Isolated Right Ventricular Infarction Mimicking Anterior ST-Segment Elevation
Onur Baydar1, Veysel Oktay2, Ugur Coskun3, Ahmet Yildiz4, Tevfik Gurmen5
1 Instructor, Department of Cardiology, Institute of Cardiology, Istanbul University, Istanbul, Turkey.
2 Instructor, Department of Cardiology, Institute of Cardiology, Istanbul University, Istanbul, Turkey.
3 Instructor, Department of Cardiology, Institute of Cardiology, Istanbul University, Istanbul, Turkey.
4 Instructor, Department of Cardiology, Institute of Cardiology, Istanbul University, Istanbul, Turkey.
5 Professor, Department of Cardiology, Institute of Cardiology, Istanbul University, Istanbul, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Onur Baydar, Instructor, Department of Cardiology, Institute of Cardiology, Istanbul University, Haseki, Aksaray 34350, Istanbul/Turkey.
E-mail: dr.onurbaydar@hotmail.com
Acute coronary syndromes in patients with presence of ST-segment elevation in the anterior precordial leads indicates left anterior descending coronary artery occlusion. However, anterior ST-segment elevation has also been described in right ventricular myocardial infarction and is thought to be due to right coronary artery (RCA) occlusion. We present a rare case of isolated RVMI presenting with anterior ST-segment elevation due to proximal occlusion of a right coronary artery that was treated by primary coronary angioplasty. Primary coronary angioplasty and stenting of this artery was performed resulting in resolution of the chest pain and ST- segment elevation.
Coronary angioplasty, Myocardial infarction, Right ventricle
Case Report
A 60-year-old man with no history of cardiac disease was admitted due to typical chest pain since 1 hour. The initial standard 12-lead electrocardiogram (ECG) showed ST-segment elevation in leads V1-V4 [Table/Fig-1]. On physical examination general health situation was moderate. His heart rate was 98 bpm and blood pressure was 160/80 mmHg. First and second heart sounds were normal. There was no additional heart sound or murmur. Other systemic examinations were unremarkable. The patient was given 5500 U of unfractionated heparin IV, 600 mg clopidogrel oral loading dose and 300 mg oral aspirin, and was transferred to catheterization lab. Coronary angiography showed patent LMCA, CX and LAD [Table/Fig-2]. Proximal occlusion of a nondominant right coronary was detected [Table/Fig-3]. Primer percutaneus coronary intervention was performed to proximal segment of the RCA using a Judkins right (7F JR 4 Cordis Europe, Roden, Holland) guiding catheter and the lession crossed with a balanced middle weight wire. After thrombus aspiration (Diver C.E.MAX), followed by implantation of 3,5 x 12 mm (Ephesos) at 20 atm with exellent angiographic result [Table/Fig-4], the patient’s chest pain resolved and transthoracic echocardiogram showed RV dilation and paradoxical interventricular septal wall motion (tapse : 1.1mm), but no wall-motion abnormalities in the left ventricle. Two days later control transthoracic echocardiogram was performed and RV function was found to be recovered. (tapse: 1.8 mm). The patient was discharged 5 days after coronary stenting in good health status without any cardiac adverse event and currently has no complaints.
ECG showed V1-V4 st segment elevation.

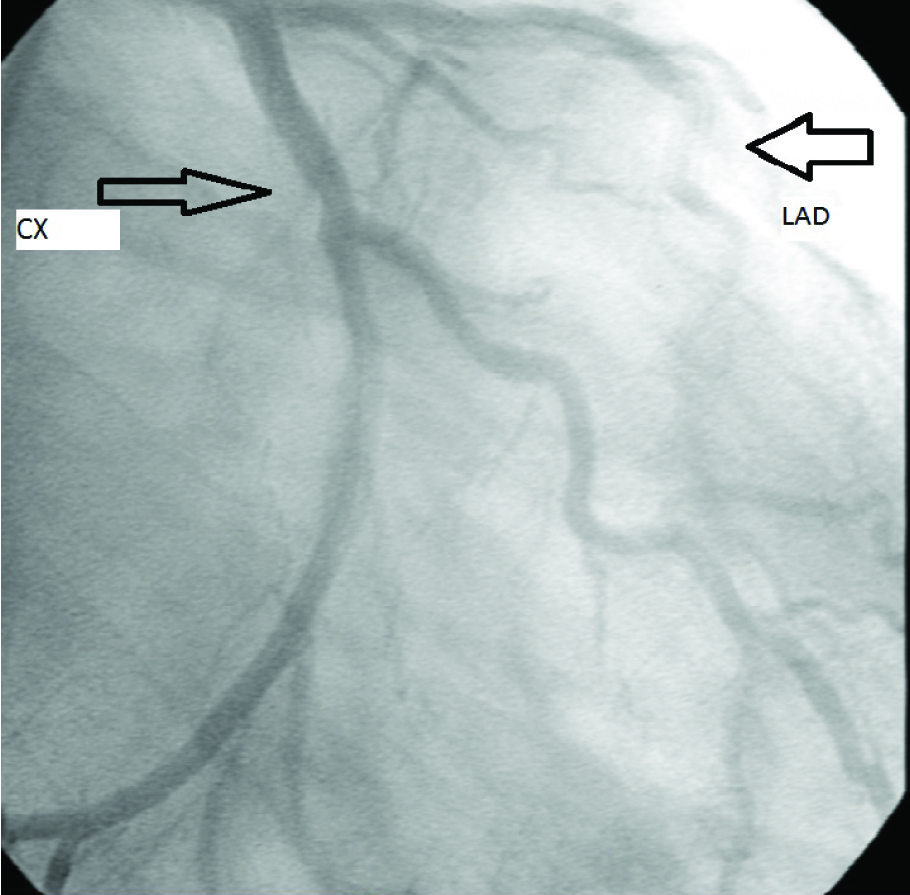
Coronary angiography showed that patent LMCA, CX and LAD.
