Papillary Height and its Relation with Interproximal Distances and Cementoenamel Junction in Subjects with Chronic Periodontitis. A Cross-Sectional Study
Nishi Tanwar1, Satish Chander Narula2, Rajender Kumar Sharma3, Shikha Tewari4
1 Assistant Professor, Department of Periodontics, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
2 Senior Professor, Department of Periodontics, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
3 Professor, Department of Periodontics, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
4 Professor, Department of Periodontics, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nishi Tanwar, B4/2, Sagar Kunj GHS, GH-3, Sec – 9A, Gurgaon, Haryana, India.
E-mail: nsh_tanwar@yahoo.co.in
Introduction
Presence of intact interdental papilla is considered as an essential component of aesthetic dentistry. Loss or absence of interdental papilla creates black triangles which are unpleasing.
Aim
The purpose of the present study was to determine relation of interproximal distances and cementoenamel junction with the classification of interdental papilla recession after surgical exposure in chronic periodontitis patients.
Materials and Methods
This cross-sectional, single masked study group involved 198 interdental papillae in 50 chronic periodontitis patients subjected to open flap debridement. The subjects were divided into three groups according to loss of height of interdental papillae: Class I papilla, Class II papilla, Class III papilla. The interproximal distances included vertical and horizontal distance. The vertical distance was measured from apical point of the contact area to alveolar crest; horizontal distance was measured between roots at the alveolar crest. Distance from mid buccal cementoenamel junction to apical point of the contact area was also measured.
Results
The vertical distance was found to be significantly affecting all the classes of loss of papillary height (p<0.05). Significantly positive correlation was found between vertical distance and buccal cementoenamel junction (p<0.05). On applying multiple linear regressions vertical distance was found to be strongest determinant of loss of papillary height.
Conclusion
Although interproximal distances and cementoenamel junction affect the height of interdental papilla, other factors influencing the existence of interdental papilla should also be taken into consideration for treatment planning to achieve better aesthetics.
Aesthetics, Black triangles, Gingiva, Surgical flap
Introduction
Presence of intact interdental papilla is considered as an essential component of aesthetic dentistry. The interdental papilla not only acts as a biological barrier in protecting the periodontal structures, but also plays an important role in aesthetics. Normally interdental papilla completely fills the gingival embrasures. Open gingival embrasures or “Black triangles” are created due to incomplete fill of interdental papilla. These black triangles results in aesthetic impairment, food retention and phonic problems [1,2]. Various factors can be responsible in the formation of open gingival embrasures. Most common causes include dimensional changes of papilla during orthodontic alignment, loss of periodontal attachment resulting in recession, loss of height of the alveolar bone relative to interproximal contact, length of embrasure area, root angulations, interproximal contact position and triangular shaped crowns and course of cementoenamel junction [1–7].
One must have a clear understanding about all the factors affecting the height and health of interdental papilla to prevent its disappearance.
The interdental space is made by contact area and the interproximal embrasures which are occupied by the interdental papilla [8]. This space can be divided into a vertical dimension between the contact point and the alveolar crest and the horizontal dimension between the mesial and distal surfaces of the adjacent teeth [9]. Studies have related these dimensions with the presence or absence of interdental papilla. Tarnow et al., studied that the interdental papillae are almost always present when the bone crest to contact point distance is ≤5mm (98%), at 6mm distance only 56% papilla was present, at 7mm or more distance papilla was no more than 27% [1]. Cho et al., recorded vertical dimensions and interadicular distances and concluded that at 1mm of interadicular distance 77.8% of interdental papilla were present, the percentage of intact papilla was decreasing with the increase in interadicular distance. It was also found that papilla was always lost when interadicular distance was ≥4mm. They concluded that interdental space have an independent and combined effect on the existence of interproximal papillae [9].
Montevecchi et al., study evaluated different variables including horizontal and vertical distance between central and lateral papilla. Study also correlated clinical classes of papillary recession with the variables [10].
Kolte et al., found 85.7% of intact papilla at vertical distance of 4mm and 78.5% of intact papilla at horizontal distance 0.5mm and 1mm [11].
