A Rare Presentation of Two Cases of Metallic Intrascleral Foreign Body Entry through Upper Eyelid
Satish C Shitole1, Rakesh K Barot2, Rakesh Shah3, Nupur Bhagat4
1 Assistant Professor, Department of Ophthalmology, Rajiv Gandhi Medical College and CSM Hospital, Kalwa, Thane, Maharashtra, India.
2 Associate Professor, Department of Ophthalmology, Rajiv Gandhi Medical College and CSM Hospital, Kalwa, Thane, Maharashtra, India.
3 Honorary Consultant, Department of Ophthalmology, Rajiv Gandhi Medical College and CSM Hospital, Kalwa, Thane, Maharashtra, India.
4 Resident, Department of Ophthalmology, Rajiv Gandhi Medical College and CSM Hospital, Kalwa, Thane, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satish C Shitole, 104/C, Magha, Kores Nakshtra, Vartak Nagar, Thane West-00606, Maharashtra, India.
E-mail: drsatish.shitole@gmail.com
Ocular injury secondary to foreign body remains an important cause of ocular morbidity with or without blindness in working population. Intraocular foreign body may have varied clinical presentation. Initially it may look an apparently normal eye followed by obvious ocular symptoms depending upon its location and degree of inflammation. It can result in partial or full thickness penetration of sclera with or without involvement of posterior segment. We hereby present two cases of metallic intrascleral foreign body entry through upper lid in young carpenters following hammer and chisel injury. In case 1, Intrascleral location of foreign body was confirmed with X ray orbit and B scan ultrasonography while in case 2 the diagnosis of intrascleral foreign body was missed at the first visit to ophthalmology clinic Both the patients underwent exploratory surgeries where intrascleral metallic foreign bodies were found without ocular penetration. An intrascleral foreign body may be missed due to small penetrating scleral wound covered by a large subconjunctival haemorrhage accompanied by minimal or no signs of inflammation and failure on part of treating ophthalmologist to suspect an intrascleral foreign body. To establish a diagnosis of intraocular particularly intrascleral foreign body, careful history taking and clinical examination along with use of imaging studies are mandatory steps which help in successful management and good visual outcome. These cases highlight the importance of considering a presumptive diagnosis of retained intrascleral foreign body in every patient with a history of penetrating ocular trauma through lid or a visible wound/scar on the lid.
Eye lid scar, Hammer and chisel injury, Scleral tear
Case Report
Case 1
A 20-year-old male carpenter presented to ophthalmology department of Rajiv Gandhi Medical College and CSM Hospital with complaints of redness & watering in right eye since 2 days. He gave history of some particle hitting over right eye 2 days back when he was hammering a nail. He was not wearing any eye protective device at the time of injury.
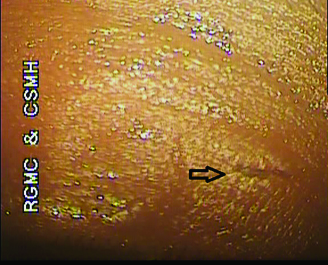
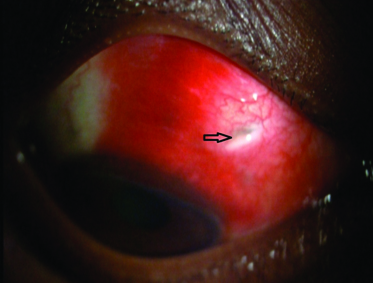
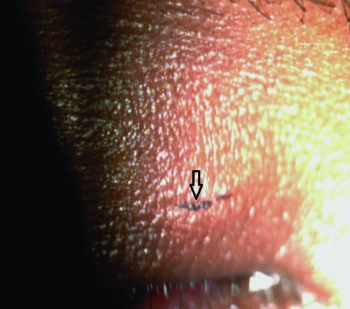
Slit lamp biomicroscopic examination revealed a 4 mm linear scar of an entry wound on medial 1/3rd of right upper eye lid skin, subconjunctival haemorrhage in superior bulbar conjunctiva extending to the upper fornix and granulation tissue over conjunctiva between 1 to 2 o’clock position 4 mm behind the limbus [Table/Fig-1,2]. Seidel’s test was negative. Remaining anterior segment examination was unremarkable. Best corrected right eye visual activity was 6/18 and left eye was 6/6. Dilated fundus Examination with Indirect Ophthalmoscope revealed no abnormality in vitreous and retina. Patient was advised X ray Orbit and B-scan Ultrasonography to rule out intraocular foreign body. Radio opaque density was noted in superior orbital region on X ray orbit AP view [Table/Fig-3]. B-Scan ultrasonography examination confirmed the intrascleral location of metallic foreign body without any associated vitreous haemorrhage, vitritis or retinal detachment.
