Intravenous Immunoglobulin Responsive Persistent Thrombocytopenia after Dengue Haemorrhagic Fever
Prabhat Kumar1, Riyaz Charaniya2, Anindya Ghosh3, Ratnakar Sahoo4
1 Senior Resident, Department of Medicine, PGIMER & Dr RML Hospital, New Delhi, India.
2 Postgraduate Resident, Department of Medicine, PGIMER & Dr RML Hospital, New Delhi, India.
3 Postgraduate Resident, Department of Medicine, PGIMER & Dr RML Hospital, New Delhi, India.
4 Professor, Department of Medicine, PGIMER & Dr RML Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prabhat Kumar, Senior Resident, Department of Medicine, OPD Block, PGIMER & Dr RML Hospital, Baba Kharak Singh Marg, New Delhi-110001, India.
E-mail: drkumar.prabhat@gmail.com
Dengue outbreak is common in Indian subcontinent and causes significant morbidity and mortality. Year 2015 has witnessed yet another Dengue epidemic in northern India and the number of cases this year is maximum in a decade. Dengue infection is a viral disease and there are 4 different serotypes DENV1, DENV2, DENV3 and DENV4. This year DENV2 and DENV4 have been isolated from most of the patients. Thrombocytopenia is hallmark of dengue infection and generally recovers within ten days of onset of symptoms. We report a case of dengue haemorrhagic fever in which thrombocytopenia persisted for almost a month and improved after Intravenous immunoglobulin (IVIG) administration. This is the first case where IVIG has been successfully used for treating persisting thrombocytopenia after dengue infection.
Immune Thrombocytopenic Purpura, Intravenous Methylprednisolone, Steroid
Case Report
A 21-year-old lady, resident of Delhi presented to our hospital with complaints of high grade fever with chills for five days and rashes in both legs for one day. On physical examination, she had tachycardia with a pulse rate of 106/min, Blood Pressure-106/70mmHg (no orthostatic fall), Respiratory rate-16/min, temperature-101.8 degree F. There was petechial rash over lower limbs. There was mild ascites without any organomegaly. A provisional clinical diagnosis of Dengue Haemorrhagic fever was made.
Blood investigation done at the time of admission showed Haemoglobin of 11.9 gm% with Total Leukocyte Count (TLC) of 5000 per cu mm (64% polymorphs, 35 % lymphocytes, 01 monocyte), PCV 36 and platelet count of 15,000 per cu mm. The renal and liver function tests along with serum electrolytes and urine microscopy were within normal limits. Tests for malaria and rickettsial disease were negative. Dengue serology IgM (by MAC-ELISA) was positive.
Initial treatment included intravenous fluids to maintain adequate hydration and oral paracetamol tablets for fever spikes. Next day her platelet count further decreased to 10,000 per cu mm. She was transfused one unit of Single Donor Platelet (SDP) and on next day platelet count increased to 30,000 per cu mm. On 3rd day of admission she became afebrile but her platelet count again came down to 20,000 per cu mm. As there was no active bleeding, we decided against further platelet transfusions. She improved clinically and petechial lesions started resolving. She was discharged on 5th day with a platelet count of 40,000 per cu mm.
Two weeks after discharge she came to the emergency room with complaints of petechial rash over upper and lower limbs for one day, without any fever. Haemogram showed a platelet count of 15,000 per cu mm and other parameters were normal. She was transfused with one unit of SDP, which raised platelet count to 30,000 per cu mm. This time we decided to look for any secondary cause of thrombocytopenia and a bone marrow examination was done on 3rd day of admission which showed adequate megakaryocytes without any other abnormality. ANA (Antinuclear antibody) test done by indirect immunofluroscence was negative and tests for HIV, hepatitis B and C were also negative.
On 4th day of second admission her platelet count again dipped to 20,000 per cu mm. She was given 1 gm of intravenous methyl prednisolone between 4th-6th day of admission. Platelet count on day 5- 20,000, day 6- 15,000, day 7- 22,000 and on day 8- 20,000 per cu mm.