Studies till date have investigated the interdental papilla and the factors affecting it in terms of its presence or absence [3,9,11–14]. The aim of present study was to investigate the interproximal distances which included the vertical distance from the contact point to alveolar crest, interproximal distance between roots at alveolar crest and distance from buccal cementoenamel junction to contact area and its correlation with the classification system of papillary recession given by Nordland and Tarnow after surgical exposure of the interdental space [15]. The purpose of classifying the loss of height of interdental papilla was to allow easy means to assess progressive degrees of interdental papilla loss using readily observed anatomical landmarks for reference, which can be helpful for better diagnosis and treatment plan.
Materials and Methods
Subjects
This cross-sectional, single masked study was conducted in the Department of Periodontics, Post Graduate Institute of Dental Sciences, Rohtak, India. A total of 250 interproximal sites in 50 patients were selected similar to the previous study done by Cho et al., from Outdoor Patient Department of Periodontics, irrespective of socio-economic status, religion and sex [9]. Patients requiring surgical intervention for the treatment of chronic periodontitis were recruited in this study. Chronic periodontitis (CP) criteria considered for the study were as follows: 1) at least two interproximal sites with attachment loss (AL) ‡4 mm (not on same tooth); or 2) at least two interproximal sites with probing depth (PD) ‡5 mm (not on same tooth) [16].
The present study was approved by institutional review board. Exclusion criteria were Teeth with open contacts, history of periodontal surgery, orthodontic treatment, translocated or tilted teeth proximal/cervical restorations or abrasions, pregnancy, history of taking medications known to increase the risk of gingival enlargement.
Data Collection
The study protocol involved a screening appointment to verify eligibility, followed by etiotropic phase therapy to establish optimal plaque control and gingival health conditions. Teeth with normal contact points were included. Sites with sulcus bleeding index >2 and papillary bleeding index >1 on probing the interdental papilla were excluded as evaluation of papillary height may be influenced by inflammation [17]. On the basis of the classification system as given by Nordland and Tarnow [15], the papillae were assigned into following four groups; Class I papilla, Class II papilla, Class III papilla prior to surgery. To ensure examiner blinding the selection of papilla was done by one examiner (S.N.) and all the measurement were recorded by another single trained examiner (N.T.). A written informed consent was taken from the patient for the same.
Following parameters were measured and recorded after raising the mucoperiosteal flap.
(I) Interproximal Distances.
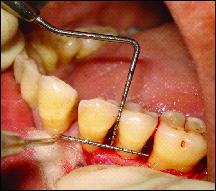
(a) The vertical distance from the contact point to alveolar crest [Table/Fig-1].

The vertical dimension between the alveolar crest and the apical point of the contact area between the teeth was measured with the help of UNC-15 probe (vertical distance).
(b) Interproximal distance between roots at alveolar crest [Table/Fig-2,3].
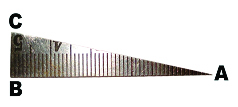
Interproximal distance between roots (horizontal distance)

Modified interproximal ruler with inherent accuracy of 0.2mm was used for measuring interproximal distance between roots (10 mm width X 50 mm length X 0.8 mm thickness) [5]. Interproximal distance was measured by ruler being laid flat and inserted interproximally at alveolar crest (horizontal distance).
(II) Distance from mid buccal cementoenamel junction line of adjacent teeth to apical point of the contact area [Table/Fig-4].
Buccal cementoenamel junction to apical point of contact area
A reference line was made at maximum contour of adjacent mid buccal cementoenamel junction with the help of periodontal probe and the distance from this line to the apical point of the contact area was measured with the help of UNC-15 probe (Hu-Friedy, Chicago, IL).
Each site was measured five times and most frequently measured and recorded number was considered to be the final measurement by the same examiner (N.T.) so as to minimize errors.
Statistical Analysis
Statistical software (SPSS version 17; SPSS, Chicago, IL, USA) was used to analyse the data, which is presented as the mean ± standard deviation. Kruskal wallis was applied for intergroup comparison followed by Mann Whitney test for comparative analysis between the two groups. The spearman correlation was used to measure associations for two variables. To find out high predictor between dependent (interproximal distances) and independent variable (cementoenamel junction), multiple linear Regression was applied. The level of statistical significance was p<0.05.
