Spinal anaesthesia is the most commonly performed block for lower abdominal, perineum and lower limb surgery. Many adjuncts like fentanyl, ketamine, tramadol, neostigmine, magnesium sulphate, etc. have been used to prolong the analgesic effect of local anaesthetics. Clonidine has been shown to significantly increase the duration of anaesthesia produced by hyperbaric or isobaric bupivacaine with good safety profile [1–3]. Strebel and colleagues suggested that a dose of 150mcg of clonidine was preferred dose with respect to prolonging spinal anaesthesia with bupivacaine without much side effects [2]. Dexmedetomidine is more selective alpha 2 adrenoceptor agonist and has recently been used as adjuvant to intrathecal local anaesthesia [4–6] Previous animal [7,8] and human trials [5] suggest a 1:10 dose ratio of dexmedetomidine and clonidine. Gupta R et al., used 5mcg of dexmedetomidine with ropivacaine and found it to be associated with prolong motor and sensory block, haemodynamic stability and reduced demand for rescue analgesics in 24 hours as compared to fentanyl [9]. Abdelhamid and El-lakany evaluated the role of dexmedetomidine 5 mcg as adjuvant intrathecally and found it to decrease postoperative analgesic requirement, less shivering among patients of lower abdominal surgery [10]. Hala EA Eid hypothesised and studied that intrathecal dexmedetomidine 10 mcg and 15 mcg would prolong sensory block in a dose dependant manner without major haemodynamic effects [11].
Different observers have recommended different doses of dexmedetomidine. According to previous few studies, as the dose is increased intrathecally, the duration of analgesia increased. But it is possible that cardiodepressant effects like hypotension and bradycardia may also increase.
In this study we tried to find out the optimum dose of dexmedetomidine that should be used in an average built adult Indian population i.e. to find out a dose which is safe and has the analgesic dose sparing effect on the subject at the same time (primary objective). Secondary objectives were to study the characteristics of blocks, the duration of analgesia, the 24 hours analgesic requirement, the highest VRS Score in 24 hours and associated side effects.
Materials and Methods
After getting approval from the Research Ethics and informed consent from 100 adult patients, a randomised controlled, double blinded trial was started. The study was conducted from December 2014 to October 2015. Patients of American Society of Anaesthesiologists (ASA) physical status I and II, of either sex, aged between 18 and 60 years, presenting for lower abdominal surgeries were taken. Patients allergic to any of the drugs used or suffering from neurological diseases, coagulopathy, cardiac diseases, obesity (body weight >120 kg) or height <150 cm or having hypertension were excluded from the study.
Before surgery patients were given instructions to use a 10-point Verbal Rating Scale (VRS), with 0 indicating no pain and 10 indicating the worst imaginable pain. Baseline VRS score were recorded. In the operating room ECG, pulse oximetry and non invasive blood pressure were monitored and baseline values were recorded. With the patient in sitting position, lumbar puncture was performed at L3-4 intervertebral space with 25 G pencil point Quinke spinal needle with all aseptic precautions. Patients were randomly divided into five groups.
All patients received drug volume of 3ml containing 2.5ml of hyperbaric bupivacaine hydrochloride (12.5mg). The study groups received dexmedetomidine (available as 50mcg/0.5ml) 5mcg (group D1), 10mcg (group D2), 15mcg (group D3) and 20 mcg (group D4) in an identical volume of 0.5ml, diluted with normal saline and added to bupivacaine in the same syringe. The control group (Group C) received 0.5ml of NS added to bupivacaine.
No premedication was given. Drugs were injected within 15-20 seconds. Patients, attending anaesthetists and operating room personnel were not aware of the patient allocations. After that the patients were placed in supine position for surgery.