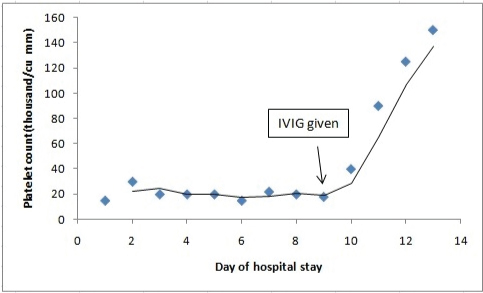
As there was no response to high dose steroids we decided to give a trial of intravenous immunoglobulins (IVIG). IVIG was given on 9th day at a dose of 1gm/kg. There was a dramatic response after IVIG administration and platelet count started improving. Platelet count on day 10- 40,000, day 11- 90,000 and on day 12- 1.25 lacs per cu mm [Table/Fig-1]. She was discharged on 13th day and was followed up. Repeat platelet counts done after 2 weeks, 1 month and 2 months were 1.7 lacs, 1.8 lacs and 1.65 lacs per cu mm respectively.
Thrombocytopenia responded dramatically to IVIG therapy.
Discussion
Dengue is a viral disease that is rampant in tropical and subtropical areas of the world. It is caused by 4 antigenically distinct dengue virus (DENV) serotypes DENV1, DENV2, DENV3 and DENV4, of the genus Flavivirus. The infection is transmitted between humans by Aedes mosquito and man is the main reservoir of the virus. The clinical feature ranges from self limiting Dengue fever (DF) to Dengue Haemorrhagic Fever (DHF). DHF is characterized by severe thrombocytopenia and haemorrhagic manifestations which can be associated with circulatory collapse and shock. As per recent WHO classification scheme for dengue, patients are classified into two groups “dengue” and “severe dengue”.
After an incubation period of 5-8 days, symptoms begin and typically follow three phases-febrile phase, critical phase and recovery phase. Febrile phase is characterized by high grade fever, headache, myalgia and mild haemorrhagic manifestations like petechiae. There can be mild leucopenia and thrombocytopenia and this phase usually last for 3-7 days. Critical phase starts at the time of defervescence and is characterized by plasma leakage. The increased vascular permeability leads to rise in haematocrit, serositis, moderate to severe thrombocytopenia and haemorrhagic manifestations. Some of the patients develop shock in this phase and carries a poor prognosis if not treated immediately; the critical phase usually lasts in 2-3 days and is followed by recovery phase. Bradycardia and a maculopapular rash are commonly seen in recovery phase.
Serologic diagnosis of dengue is made by detection of High levels Serum IgM antibodies to dengue by ELISA. Serum IgM typically appears after 4-5 days of onset of symptom. Detection of nonstructural protein 1(NS1) by ELISA has the highest diagnostic yield between day 1-4 of illness.
Thrombocytopenia is defined as rapid decline in platelet count or platelet count less than 150,000 per microliter of blood. In dengue infection platelet starts decreasing after day 3 of illness and reaches normal levels on 8th or 9th day [1,2]. There are various proposed mechanisms of thrombocytopenia in dengue. Bone marrow suppression occurs during early phase of the disease. The factors responsible for marrow suppression are defective bone marrow regulation, direct insult to progenitor cell by DENV and infection of stromal cells [3]. Increased peripheral destruction of platelet also contributes to thrombocytopenia. It has been demonstrated that patients of dengue have anti-platelet antibodies of IgM isotype [4]. Anti platelet IgM titres are typically more in DHF than DF, complement activation further aggravates platelet destruction. Direct platelet infection by DENV leading to immune mediated destruction has been shown in various studies [5]. Both coagulation and fibrinolytic pathways are activated in dengue infection leading to consumption of platelets [6]. Lastly, there is platelet dysfunction in DENV causing altered activation and aggregation of platelets.