Results
Although initially a total of 250 papillae were measured. Out of 250 papillae only 198 were involved in the analysis. The number of normal papillae in cases of chronic periodontitis was found very few i.e. approximately 10 which were excluded from the analysis and few papillae were dropped out because of anatomic variations of tooth size like triangular shape of crown etc. Post-hoc calculation showed power > 95% with sample size of 198 in which R2 is equal to 0.184 (regression coefficient) which calculated effect size to be 0.225.
A descriptive analysis of various parameters of different types of interdental papillae is shown in [Table/Fig-5]. Intergroup comparison of various parameters with respect to loss of height of interdental papilla was done by applying Mann-Whitney test, statistically significant results were found in all classes of papilla with the vertical distance (p<0.05). Interproximal distance between roots (Horizontal distance) was statistically significant in class I and class III, class II and class III only (p<0.05). Buccal cemento-enamel junction to contact point was statistically significant only in class II and class III papillae (p<0.05) as shown in [Table/Fig-6]. The spearman correlation was used to measure associations of two variables, a positive significant relation was seen in vertical distance and buccal cemento-enamel junction and a negative significant relation was seen in Interproximal distance between roots (horizontal distance) and buccal cementoenamel junction [Table/Fig-7]. On applying linear regression, vertical distance was found to be the strongest determinant of loss of height of interdental papillae [Table/Fig-8].
| Variable | TYPE I (n=22) | TYPE II (n=157) | TYPE III (n=19) | TOTAL(n=198) |
|---|
| Vertical distance | 6.32± 1.21 | 7.14±1.36 | 8.32±1.25 | 7.16±1.40 |
| Interproximal distance between roots (horizontal distance) | 2.07±0.72 | 2.22±0.72 | 2.69±0.81 | 2.25±0.74 |
| Buccal Cemento Enamel Junction | 4.59±1.14 | 4.78±1.11 | 4.16±0.9 | 4.70±1.11 |
Intergroup Comparison of various parameters (Mann-Whitney test).
| Variable | Type-I PapillaandType-II Papilla | Type-I PapillaandType-III Papilla | Type-II PapillaandType-III Papilla |
|---|
| Vertical distance | 0.01 | <0.01 | <0.01 |
| Interproximal distance between roots (horizontal distance) | NS | 0.01 | 0.02 |
| Buccal Cemento Enamel Junction | NS | NS | 0.02 |
Spearman correlation in between various parameters.
| Parameters | Vertical Distance | Interproximal Distance Between Roots | Buccal Cemento Enamel Junction |
|---|
| Vertical distance | Correlation Coefficient | - | 0.041 | 0.405 |
| Significance(p-value) | - | 0.564 | 0.000 |
| Interproximal distance between roots (horizontal distance) | CorrelationCoefficient | 0.041 | - | -0.354 |
| Significance(p-value) | 0.564 | - | 0.000 |
p < 0.05 significant
Multiple linear Regression between Dependent and Independent variables dependent (interproximal distances) and independent variable (cementoenamel junction).
| Vertical Distance | Interproximal Distance Between Roots (horizontal distance) |
|---|
| Buccal Cemento Enamel Junction | (p) | R2 | (p) | R2 |
| <0.01 | 0.184 | <0.01 | 0.05 |
Discussion
Preserving papilla in the gingival embrasure of the aesthetic zone is a key consideration in restorative and orthodontic treatment. Multidisciplinary approach helps us to maintain appropriate interdental space to create an intact papilla [18]. The purpose of the present study was to analyse the loss of height of interdental papillae and its relation with the interproximal distances and buccal cementoenamel junction. It provides a description of the extent of reduction of papillary height. Studies till date have investigated the interdental papilla and the factors affecting it in terms of its presence or absence. Our study has an edge over these studies as the interdental papilla was analysed in terms of various stages of its gradual loss [15]. We used this classification due to its extreme clarity and clinical practicality. It can easily compare the previous studies [1,9] as it includes important points of anatomical reference that are available on natural teeth.