Respiratory depression (RR<8 or SpO2 <95%) was treated with O2 supplementation or respiratory support if required. Hypotension defined as a decrease of systolic blood pressure by >30% from baseline or a fall below 90 mm Hg, was treated with incremental iv doses of 6 mg of injection mephentermine and iv fluid as required. Bradycardia, defined as heart rate (HR) below 50 bpm, was treated with 0.3-0.6 mg of iv atropine. HR, mean arterial blood pressure (MAP) and oxygen saturation were monitored and recorded after the block every 5 minutes for 30 minutes; then at 15min upto 120 min and at 30 min interval thereafter. The incidence of adverse effects such as nausea, vomiting, shivering, respiratory depression, sedation and hypotension were recorded. Sensory testing was assessed by loss of pinprick sensation to 23 G hypodermic needle and dermatome levels were tested every min until the highest level had stabilised by consecutive testing. After this sensory level was tested every 10 minutes till the effect regressed by 2 segments. Thereafter the level was tested every 20 minutes till the sensation was felt at S1 dermatome. Highest level of sensory blockade, the time to reach this level after injection, the time to S1 regression, time to urinate and side effect if any were recorded. The motor block was assessed using the modified Bromage Scale [12]. Sedation was assessed using Ramsay sedation scale [13] before the block and every 15 minutes. Postoperatively HR, MAP, Oxygen saturation (SpO2), sedation score and pain score were recorded initially every one hour for 2 hours, then every 2 hour for next 8 hours and then every 4 hour till 24 hours. Pain score was recorded using VRS scale.
The duration of analgesia was considered as the period from the injection of the study drug to the first request made by the patient for rescue analgesics. Intravenous infusion of diclofenac 75 mg was given, which was repeated after 12 hours, if needed. In absence of satisfactory pain relief with diclofenac, oral tramadol 100 mg was supplemented which could be repeated 4 hourly to a maximum of 400mg. All the analgesics supplemented were recorded.
Statistical Analysis
Data were analysed using SPSS 16. To calculate the sample size, a power analysis of α = 0.05 and β = 0.8 showed that 20 patients were needed in each study group to detect an increase of 30 min difference between the median duration of postoperative analgesia between the groups. Results were expressed as mean and standard deviation (SD) or number or percentages. Analysis of data between groups were performed using one-way analysis of variance (ANOVA). Kruskal Wallis test for non-parametric data was used. Between study groups data were compared using t-test or Mann-Whitney U test. The p-value of less than 0.05 was considered statistically significant.
Results
One hundred patients were enrolled into the study each group: C, D1, D2, D3 and D4 containing 20 patients. The groups were comparable with respect to age, weight, height, sex distribution, ASA physical status and operative time [Table/Fig-1]. There was no significant difference in the type of surgery. Baseline preoperative pain, sedation scores and haemodynamic data did not differ significantly among the groups.
| Patient Profile | Group C | Group D1 | Group D2 | Group D3 | Group D4 | p-value |
|---|
| N=20 | N=20 | N=20 | N=20 | N=20 |
|---|
| Age (years) | 44.21±11.2 | 39.6±10.7 | 39.8±9.58 | 43.32±12.3 | 45.85±9.71 | p=0.73 |
| Sex (M:F) | 15:5 | 16:4 | 13:7 | 14:6 | 12:8 | p=0.14 |
| Weight(kg) | 62.12±7.31 | 62.5±8.01 | 58.8±9.72 | 63.75±8.13 | 61.25±9.29 | p=0.09 |
| Height(cm) | 165.6±3.89 | 167.5±4.03 | 166.9±4.78 | 170.4±3.93 | 167.1±4.29 | p=0.28 |
| ASA I:II | 16:4 | 12:8 | 13:7 | 15:5 | 16:4 | p=0.14 |
| Operative time (min) | 97.5±12.7 | 94.69±13.03 | 93.77±14.2 | 101.15±11.3 | 108.28±8.91 | p=0.08 |
The characteristics of sensory and motor blocks in different groups have been summarised in [Table/Fig-2]. We found significant difference among the groups as far as the onset of sensory or motor blocks or time to reach T10 or the highest level is concerned in comparison to placebo. The trend shows that both sensory and motor block onset time and the time for the block to reach T10 or the highest level decreases as the dose of dexmedetomidine increases. The median and range of the peak sensory level reached were not statistically different among the groups.
