Unusual Finding in the Inguinal Canal: Abdominal Tuberculosis Presenting as Inguinal Hernia
Priya Dhandore1, Narendra Narayan Hombalkar2, Mohd Hamid Shafique Ahmed3
1 Assistant Professor, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
2 Associate Professor, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
3 Assistant Professor, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mohd. Hamid Shafique Ahmed, Assistant Professor, Department of Surgery, Government Medical College, Miraj-416416, Maharashtra, India.
E-mail: khanmohdhamid@gmail.com
Abnormal findings in the inguinal canal during Herniotomy are not very rare for a paediatric surgeon. These abnormal findings may range from opposite gender sex organ (e.g. uterus and fallopian tube during orchidopexy) to unexpected malignancy (e.g. Rhabdomyosarcoma) to the abnormal embryological development (Splenogonadal fusion). Though abdominal tuberculosis is common, abdominal tuberculosis presenting as an inguinal hernia is exceedingly uncommon. We report an unusual case of abdominal tuberculosis presenting as inguinal hernia.
Ascitic fluid, Herniotomy, Tubercular peritonitis
Case Report
A seven-year-old boy presented to surgical outpatient department for right sided inguino-scrotal swelling. On clinical examination the boy had a right sided inguinal hernia which was reducible. There were no other positive findings and no other significant medical history. His chest x-ray done for the pre anaesthetic evaluation was normal. He was medically fit and underwent right sided Herniotomy.
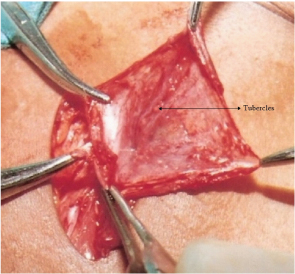
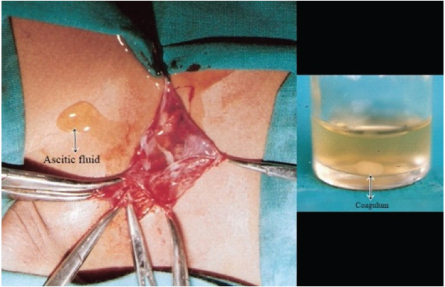
During surgery it was found that the hernial sac was quite thick and nodular. The sac was separated from the cord structures and opened. The peritoneal surface of the sac was studded with very fine to medium sizes tubercles suggesting tubercular involvement [Table/Fig-1]. There was presence of excessive amount of peritoneal fluid which kept on coming from the peritoneal open end of the sac. The peritoneal fluid was collected and it formed coagulum on standing [Table/Fig-2]. The intestinal loops which were near the internal ring were drawn outside and inspected, apparently they were normal. No other gross abnormality was found. The sac was meticulously doubly ligated. The redundant sac was excised and sent for histopathology. The spermatic cord was grossly normal and was not thickened. The right testicle was delivered into the wound from the incision and the tunica was opened. Grossly the right testis was normal. Postoperative recovery was uneventful. Histologically the redundant sac showed multiple epitheloid granuloma with Langhan’s type giant cells, characteristic of tuberculosis. Postoperatively ESR was done which was 95mm at the end of first hour. Ascitic fluid was exudative in nature with predominance of lymphocytes. Urine was collected and it was negative for Acid Fast Bacilli. Andominal Ultrasound was done which was normal. The patient was put on multi drug antitubercular therapy (Rifampacin, Isoniazide, Pyrazinamide and Ethambutol) and was free of disease when seen nine months after surgery.
Intraoperative image showing small to medium sized tubercular nodules over the hernia sac.
Intraoperative image showing ascitic fluid over the hernia sac with coagulum containing ascitic fluid in the test tube.
