Benign Lymphoepithelial Cyst of the Parotid in HIV Negative Patient
Suresh Pillai1, Ashish Chandra Agarwal2, Ajay Bhandarkar Mangalore3, Balakrishnan Ramaswamy4, Shama Shetty5
1 Senior Consultant, Department of Otolaryngology-Head and Neck Surgery, Sultan Qaboos Medical University, Oman.
2 Assistant Professor, Department of Otolaryngology-Head and Neck Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
3 Associate Professor, Department of Otolaryngology-Head and Neck Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
4 Professor and Head, Department of Otolaryngology-Head and Neck Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
5 Senior Resident, Department of Otolaryngology-Head and Neck Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ashish Chandra Agarwal, Assistant Professor, Department of Otolaryngology-Head and Neck Surgery, Kasturba Medical College, Madhavnagar, Manipal University, Manipal - 576104, Karnataka, India.
E-mail: ashishagr3@rediffmail.com
Benign lymphoepithelial cysts are slow growing tumours commonly seen in HIV positive adults. It is rare to find them in non HIV individuals. In this article we discuss an uncommon presentation of a parotid swelling occurring in a 49-year-old non HIV male, which was diagnosed as benign lymphoepithelial cyst. The various investigative modalities and treatment options are outlined in this article.
Cystic lymphoid hyperplasia, Parotidectomy, Salivary gland
Case Report
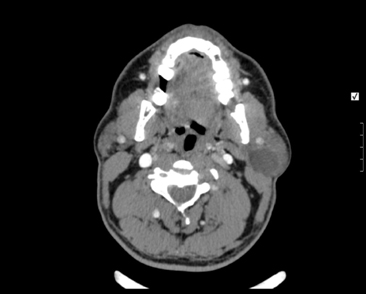
A 49-year-old gentleman presented to the ENT outpatient department of a tertiary care hospital with history of recurrent swelling over left side of the face [Table/Fig-1] since 2 years. It was insidious in onset and had gradually progressed to the present size of about 4x4 cm. The swelling was not associated with pain or change in size while having food, but, was cosmetically disfiguring. He had been treated with repeated course of antibiotics during the past two years without improvement. Clinical examination revealed an oval swelling over the left parotid region which was 4x4 cm in dimension, firm in consistency and not adherent to the skin or underlying structures. There was no cervical lymphadenopathy. Right parotid gland was normal. Stensens duct opening was normal. No discharge was seen coming from the duct orifice on applying pressure over the gland. CT scan [Table/Fig-2] of the parotid showed a non-enhancing, homogenous, hypodense lesion in the superficial lobe of left parotid gland and the Fine Needle Aspiration Cytology (FNAC) was suggestive of chronic sialadenitis. The hospital protocol for HIV diagnosis was followed. HIV rapid test, ELISA and Western blot were reported negative. Differential diagnosis considered was pleomorphic adenoma, warthin’s tumour, fibroma and lipoma. The patient underwent left superficial parotidectomy under general anaesthesia for removal of the swelling. The histopathology [Table/Fig-3] report was suggestive of a Benign Lymphoepithelial Cyst (BLEC) of the parotid. The lesion did not recur at 3 months, 6 months and 1 year of follow up and facial nerve function was normal.
Swelling in the region of left Parotid.

Axial CT scan demonstrating the lesion in the superficial lobe of left Parotid.
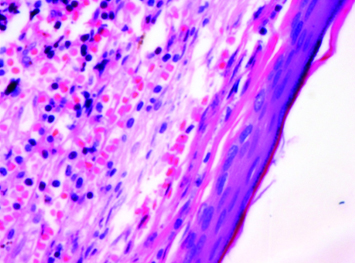
Haematoxyllin and eosin staining (10X magnification) showing cyst composed of keratin flakes and lymphoplasmacytic infiltrates.
Discussion
BLEC has been defined as occurrence of single or multiple cysts within salivary gland lymph nodes [1,2]. The primary pathogenic mechanism deals with involvement of lymph node tissue and hence an elevated concentration of the retrovirus can be noted within this tissue [3]. Lymphocytic enlargement within the parotid gland has been described in various ways, namely, AIDS related lymphadenopathy, cystic lymphoid hyperplasia, Benign Lymphoepithelial Lesion (BLEL), HIV-associated salivary gland disease and Diffuse Infiltrative Lymphocytosis Syndrome (DILS) [4].