Persistent thrombocytopenia after dengue fever is a rare entity with only few reported cases [7–9]. In most of the previous cases there was response after steroid therapy which was given either as intravenous methylprednisolone or oral prednisolone [10]. Steroid acts by inhibiting Fc-receptor mediated platelet phagocytosis and by reducing anti-platelet antibody synthesis [11]. In our case, no response was seen after three days of pulse intravenous methylprednisolone and IVIG was given subsequently. The response was immediate and platelet count increased to 100,000 per mcL within 48 hours of IVIG administration. IVIG is an immunomodulator and has been used in several autoimmune conditions including Immune Thrombocytopenic Purpura (ITP). However, the mechanism of action of IVIG is not known yet. It has been postulated that it acts in ITP by inhibiting autoantibody adsorption on patient’s platelet, decreasing Fc-receptor mediated platelet destruction anti-idiotypic inhibition of anti platelet antibody [12]. Although a baseline platelet count of the patient was not available, we assume that it was normal as she never had any bleeding manifestations in past.
Conclusion
Thrombocytopenia following dengue fever is well known but is usually transient. Persistent thrombocytopenia after dengue fever is rare and usually responds to steroid therapy. Our patient did not show any response to steroids and recovered after starting IVIG. Better response to IVIG in this case confirms the fact that pathogenesis of thrombocytopenia in dengue is predominantly immunological.
[1]. Mitrakul C, Bleeding problem in dengue haemorrhagic fever: platelets and coagulation changesSoutheast Asian J Trop Med Public Health 1987 18(3):407-12. [Google Scholar]
[2]. Srichaikul T, Nimmannitya S, Haematology in dengue and dengue haemorrhagic feverBailliere’s best practice & research Clinical haematology 2000 13(2):261-76. [Google Scholar]
[3]. Srichaikul T, Disseminated intravascular coagulation indengue haemorrhagic feverThe Southeast Asian Journal of Tropical Medicine and Public Health 1987 18(3):303-11. [Google Scholar]
[4]. Lin CF, Lei HY, Liu CC, Liu HS, Yeh TM, Wang ST, Generation of IgM antiplatelet autoantibody in dengue patientsJ Med Virol 2001 63(2):143-49. [Google Scholar]
[5]. Saito M, Oishi K, Inoue S, Association of increased platelet-associated immunoglobulins with thrombocytopenia and the severity of disease in secondary dengue virus infectionsClinical and Experimental Immunology 2004 138(2):299-303. [Google Scholar]
[6]. Petaja J, Inflammation and coagulation. An overviewThrombosis Research 2011 127(2):S34-S37. [Google Scholar]
[7]. Patil ND, Persistent thrombocytopenia after Dengue haemorrhagic feverIndian Pediatr 2006 43(11):1010-11. [Google Scholar]
[8]. Prashanth GP, Mugali SB, Persistent thrombocytopenia in dengue haemorrhagic feverIndian Pediatr 2011 48(9):737 [Google Scholar]
[9]. Kohli U, Saharan S, Lodha R, Kabra SK, Persistent thrombocytopenia following dengue shock syndromeIndian J Pediatr 2008 75(1):82-83. [Google Scholar]
[10]. Bhalla A, Bagga R, Dhaliwal LK, Sharma R, Varma S, Steroid responsive prolonged thrombocytopenia in dengueIndian J Med Sci 2010 64:90-93. [Google Scholar]
[11]. Mizutani H, Furubayashi T, Imai Y, Kashiwagi H, Honda S, Take H, Mechanisms of corticosteroid action in immune thrombocytopenic purpura (ITP): experimental studies using ITP-prone mice, (NZW x BXSB) F1Blood 1992 79(4):942-47. [Google Scholar]
[12]. Hansen RJ, Balthasar JP, Mechanisms of IVIG action in immune thrombocytopenic purpuraClin Lab 2004 50(3-4):133-40. [Google Scholar]