Characteristics of sensory and motor block of the studied groups (minutes).
| Group | C | D1 | D2 | D3 | D4 | p-value |
|---|
| Onset time of sensory block | 2.94±0.24 | 2.15±0.74 | 2.01±0.63 | 1.82±0.14 | 1.65±0.32 | 0.0071 |
| Onset time of motor block | 3.61±0.67 | 2.72±0.46 | 2.33±0.57 | 2.23±0.39 | 1.66±0.11 | 0.0004 |
| Onset time to reach T10 dermatome | 8.11±1.09 | 6.55±0.97 | 6.22±0.42 | 4.77±0.31 | 3.45±0.17 | 0.0037 |
| Time to achieve max block | 18.01±3.41 | 14.43±3.11 | 12.01±2.97 | 9.33±2.67 | 8.99±2.72 | 0.037 |
| Highest sensory level | T8(T6-T8) | T8(T6-T8) | T6(T4-T8) | T6(T6-T8) | T6(T6-T8) | |
| Time of 2 segment sensory regression | 94.1±12.2 | 121.3±10.2 | 157.9±28.7 | 218.6±26.8 | 297.2±30.9 | p=0.000 |
| Time of regression to S1 | 228.3±50.4 | 289.1±15.2 | 382.8±48.1 | 598.4±59.6 | 759.8±62.4 | p=0.006 |
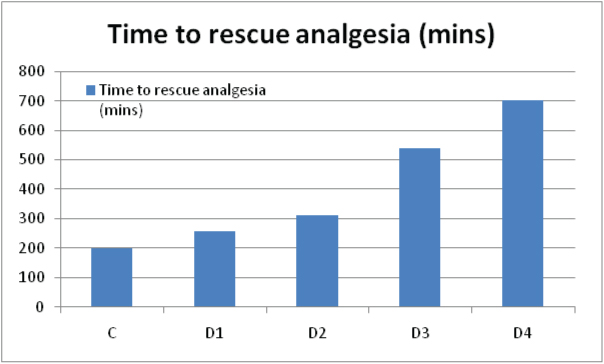
| Time to rescue analgesia | 201.5±29.1 | 259.1±15.2 | 310.7±48.1 | 540.3±51.6 | 702.4±52 | p=0.003 |
| Time of regression to Bromage 0 | 150.6±23.8 | 251.4+46.5 | 386.3+30.7 | 411.7+48.7 | 460.7±52.1 | p=0.006 |
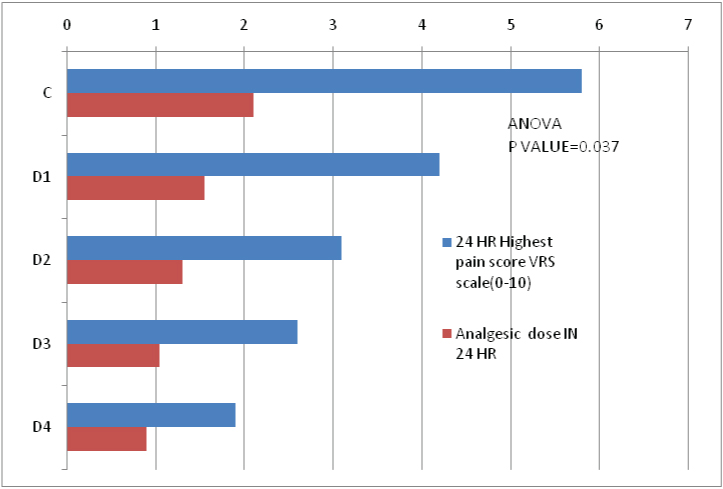
| Highest pain score VRS scale 0-10) | 5.8 | 4.2 | 3.1 | 2.6 | 1.9 | |
| NO. of Diclofenac injections in 1st 24 hours potoperativey | 42 | 31 | 26 | 21 | 18 | |
There was a dose dependent prolongation of the time to two segment sensory regression, regression of sensory level to S1 and regression of motor block to 0 on modified Bromage scale (significant) when compared to placebo. Likewise the duration of analgesia was significantly prolonged among the groups as the dose of dexmedetomidine increased as indicated by the time of first rescue analgesia [Table/Fig-3].