Histologically, lymphocytic involvement in HIV positive patients presents in three distinct forms: 1) Reactive follicular hyperplasia, also called as Persistent Generalized Lymphadenopathy (PGL); 2) Diffuse lymphocytic infiltration (BLEL); and 3) Intraductal epithelial proliferation with cyst formation (BLEC) [4]. Salivary gland BLEL is known to be associated with an increased risk of malignant lymphoma. BLEC has a wall lined by stratified epithelium, most commonly squamous, but may be columnar, cuboidal, or pseudo-stratified type. The cyst wall also contains aggregations of lymphoid tissue and the salivary parenchyma has a normal appearance. This feature differentiates BLEC from BLEL. In our patient, the histopathology revealed the cyst wall lined by focally atrophied stratified squamous epithelium with luminal keratin flakes, surrounded by periepithelial dense lymphoplasmacytic infiltration.
The first case of BLEC was reported by Hildebrandt in 1895, and until 1981, only 21 cases had been described [4]. With the emergence of HIV epidemic, the incidence of parotid gland BLEC has increased and it now occurs in an estimated 3% to 6% of HIV-positive adults and 1% to 10% of HIV positive children, respectively [4]. The exact prevalence of its occurrence in non HIV patients could not be found in literature.
BLEC usually presents in the early stage of HIV infection as slowly progressive, asymptomatic parotid gland enlargement. It may present with cervical lymphadenopathy in up to 90% of cases. CT and MRI show the presence of bilateral and multicystic appearance of lymph nodes in an HIV affected patient when compared to a non HIV patient and this can be considered to be an important radiological diagnostic sign [5]. BLEC do not recur or metastasize, hence it is important to differentiate them from aggressive lesions, especially cystic low grade muco-epidermoid carcinoma [4]. Ultrasound, CT, and MRI demonstrate multiple thin-walled cysts with diffuse cervical lymphadenopathy [6], but in our case we did not encounter cervical lymphadenopathy possibly due to the fact that the patient was not immunocompromised. FNAC in case of BLEC usually yields a straw or yellow colored fluid, but in our patient, cheesy material was found within the cyst due to the presence of keratin flakes as a result of the squamous epithelial lining.
Different treatment options for HIV-associated BLEC include observation, repeated aspiration, antiretroviral medication, sclerosant therapy, radiation therapy and surgery [4]. Observation can be made in asymptomatic patients and most children. Aspiration is generally ineffective and the cysts recur within weeks to months. Sclerotherapy may occasionally be attempted for treating HIV associated BLEC.
Conclusion
BLEC is a rare benign swelling in non HIV patients. Our search of medical literature reveals this swelling to be predominantly present in HIV positive individuals. Though there are multiple treatment options available, there are very few articles outlining the management in non HIV patients. Our patient remained recurrence free even after a period of one year following superficial parotidectomy. This article has been written to highlight the fact that BLEC must be kept in mind as one of the differential diagnosis for parotid swellings even in non HIV patients.
[1]. Varnholt H, Thompson L, Pantanowitz L, Salivary gland lymphoepithelial cystsEar, Nose & Throat J 2007 86(5):265 [Google Scholar]
[2]. Ebrahim S, Singh B, Ramklass SS, HIV-associated salivary gland enlargement: a clinical reviewSADJ 2014 69(9):400-03. [Google Scholar]
[3]. Naidoo M, Singh B, Ramdial PK, Moodley J, Allopi L, Lester B, Lymphothelial lesions of the parotid gland in the HIV era- a South African experienceS Afr J Surj 2007 45(4):136-38.:140 [Google Scholar]
[4]. Dave SP, Pernas FG, Roy S, The benign lymphoepithelial cyst and a classification system for lymphocytic parotid gland enlargement in the pediatric HIV populationLaryngoscope 2007 117(1):106-13. [Google Scholar]
[5]. Alves CAF, Junior OR, Borba AM, Parotid lymphoepithelial cyst in non-HIV patientJ Clin Exp Dent 2011 3(Suppll):e400-03. [Google Scholar]
[6]. Suskind DL, Travil MA, Handler SD, Doxycycline sclerotherapy of benign lymphoepithelial cysts of the parotid: a minimally invasive treatmentInt J Pediatr Otorhinolaryngol 2000 52(2):157-61. [Google Scholar]