Moreover in this study, all the parameters were measured by visualizing the alveolar crest and cementoenamel junction after elevating the flap instead of the previous non-invasive technique [3,10,12–14]. The surgical exposure helped in clearer picture of the anatomy of the bone in the interdental area. Modified interproximal ruler with inherent accuracy of 0.2mm [9] was used for measuring interproximal distance between roots (10 mm width X 50 mm length X 0.8 mm thickness). This ruler made an easy access to measure shortest interproximal distance of roots.
Teeth with proper contacts requiring surgical intervention for the treatment of chronic periodontitis were enrolled in the study. Contact areas in the transpositioned and tilted teeth can be difficult to measure, and the denaturation of papillae was expected from the frequent inflammation by food impaction so they were excluded from the study. Areas with previous periodontal surgery were excluded due to possibility of scar formation in the interdental papilla [3]. Orthodontically treated areas were excluded because orthodontic treatment can artificially suppress the interdental soft tissue, deform interdental papilla and reshape the interdental contact area. All the cases included were with horizontal bone loss.
On applying multiple linear regressions vertical distance was found to be strongest determinant of loss of papillary height. These findings concluded that though many factors affect the loss of height of interdental papilla but vertical distance was found to be strongest determinant of loss of papillary height. This finding was in accordance with the study done by Kolte et al., [11]. This can be explained on the basis that, the soft tissue have a tendency to recede with the bone loss and the interdental bone height is the main factor determining loss of height of interdental papilla with class-I (6.32± 1.21), class II (7.14±1.36), class III (8.32±1.25). A statistically significant difference was seen for interproximal distance between roots at alveolar crest (horizontal distance) in between class II and class III papillae and class I and class III papillae respectively. Difference in horizontal distance with class I and class II papillae were non-significant, other factors might be influencing the loss of height of interdental papillae from Class I to Class II such as close proximity of root surfaces, length of embrasure area, etc. Significantly positive correlation was found between vertical distance and buccal cementoenamel junction while a significant negative relation was seen in horizontal distance and buccal cementoenamel junction.
Most of the studies have evaluated the above parameters in respect to maxillary incisors region only so as to reduce anatomical variability in distinct areas. This can limit the results to particular area and moreover there is requirement to treat multiple interdental sites. The current study evaluated anterior as well as posterior region simultaneously so as to reflect the overall opinion about interproximal embrasures as a whole. Individual interdental space must be studied and not only incisors but the teeth involved up to the smile line.
Periodontal tissues make an important contribution in maintaining beautiful and harmonious smile. Loss of interdental papilla plays an important role in this. Vertical bone loss is found to be the most significant factor in prediction of black triangles. Our study correlated the vertical distance with the classification system which found statistically significant relation i.e., class-I (6.32± 1.21), class II (7.14±1.36), class III (8.32±1.25) respectively. These findings can be helpful in easy prediction of interdental space dimensions of different type of papillary recession with readily observed clinical landmarks and its management [16]. A thorough understanding of anatomic form of interdental space helps in predicting long term success in papilla regenerative procedures [19–22].
Limitations
The present study evaluated only one ethnic group. The study could be done to compare the smokers and non smokers and including the socioeconomic status with large sample size. Further comprehensive studies are needed which would explore the interdental space and the other factors exploring this area, including the limitations of the present study.
Conclusion
In the present study, vertical distance was found to be strongest determinant of loss of papillary height. The findings of the study suggest that though many factors affect the loss of height of interdental papilla but vertical distance was found to be strongest determinant of loss of papillary height. Although interproximal distances and cementoenamel junction affect the height of interdental papilla, other factors influencing the existence of interdental papilla should also be taken into consideration for treatment planning to achieve better aesthetics.