Discussion
Abdominal Tuberculosis (ATB) is one of the common forms of extra pulmonary tuberculosis. ATB includes tuberculosis of gastrointestinal tract, peritoneum, omentum, mesentery, lymph nodes and solid intra-abdominal organs like liver, spleen, and pancreas. Three varieties of chronic tubercular peritonitis have been described, namely ascitic type, encysted (loculated) type and fibrous type [1]. Abnormal findings in the inguinal canal during the operation of Herniotomy are not very rare for a paediatric surgeon. These abnormal findings may range from opposite gender sex organ (e.g. uterus and fallopian tube during orchidopexy) to unexpected malignancy (e.g. Rhabdomyosarcoma) to the abnormal embryological development (Splenogonadal fusion) [2]. ATB is still a common entity in Indian subcontinent. Among the varied manifestation of ATB, presentation as an inguinal hernia is not common. English literature search had revealed only a few case reports [3–11]. Ascitic form of tubercular peritonitis is supposed to be of the milder form due to strong host resistance. The disease is insidious in onset. Pain is conspicuous by its absence. Clinical or subclinical ascites is reported in virtually all patients with tubercular peritonitis and is frequently the presenting feature. The most common form of abdominal tuberculosis is wet type (Ascitic) Peritonitis. In these cases ascites may be localized or generalised throughout the peritoneal cavity. Multiple tubercles are present on both the layers of peritoneum. A congenital inguinal hernia is the manifestation of patent processus vaginalis (continuation of peritoneum in the inguinal canal). The tubercular pathology which affects primarily the peritoneum, can affect the hernia sac which can be encountered during routine herniotomy operation. The excessive amount of abdominal fluid causes raised intra abdominal pressure and can itself be the cause of the inguinal hernia or sometimes the umbilical hernia [1]. The tubercular ascitic fluid may also trickle down to the patent processus vaginalis and will be picked up during herniotomy. Tuberculous peritonitis can be diagnosed by abdominal ultrasound or CT to detect ascites and lymphadenopathy with or without diffuse thickening of the peritoneum, mesentery and/or omentum. Ascitic fluid is typically a straw coloured (protein>25-30g/l) with white cell (> 500mm3) and (lymphocytes >40%). Unfortunately, diagnostic smears for acid fast bacilli are diagnostic in only < 3% of patient and culture may take upto 4-8 weeks. Laparoscopy and peritoneal biopsy is perhaps the most effective method of diagnosing tuberculous peritonitis. Multiple epitheloid granuloma with Langhan’s type giant cells on histopathology clinches to the diagnosis of tuberculosis. With wider prevalence of HIV and the subsequent increase in infections like tuberculosis, testing for HIV may be appropriate. Management is principally supportive (nutrition and hydration) and medical (systemic multidrug antitubercular therapy) although surgery may be required for specific complication such as intestinal obstruction due to strictures, adhesions or perforation [12].
Conclusion
A good clinical systemic examination especially of abdomen for the presence of ascites or palpable nodal masses or thickened bowel loops can give clue towards abdominal tuberculosis as the cause of hernia in selected cases. Many times during herniotomy the hernial sac is merely twisted and ligated from outside without its inspection from inside. Also the hernia sac is not routinely subjected to histopathological examination. This case highlights the importance of thorough inspection of the hernial sac and of tissue diagnosis of the hernial sac if it appears abnormal or associated with ascites. If confirmed as abdominal tuberculosis it should be treated with standard multidrug antitubercular regimen.
[1]. Tewari M, Sahoo SP, Shukla HS, Abdominal Tuberculosis. In: Surendra K.Sharma, Alladi Mohan, editorsTuberculosis 2009 2nd editionIndiaJaypee Brothers Medicalpublishers (P) LTD:275-79. [Google Scholar]
[2]. Bloom DA, Wan J, Key D, Disorders of the male external genitalia and inguinal canal. In: Kelalis PP, King LR, Belman AB, et alClinical Pediatric Urology 1992 3rd editionPhiladelphiaWB Saunders:1015-49. [Google Scholar]
[3]. Narasimharaw KL, Pradeep R, Mitra SK, Pathak IC, Abdominal tuberculosis presenting as inguinal herniaIndian Pediatr 1983 20:790-91. [Google Scholar]
[4]. Taylor BA, Tuberculous peritonitis presenting in a hernial sacJ R Coll Surg Edinb 1986 31(5):313-15. [Google Scholar]
[5]. Faccin M, Youssef SR, Mozetic V, Catapani WR, Inguinal hernia incarceration as a form of intestinal tuberculosisSao Paulo Med J 1996 114(1):1097-99. [Google Scholar]
[6]. Rao BJ, Kabir MJ, Varshney S, Richter’s hernia: a rare presentation of abdominal tuberculosisIndian J Gastroenterol 1999 18(1):33 [Google Scholar]
[7]. Bhatia S, George RK, Sharma R, Abdominal tuberculosis presenting as an inguinal herniaTrop Gastroenterol 2005 26(2):98 [Google Scholar]
[8]. Basrur GB, Naik RP, Doctor NH, Primary presentation of abdominal tuberculosis in an inguinal herniaIndian J Surg 2006 68(3):174-75. [Google Scholar]
[9]. Lazarus J, Pillay K, Abdominal tuberculosis presenting as an inguinal hernia in a childUrology 2011 77(6):1470-71. [Google Scholar]
[10]. Vashist M, Singhal N, Verma M, Deswal S, Mathur S, Abdominal Tuberculosis In A Hernial Sac: A Rare PresentationThe Internet Journal of Surgery 2012 28(2):1-3. [Google Scholar]
[11]. Dewanda NK, Midya M, Rai NN, Hernial Sac Tuberculosis- An Unusual Presentation of Gastrointestinal Tuberculosis: Case Report with Review of LiteratureIJSRP 2014 4(2):1-3. [Google Scholar]
[12]. Knowles CH, The peritoneum, omentum, mesentry and retroperitoneal space. In: Williams N S, Bulstrode J.K. C, O’Connell P.R. editorsBailey & Love’s Short Practice of Surgery 2013 26th editionGreat BritainCRC Press, Taylor & Francis Group:976 [Google Scholar]