Time of first rescue analgesia.
Considering the supplementary analgesic requirement among the five groups, there were significant decrease in analgesic requirement in 24 hours in groups D1, D2, D3 and D4 when compared to placebo [Table/Fig-4]. Six patients in group C and 3 in group D1 also required tramadol. None of the patients among groups D2, D3 and D4 required tramadol supplementation.
Highest VRS score and 24 hours analgesics requirements.
We also found that some level of sedation was found among 1, 4 and 9 patients belonging to Group D2, D3 and D4 respectively. The number of such patients increased in the groups that received higher dose of dexmdetomidine and so did the sedation score in the groups. But there was no significant difference in the sedation scores among the different groups having sedation. Two, 2 and 4 patients had respiratory depression among the groups D2, D3 and D4 who were given oxygen supplementation [Table/Fig-5].
Adverse effects in all groups.
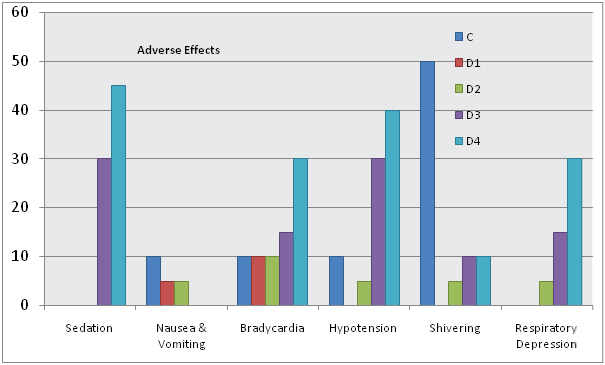
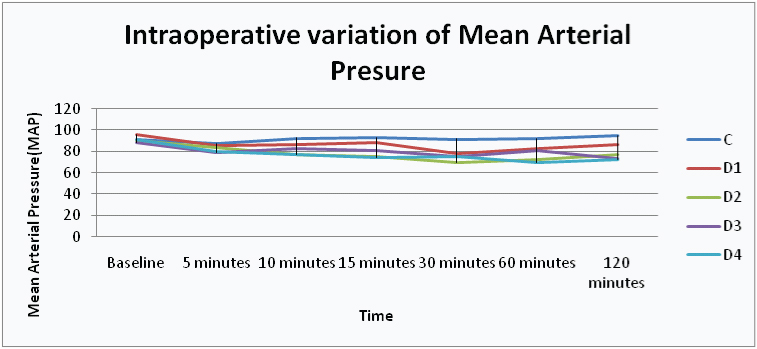
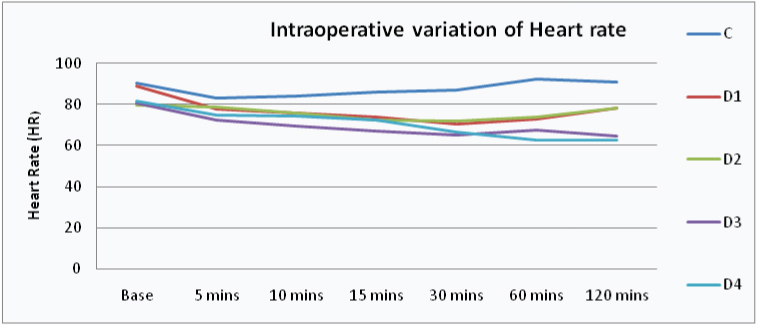
The mean value of MAP and HR were comparable between the groups throughout the duration of study [Table/Fig-6,7]. Some patients required supplementation of injection mephentermine to coutereract hypotension which was more in group C, D3 and D4 when compared with group D1 and D2. Nausea and vomiting was noted in few patients of C, D2 and D3 and was treated by giving injection ondansetron 8 mg Complete recovery of sensory and motor function was seen in all the patients. None of the patients showed any neurological deficit in follow up visits. Seven patients of the control group, 3 patients of D2 and 2 patients of group D3 had shivering [Table/Fig-5].