p < 0.05 significant
[1]. Tarnow DP, Magner AW, Fletcher P, The effect of the distance from the contact point to the crest of the bone on the presence or absence of the interproximal dental papillaJournal of Periodontology 1992 63:995-96. [Google Scholar]
[2]. Prato GP, Rotundo R, Cortellini P, Tinti C, Azzi R, Interdental papilla management: a review and classification of the therapeutic approachesInt J Periodont Restor Dent 2004 24:246-55. [Google Scholar]
[3]. Choquet V, Hermans M, Adriaenssens P, Daelemans P, Tarnow DP, Malevez C, Clinical and radiographic evaluation of the papilla level adjacent to single- tooth dental implants. A retrospective study in the maxillary anterior regionJ Periodontol 2001 72:1364-71. [Google Scholar]
[4]. Kurth JR, Kokich VG, Open gingival embrasures after orthodontic treatment in adults: prevalence and etiologyAm J Orthod Dentofacial Orthop 2001 120:116-23. [Google Scholar]
[5]. Gastaldo JF, Curry PR, Syndyk WR, Effect of the vertical and horizontal distances between adjacent implants and between a tooth and an implant on the incidence of interproximal papillaJ Periodontol 2004 75:1242-46. [Google Scholar]
[6]. Zetu L, Wang HL, Management of interdental/interimplant papillaJ Clin Periodontol 2005 32:831-39. [Google Scholar]
[7]. Cardarpoli D, Re S, Interdental papilla augmentation procedure following orthodontic treatment in a periodontal patientJ Periodontal 2005 76:655-61. [Google Scholar]
[8]. Takei HH, The interdental spaceDent Clin N Am 1980 24:169-76. [Google Scholar]
[9]. Cho HS, Jang HS, Kim DK, Park JC, Kim HJ, Choi HS, The effects of interproximal distance between roots on the existence of interdental papillae according to the distance from the contact point to the alveolar crestJournal of Periodontolgy 2006 77:1651-57. [Google Scholar]
[10]. Montevecchi M, Checchi V, Piana L, Checchi L, Variables affecting the gingival embrasure space in aesthetically important regions: differences between central and lateral papillaeOpen Dent J 2011 5:126-35. [Google Scholar]
[11]. Kolte AP, Kolte RA, Mishra PR, Dimensional Influence of Interproximal Areas on Existence of Interdental PapillaeJ Periodontal 2014 85:795-801. [Google Scholar]
[12]. Chang LC, The association between embrasure morphology and central papilla recessionJ Clin Periodontol 2007 34:432-36. [Google Scholar]
[13]. Chang LC, Assesment of parameters affecting the presence of the central papilla using a non-invasive radiographic methodJ Periodontol 2008 :603-09. [Google Scholar]
[14]. Lee DW, Kim CK, Park KH, Cho KS, Moon IS, Non-invasive method to measure the length of soft tissue from the top of the papilla to the crestal boneJ Periodontol 2005 76:1311-14. [Google Scholar]
[15]. Nordland WP, Tarnow DP, A classification system for loss of papillary heightJournal of Periodontology 1998 169:1124-26. [Google Scholar]
[16]. Page RC, Eke PI, Case definitions for use in population based surveillance of periodontitisJ Periodontol 2007 78(Suppl 7):1387-99. [Google Scholar]
[17]. Saxer UP, Muhlemann HR, Motivation and education (in german)SSO Schwetz Monatsschr Zahnheilkd 1975 85:905-19. [Google Scholar]
[18]. Sharma AA, Park JH, Esthetic considerations in interdental papilla: remediation and RegenerationJ Esthet Restor Dent 2010 22:18-30. [Google Scholar]
[19]. Beagle JR, Surgical reconstruction of interdental papilla: case reportInt J Periodont Restor Dent 1992 12:145-51. [Google Scholar]
[20]. Han TJ, Takei HH, Progress in gingival papilla reconstructionPeriodontol 2000 1996 11:65-68. [Google Scholar]
[21]. Blatz MB, Hurzeler MB, Strub JR, Reconstruction of the lost interproximal papilla-presentation of surgical and non-surgical approachesInt J Periodont Restor Dent 1999 19:395-406. [Google Scholar]
[22]. Azzi R, Etienne D, Carranza F, Surgical reconstruction of the interdental papillaInternational Journal of Periodontics & Restorative Dentistry 1998 18:467-73. [Google Scholar]