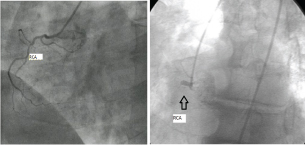
Proximal occlusion of a nondominant right coronary was detected and primer percutaneus coronary intervention was performed to proximal segment of the RCA.
Discussion
The ECG changes in RVMI are ST-segment elevation in the inferior leads with concomitant ST-segment elevation in the precordial leads V3RV4R [1]. When the inferior wall and right ventricle simultaneously become occluded, precordial ST elevation is often not detectable because, the dominant electrical forces of the inferior wall suppress the ECG changes caused by the ischemia of the ventricle [2]. Isolated RVMI occurs in less than 3% of all patients with myocardial infarction [3]. It is described as occlusion of a nondominant RCA [4] and loss of large RV branches during coronary angioplasty of the RCA [5].
Cases of sudden cardiac death [6], as well as those where autopsy confirmed the isolated RVMI [7–9] have also been reported.
ECG features may help differentiate ST-segment elevation secondary to isolated RVMI from left anterior descending artery territory infarction, though not specific. The absence of Q-wave development in the anterior precordial leads may favor the diagnosis of RVMI [1]. In most patients with RVMI, ST-segment elevation in V4R is higher than that found in V1–V3. Kida et al., demonstrated 57 patients undergoing PTCA of the right coronary artery and observed ST elevation in precordial leads caused by occlusion of the right coronary artery when the blood flow in all right ventricular branches was obstructed [10]. They showed that this type of ST elevation in precordial leads is caused by right ventricular ischemia.
Conclusion
The present case of isolated RVMI is an uncommon but important differential diagnosis of anterior ST-segment elevation and highlights the value of careful review of angiographic images. Primary percutaneous intervention of the vessel may cure the chest pain and rectify the ST-segment changes. Thus the damage to RV myocardium can be minimized.
[1]. Geft IL, Shah PK, Rodriguez L, ST elevation in leads V1 to V5 may be caused by right coronary artery occlusion and acute right ventricular infarctionAm J Cardiol 1984 53:991-96. [Google Scholar]
[2]. Yano S, Mikuriya Y, Nasu M, Influence of right ventrivular ischemia on precordial ST depression during right coronary artery occlusionJpn Circ J 1993 57:803-08. [Google Scholar]
[3]. Kinch JW, Ryan TJ, Right ventricular infarctionN Engl J Med 1994 330:1211-17. [Google Scholar]
[4]. Gregory S, Desai A, Fifer M, Isolated right ventricular infarction resulting from occlusion of a nondominant right coronary arteryCirculation 2004 110:500-01. [Google Scholar]
[5]. Hilliard A, Nkomo V, Mathew V, Isolated right ventricular infarction—an uncommon cause of acute anterior ST segment elevationInt J Cardiol 2009 132:51-53. [Google Scholar]
[6]. Rao J, Mascarenhas D, Schiavone J, Nondominant right coronary artery occlusion and ventricular tachyarrhythmiasCatheter Cardiovasc Interv 2002 56:53-57. [Google Scholar]
[7]. Vesterby A, Steen M, Isolated right ventricular myocardial infarction. A case reportActa Med Scand 1984 216:233-35. [Google Scholar]
[8]. Bellamy GR, Hollman J, Isolated right ventricular infarction following percutaneous transluminal coronary angioplastyAm Heart J 1986 111:168-69. [Google Scholar]
[9]. Saw J, Amin H, Kiess M, Right ventricular ischemia mimicking acute anterior myocardial infarctionCan J Cardiol 1999 15:1143-46. [Google Scholar]
[10]. Kida M, Morishita H, Yokoi H, Yoshinaga M, Yasumoto H, Kimura T, Precordial ST-segment elevation caused by right coronary artery occlusionJ Cardiol 1987 17:455-64. [Google Scholar]