Case 1 Arrow showing Entry wound of 4 mm on upper eye lid skin
Case 1 Arrow showing Subconjunctival hemorrhage in superior bulbar conjunctiva between 1 to 2 o’clock positions.
Case 1 Arrow showing Radio opaque density in superior orbital region on x ray orbit.
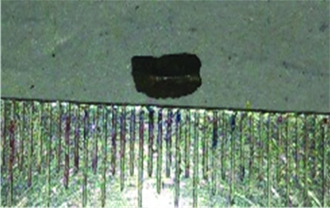
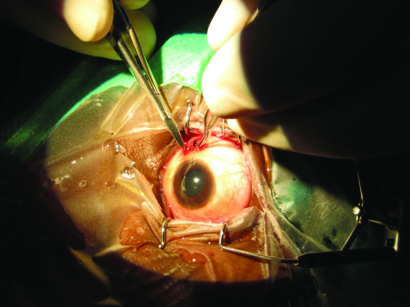
Patient was operated upon next day for right eye intrascleral foreign body removal under peribulbar anesthesia. During surgery, a linear scar on conjunctiva 4 mm away from limbus at 2 o’clock position was noted and two edges of conjunctival scar were separated to expose scleral wound. On exploration of scleral wound intrascleral metallic foreign body was noticed. The metallic iron foreign body of size 5 mm x 1.5 mm was removed after extending the scleral wound and underlying choroid was evident without vitreous prolapsed [Table/Fig-4,5 and 6]. Fibrous and exudative tissue around the wound was excised. Sclera was sutured with 6-0 vicryl interrupted sutures. Prophylactic retinal laser was done to avoid secondary retinal detachment. Vision on 1st postoperative day was 6/12 and after 1 month vision was 6/6.
Case 1 Removal of intrascleral foreign body.
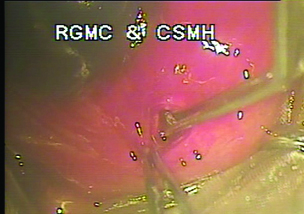
Case 1 Scleral wound with underlying choroid.

case 1 Metallic foreign body (5mm x 1.5mm).
Case 2
An 18-year-old male carpenter presented to ophthalmology department of Rajiv Gandhi Medical College and CSM Hospital with complaints of redness since 13 days and pain, watering with foreign body sensation in left eye since 5 days. He gave history of some particle hitting over left eye 13 days back when he was hammering a nail without use of protective goggles, followed by a reddish patch in upper part of the eye. It was not accompanied by pain, watering or decrease in vision. Next day he visited a local ophthalmologist and was given treatment for sub conjunctival haemorrhage. No radiological investigation was done during that visit. A week later he started having pain, watering and foreign body sensation in the same eye which increased in intensity over few days. After five days of complains, he visited our outpatient department.
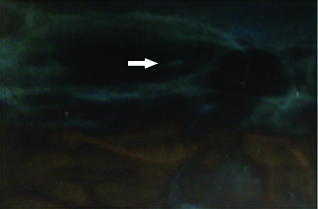
Slit lamp biomicroscopic examination revealed a linear scar of 2 mm on medial 1/3rd of left upper eye lid, suggesting an entry wound [Table/Fig-7]. A subconjunctival haemorrhage in superior bulbar conjunctiva was noted nasally from 10-11 o’clock position approximately 5 mm behind the limbus. Intrascleral metallic foreign body was seen jutting out from the subconjunctival haemorrhage [Table/Fig-8]. Seidel’s test was negative. Remaining anterior segment examination was unremarkable. Best corrected left eye visual activity was 6/24 and right eye was 6/6. Dilated fundus Examination with Indirect Ophthalmoscope revealed vitreous haemorrhage and normal retina. Patient was advised an X-ray of Orbit and B-scan Ultrasonography of left eye to look for exact location and depth of intraocular foreign body. Radio opaque density was noted in left superior orbital region on X ray orbit. Ocular B-scan revealed echogenic debris within the vitreous humor in the left eye suggestive of a vitreous haemorrhage and an acoustic shadow suggestive of a foreign body in the posterior aspect of the left eye in the scleral layers.
Case 2 Arrow showing Entry wound of 2mm on upper eye lid skin.
Case 2 Jutting out Intrascleral metallic foreign body.

The patient was posted for left eye intrascleral foreign body removal under peribulbar anesthesia. Conjunctiva was incised between 10-11 o’clock and scleral wound was explored and the metallic iron foreign body of size 3 mm x 2.5 mm was removed with ease as it was non adherent to sclera [Table/Fig-9,10]. Fibrous and exudative tissue near wound was excised and scleral edges of the wound were freshened with 11 no. blade and sutured with interrupted 6-0 vicryl sutures. Prophylactic retinal laser was done to avoid secondary retinal detachment. Best corrected visual acuity on 1st postoperative was 6/24 and 6/6 at the end of one month. On follow up examination at one month vitreous haemorrhage had resolved and retina was normal.
