s technique and femoral canal closed with plugging of rolled out piece of mesh. If the bowel was found to be healthy it will be managed with classical mesh repair of surgeons choice.
One skin incision approach.
Window to window one skin incision approach for strangulated femoral hernia.
Window to window one skin approach for strangulated inguinal hernia.
Results
Total 52 patients who were operated with the classical approach are compared with 52 patients who were operated with present approach in [Table/Fig-4,5]. In the classical approach, out of 52 cases 42 cases were strangulated inguinal hernias and 10 cases were strangulated femoral hernias. Three cases required laparotomy (5.7%). Twelve cases required change of approach with change of incision (23%). Eight cases developed wound infection after mesh repair (15%). Four cases required removal of mesh (7.6%). Two cases developed recurrence (3.8%). Drain placement was compromised.
Showing differences between Classical and Present Approach.
| S. No. | Classical Approach (Multiple) | Present Approach (Single) |
|---|
| 1. | Change of approach with change of incisionis required, if gangrenous bowel encountered. | No change required. |
| 2. | Unnecessary division of muscles. | Retains normal anatomy. |
| 3. | Each approach deals only specific situation.Ex: Elective, emergency, inguinal, femoral. | Deals with all. |
| 4. | Resection and end to anastomosis is done at the repair site. | Done at different window away from repair site. |
| 5. | Mesh repair is with high chance of infection. | Mesh repair is with low chance of infection. |
| 6. | Laprotomy may be needed. | No laprotomy is needed. |
| 7. | Placement of drain is difficult task. | Placement of drain is easy task. |
Data Analysis (N=52) showing in Classical & Present Approaches.
| Conversion/Complication | Classical Approach | Present Approach(Cases & %) |
|---|
| No. of Cases | % (Percentage) |
|---|
| LaparotomyChange of approachChange of incisionWound InfectionMesh Removal | 0312120804 | 5.72323157.6 | –––02 (3.8)*– |
Data were expressed in statistical significance as * p<0.05 (p-value).
In the present approach out of 52 cases 36 were strangulated inguinal hernias and 16 were strangulated femoral hernias, no obturator hernia encountered. No case required laparotomy (0%). No case required change of approach with change of incision (0%). No case required removal of mesh (0%). No case was with recurrence (0%). Only 2 cases developed wound infection at lateral part of incision at the site of second window (3.8%) i.e. (p<0.05). This may be due to availability of higher antibiotics and anastomosis of bowel was away from the mesh repair site. Drain placement is easy through second window.
Discussion
In the classical approach there was change of approach (23%) with change of incision (23%) and in some cases laparotomy (5.7%) and in some cases mesh removal (1.9%) required to complete the procedure. In the present new approach all these were avoided. Wound infection can be reduced significantly *p<0.05 (p-value), leading to decrease chances of mesh removal. This new approach is useful for all groin hernias means elective, emergency, inguinal and femoral which may or may not be with gangrenous bowel without changing incision and approach [7]. The procedure started as simple hernia incision and extended after finding gangrenous bowel. The only difference is that incision is low line skin crease to make access to deal femoral hernia. As the gangrenous bowel is reduced through one window and brought out through another window for resection and anastomosis, hence we name this technique as “Window to Window – One skin incision” approach.
In this present technique, there is no division of muscles, no division of inguinal nerve, no ligation of inferior epigastric artery, hence the the normal anatomy retained. Resection and anastomosis can be done through the same incision away from the site the mesh repair which is covered with mop. As the peritoneal cavity is entered through grid iron incision, any loop of small bowel upto the ileo caecal junction, the vermiform appendix, the caecum and the proximal ascending colon can be managed comfortably. Also, an intra-peritoneal drain can be kept with ease through this incision. In case of a strangulated femoral hernia, the limitations of all the three classical approaches are obviated with this technique especially the change of incision. The limitations of this study is one centre and with one team. It requires multicentre study and analysis.
Sometimes, while releasing the constricting agent, the loop of bowel slips into the peritoneal cavity, and the surgeon is worried whether a gangrenous loop is reduced inadvertently. In such cases, the surgeon can use this technique to explore the bowel and verify the viability of the bowel. This new approach seems to be easier to perform and more ideal compared to other one skin approaches [8,9].
Conclusion
In this present era of minimal access surgery, there is still a role for open surgery, especially strangulated hernias. We propose this new approach to deal all the right-sided groin hernias which is easy to follow. It is a simple approach avoids the confusion as to which incision is to be taken for a strangulated groin hernia, especially so for a femoral hernia. It retains normal anatomy, permits resection and anastomosis of bowel and allows mesh repair without increased risk of infection leading to decreasing recurrence. It gives as good access to place an intra-peritoneal drain and avoids unnecessary laparotomy to inspect a loop of bowel slipped into the abdomen. Hence this new window to window -single incision approach gives a best approach for strangulated groin hernias.
Data were expressed in statistical significance as * p<0.05 (p-value).
[1]. Hachisuka T, Femoral hernia repairSurg Clin North Am 2003 83(5):1189-205. [Google Scholar]
[2]. Elton C, Stoodley BJ, Repair of concomitant inguinal and femoral hernias under local anaesthesiaInt J Clin Pract 2001 55(9):645-46. [Google Scholar]
[3]. Alimoglu O, Kaya B, Okan I, Dasiran F, Guzey D, Bas G, Sahin M, Femoral hernia: a review of 83 casesHernia 2006 10(1):70-3. [Google Scholar]
[4]. Stagnitti F, The femoral hernia: problems in emergency surgeryG Chir 2006 27(6-7):290-94. [Google Scholar]
[5]. Mathonnet M, Mehinto D, Femoral hernias: repair techniquesJ Chir (Paris) 2007 144(Spec No. 4):S15-18. [Google Scholar]
[6]. Peter G, McEvedy. Femoral HerniaAnn R Coll Surg Engl 1950 7(6):484-96. [Google Scholar]
[7]. David T, Strangulated femoral herniaMed J Aust 1967 1:258 [Google Scholar]
[8]. Sorelli PG, El-Masry NS, Garrett WV, Open femoral hernia repair: one skin incision for allWorld Journal of Emergency Surgery 2009 (4:44):1-3. [Google Scholar]
[9]. Thomasn PT, Kittappa K, The Thomas Repair of the strangulated femoral hernia – one skin incision for allJournal of Surgical Case Reports 2011 (7:8):1-3. [Google Scholar]