Intraoperative mean arterial pressure.
Intraoperative mean heart rate.
Discussion
Injection Bupivacaine when used alone is adequate for surgeries lasting 2-3 hours. Hence, if we require regional anaesthesia for longer duration we use some additive. Addition also has advantage of providing postoperative analgesia. A number of adjuvants have been studied to prolong the effect of spinal anaesthesia. Dexmedetomidine is one among them.
Dexmedetomidine is a specific and selective alpha 2 adrenoceptor agonist. Activation of receptors in the brain and spinal cord inhibits neuronal firing and leads to sympatholytic effect, causing hypotension, bradycardia, sedation and analgesia [14].
Many animal studies conducted using intrathecal dexmedetomidine at a dose range of 2.5-100 mcg did not report any neurological deficit or neurotoxicity [15–19]. Kanazi et al., used a small dose of dexmedetomidine (3mcg) with bupivacaine intrathecally in humans. They found a shorter onset of motor block and a prolongation in the duration of motor and sensory block with haemodynamic stability and lack of sedation [5]. According to Gupta et al., 5 mcg of dexmedetomidine when added to hyperbaric bupivacaine, there was significant prolongation of the duration of sensory as well as motor block, quality of intraoperative and postoperative analgesia improved, the patients were haemodynamically stable and had minimal side effects [9]. Al-Mustafa et al., studied effect of dexmedetomidine 5 and 10 mcg with bupivacaine in urological procedures and found that dexmedetomidine prolongs the duration of spinal anaesthesia in a dose-dependent manner [20]. Hala EA Eid et al., in their study using 10 and 15 mcg in spinal anaesthesia with in 3 ml of 0.5% hyperbaric bupivacaine, found significantly prolonged anaesthetic and analgesic effect which could be of benefit in complex lower limb surgeries especially using 15 mcg dose [11].
In our study we used four different doses of dexmedetomidine, 5, 10, 15 and 20mcg in comparison with placebo as an adjunct to hyperbaric bupivacaine in order to explore which dose is the optimum for intrathecal use i.e. provides maximum duration of intraoperative anaesthesia and postoperative analgesia and at the same time produce negligible side effect. Hala E A Eid et al., found no haemodynamic instability in their study using 10 and 15 mcg in spinal anaesthesia [11]. Hence we decided to take a dose of 20 mcg to compare it with 15 mcg of dexmedetomidine to see if this also gives haemodynamic stability and upto what extent it prolongs the analgesic effect of bupivacaine.
The onset of sensory and motor block was significantly earlier in dexmedetomidine groups as compared to control group and in groups with higher doses when compared to those with lower doses. Similar to our result Ogan et al., and Shukla et al., showed significantly earlier onset of peak sensory block and time to reach Bromage 3 level of sensory block [21,22]. We found that all patients receiving dexmedetomidine had less postoperative pain scores and longer duration of analgesia as compared to control group. This effect was more pronounced as the dose of dexmedetomidine increased as indicated by the 24 hours analgesic consumption. The haemodynamics were maintained towards low normal in most of the patients in group D1 and D2. Some patients in these groups and more number of patient in group D3 and D4 had hypotension which was corrected by giving i.v. fluid boluses and injection mephentermine.