Case 2 Removal of foreign body.
Case 2 Metallic foreign body of size 3mm x 1 mm.

Discussion
The foreign bodies may be classified as metallic or nonmetallic, with the metallic being divided into magnetic and nonmagnetic [1]. Most intraocular foreign bodies are found in young male workers as a consequence of work accidents and majority of these types of injuries are preventable [2].
Very little medical literature is available on diagnosis and management of intrascleral foreign body. In both the cases iron foreign bodies were found. Iron containing intrascleral foreign body may result in ocular siderosis even after a period of one year [3]. Complications associated with intrascleral location of foreign body are cataract, siderosis bulbi, uveal melanoma, Chorioretinitis Sclopetaria and secondary infection [4–6]. Sertan et al., reported case of retained intrascleral metallic foreign body for 25 years causing cataract formation probably due to low grade anterior uveitis [7].
Both our Patients were young male carpenters and sustained ocular injury due to non usage of protective eye wear while using hand wielded hammer and chisel. In our patients, the entry point of intraocular foreign body was through the upper eye lid which is a common site of entry in addition to cornea [2]. The size and velocity of the particle are of importance, as it determines the injury to deeper structures like vitreous or retina. Our cases were unusual because they were not associated with globe penetration inspite of having full thickness scleral penetration. The possible explanation is the decrease in velocity of the foreign body before entering sclera as it hit upper eye lid first.
An intrascleral foreign body may be missed due to a small penetrating scleral wound covered by a large subconjunctival haemorrhage accompanied by minimal or no signs of inflammation as in case 1 and failure on part of treating ophthalmologist to suspect an intrascleral foreign body as evident in case 2. Therefore these cases highlight the importance of considering a presumptive diagnosis of retained intrascleral foreign body in every patient with a history of penetrating ocular trauma through lid or a visible wound/scar on the lid. These cases also suggest that establishing a diagnosis of intraocular particularly intrascleral foreign body requires a careful history taking and clinical examination alongwith use of imaging studies. These steps are mandatory which evantually help in successful management and good visual outcome [8,9].
These cases also suggest that injuries sustained by these workers were totally preventable with the use of well fitted, protective eye wear with good visibility and strict compliance on its use. Extensive occupational eye safety program with focus on the specific tasks or kinds of work with high risk, regardless of sex and age and developing a country wide strategy will take a long way in preventing work related eye injuries.
Conclusion
Small intrascleral foreign body may be easily missed due to small penetrating wound which may be accompanied by minimal or no sign of inflammation. A careful history, clinical examination, suspician of IOFB and imaging studies are useful for establishing the diagnosis of foreign body. Timely intervention and monitoring for complications help in acheiving good visual outcome in such cases Occupation eye safety campaigns among workers are required for prevention of such injuries.
[1]. De Juan E, Sternberg P, Michels RG, Penetrating Ocular Injuries. Types of injuries and visual resultsOphthalmology 1983 90(11):1318-22. [Google Scholar]
[2]. Lit ES, Young LH, Anterior and posterior segment intraocular foreign bodiesInt Ophthalmol Clin 2002 42:107-20. [Google Scholar]
[3]. Fineman MS, Sharma S, Shah GK, Ultrasound biomicroscopic diagnosis of an occult Intrascleral foreign body: an unusual case of ocular siderosisRetina 2001 21(3):265-67. [Google Scholar]
[4]. Macarie SS, Macarie D, Complications of intraocular foreign bodiesOftalmologica 2004 48(3):57-60. [Google Scholar]
[5]. Park SS, Theodossiadis PG, Gragoudas ES, Intrascleral foreign body simulating extrascleral extension of uveal melanomaArch Ophalmol 1994 112:1620 [Google Scholar]
[6]. Burch PG, Albert DM, Transscleral ocular siderosisAm J Ophthalmol 1977 84:90-97. [Google Scholar]
[7]. Sertan G, Yasar S, Muammer O, Rabia S, Cataract in Low-Grade Uveitis Due to Scleral Foreign BodyEur J Gen Med 2014 11(4):282-84. [Google Scholar]
[8]. Lustrin ES, Brown JH, Novelline R, Weber AL, Radiologic assessment of trauma and foreign bodies of the eye and orbitNeuroimag Clin North Am 1996 6(1):219-37. [Google Scholar]
[9]. Yeh S, Colyer MH, Weichel ED, Current trends in management of intraocular foreign bodiesCurr Opin Ophthalmol 2008 19:225-33. [Google Scholar]