Sedation score of 2 in many patients in group D3 and D4 and a few patients in D2 can be justified as alpha 2 agonists produce sedative effect by acting on alpha 2 adrenergic receptors in locus ceruleus [23,24]. The cause of sedation in higher doses may be due to systemic absorption and vascular redistribution to the higher centres or cephalad migration in CSF [25]. Similar result was seen by Hala EA Eid et al., with intrathecal dexmedetomidine 15 mcg in concentration [11]. In fact sedation had added benefit as patients were calm and quiet and did not require any extra sedation and at the same time they were conscious and could be easily aroused.
In our study there were significant increase in the duration of sensory and motor block of spinal anaesthesia and prolonged postoperative analgesia. The effect was more as the dose increased. This effect can be utilized in patients undergoing prolonged surgery and it can be a good alternative to epidural anaesthesia which requires a much higher dose of drug and to general anaesthesia. But one has to be vigilant because a good number of patients had a fall in heart rate and BP when 15 and 20 mcg dose of dexmedetomidine were used intrathecally. Hala EA Eid et al., and Al-Mustafa et al., also found a dose dependant prolongation of motor and sensory block and reduced requirement of analgesics with increasing dose of dexmedetomidine (5, 10 and 15 mcg) [11,20]. This is the only study in which a dose of 20 mcg have been used.
Bradycardia occurred in 30% cases in D4 and 15% cases in D3 compared to 10% cases in control, D1 and D2 each. Bradycardia with Dexmedetomidine is due to postsynaptic activation of central alpha group 2 adrenoceptors resulting in sympatholytic effect, leading to hypotension and bradycardia, an effect that can be judiciously used to attenuate the stress response of surgery [26].
In all cases where dexmedetomidine was used, the fall in BP and heart rate was seen after 30 minutes. This can be explained by the biphasic response of dexmedetomidine: A short hypertensive phase and subsequent hypotension. The initial hypertensive phase is due to alpha 2B adrenergic receptors whereas hypotension is mediated by the alpha 2A adrenergic receptors. According to Gertler R et al., the initial response lasts for 5 to 10 minutes and is followed by a decrease in blood pressure of approximately 10% to 20% below baseline and stabilization of the heart rate, also below baseline values; both of these are caused by the inhibition of the central sympathetic outflow overriding the direct stimulating effects [27]. We believe that the initial hypertension caused by dexmedetomidine is compensated by hypotension caused by Bupivacaine. Hence BP was maintained for about 30 minutes and we noticed the hypotensive phase only after that, nausea or vomiting was associated with the hypotensive episodes. This may be due to the fact that increased vagal activity after sympathetic block causes increased peristalsis of the gastrointestinal tract, which leads to nausea [28]. But in D4 though the incidence of hypotension was high as compared to other groups, nausea and vomitting was not seen in any patient. This could be due to sedation.
Shivering was noticed in patients of D2 and D3 but not in D4. Previous studies have shown that dexmedetomidine has antishivering property [29]. So the incidence in D2 and D3 could be due to OT environment.
Limitation
The limitation of our study is that we have considered the analgesic effect of intrathecal dexmedetomidine in healthy patients of ASA I and II. Its effect on patients of ASA III and IV and those having co-morbidities is yet to be studied. We also cannot comment about its effect on patients in extremes of age. So, use of recommended dose of dexmeditimodine in comorbid, elderly and complicated systemic illness should be weighed before use.
Conclusion
Dexmedetomidine significantly enhances the onset of sensory and motor block in comparison to placebo in a dose dependant manner and so is the duration of blocks and the anagesia provided. Hence it can be exploited in long duration surgery as an alternative to epidural anaesthesia. But when we use higher doses like 15mcg and 20mcg more vigilance is required due to higher incidence of hypotension and bradycardia. Significant prolongation of analgesia and significantly less side effects leads us to conclude that 10 mcg of dexmedetomidine is the optimum dose. We recommend the use of 10mcg of intrathecal dexmedetomidine as an adjuvant to bupivacaine as it seems to be a good alternative to other additives for long duration surgical procedures due to its profound intrathecal anesthetic and analgesic properties combined with minimal side effects.