Ileo-Colic Burkitt Lymphoma in a Young Adult Female- A Case Report
Mima Maychet B. Sangma1, Simon D Dasiah2, Aju James Ashok3
1 Associate Professor, Department of General Surgery, Indira Gandhi Medical College & Research Institute, Pondicherry, India.
2 Professor and Head, Department of General Surgery, Indira Gandhi Medical College & Research Institute, Pondicherry, India.
3 Junior Resident, Department of General Surgery, Indira Gandhi Medical College & Research Institute, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mima Maychet B. Sangma, Flat No. 51, Sree Nivas Towers Kathirkamam, Vazhudavur Road, Kathirkamam, Pondicherry-605009, India.
E-mail: mimamaychet@gmail.com
Burkitt’s lymphoma is an uncommon and aggressive type of Non-Hodgkin’s lymphoma and is one of the fastest growing cancer tumour in humans; growth fraction close to 100%. We report a case of a young adult female presented with acute pain abdomen with ileo-caecal mass. On clinical presentation, initial diagnosis was acute appendicitis with lump formation. Ultrasound reported as diffuse inflammatory changes and later CECT was done which reported as Gastro-Intestinal Stromal Tumour (GIST). On laparotomy, a huge hard mass was found on ileo-caecal region and right hemicolectomy was done. Diagnosis was confirmed as Non-Hodgkins Burkitt’s Lymphoma by HPE and immunohistochemistry testing. So, careful workup is the key to initiate early treatment. This patient had complete remission after the right hemicolectomy followed by multiagent chemotherapy.
Acute appendicitis, Ileo-caecal mass, Non-hodgkin’s lymphoma, Primary gastrointestinal tumour
Case Report
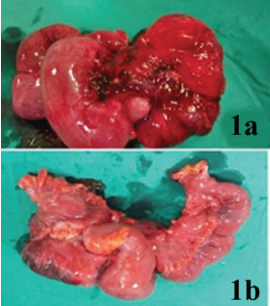
A 27-year-old woman presented with right lower quadrant pain abdomen for 2-months. The pain aggravated one week prior to presentation and was associated with fever and vomiting. On examination right iliac fossa lump was felt which was initially thought to be acute appendicitis with lump formation. USG reported diffuse inflammatory changes involving terminal ileum, caecum and ascending colon. Appendix was not visualized separately. CECT showed lobulated thick walled lesion in the ileo-caecal junction suggesting GIST (Gastro-intestinal-stromal-tumours). On laparotomy, a hard diffuse lump in the ileo-caecal region, caecum and ascending colon were found coiled and pulled up. We proceeded with right hemicolectomy [Table/Fig-1a,b].
/b> A right hemicolectomy specimen with hard diffused lump involving terminal ileum, caecum, appendix and ascending colon.
The specimen was sent for HPE and the opened specimen of terminal ileum, along with appendix and distorted caecum reported thickening of the wall with a firm white appearance of tumour. The rest of the ascending colon mucosa appeared unremarkable.
Microscopic findings showed sections of walls of ileum, appendix, meso-appendix and caecum reported transmural infiltration composed of sheets of medium sized cells with round, mildly mitotically active nuclei, clumped formation and 2-3 prominent nuclei [Table/Fig-2a,b]. The tumour also reported infiltration of cells with mesenteric adipose tissue and 3 positive lymph nodes in peri-ileal and peri-caecal-adipose tissue. Ileal surgical margin was free of tumour.
/b> HPE of burkitt lymphoma showing tumour cells stained with (2a) CD20 tumour marker for mature B-Cells, with a Ki-67 index of 95% (2b) H&E Stain with round mildly mitotically active nuclei, clumped formation (10x).

Immunohistochemistry test reported tumour cells positive for B-Cell Marker (CD-20), with a Ki-67 index of 95%. HPE reported high grade B-cell Non-Hodgkin’s Burkitt lymphoma.
Discussion
Burkitt’s Lymphoma is an uncommon and aggressive form of Non-Hodgkin’s lymphoma in adults. Burkitt’s lymphoma accounts for 40% of all childhood Non-Hodgkin’s lymphoma and it represents only <5% of lymphoma cases in adults [1]. Therefore there are fewer reports on the outcome of Burkitt patients in adult than in paediatric series.
The three variants of Burkitt’s lymphoma which has been recognised are endemic, sporadic (non-endemic) and immunodeficient [2]. Sporadic Burkitt’s Lymphoma consists of 1-2% in adult Non-Hodgkin’s lymphoma. Most patients with Burkitt’s Lymphoma in United States present with bulky abdominal mass, B-Symptoms and laboratory evidence of tumour lysis [3].
In abdomen the ileo-caecal region is the most presenting site;the ovaries, kidneys also have been reported in some patients [4]. Sporadic Burkitt’s lymphoma has a predilection for involving the abdomen. Abdominal symptoms are frequent initial complaint in Burkitt’s lymphoma. However acute surgical abdomen is a rare presentation. Our patient presented with an acute pain abdomen with fever and vomiting with localized ileo-caecal mass. Though Burkitt’s Lymphoma is more common in children, adult presentation in very rare and incidence of Burkitt’s Lymphoma is even more lesser in female than in male. In the present study, our patient is an adult female who presented at the age of 27-years with acute pain abdomen, which is a rare presentation. We proceeded with right hemicolectomy with colonic and ileal margins free of tumour cells followed by chemotherapy. Patient had uneventful recovery and follow up CT scan even after 1-year shows no recurrence of tumour.
Dunning et al., also presented with signs and symptoms of colonic ischaemia presenting from lymphoid infiltration of the bowel wall [5]. In a study done by Fuat I et al., a 13-year old boy also presented with ileo-caecal mass and acute pain abdomen on right iliac fossa [6]. His initial clinical presentation was diagnosed as acute appendicitis with lump formation but later on huge caecal mass was found on laparotomy. Final HPE findings revealed Burkitt’s Lymphoma which is similar to our presentation.
Sharath KKL et al., had similar presentation in a 20-year-old male presented as ileo-caecal mass with intussusceptions [7]. On laparotomy, with high suspicion of malignancy, right hemicolectomy was done and later HPE and immunohistochemistry reported as Non-Hodgkin’s Burkitt Lymphoma.
Verma SK et al., in their study reported that primary modality of treatment is multi agent systemic chemotherapy [8]. Goncalves JP et al., found similar findings as the present study with the initial clinical presentation diagnosed as acute appendicitis [9]. They concluded that histology is the gold standard in confirming the diagnosis. Complete surgical excision of small tumour of Burkitt’s Lymphoma can cure the disease followed by chemotherapy. But if there is an extensive involvement of the tumour in the abdomen, limited biopsy and multi agent chemotherapy is sufficient [5].
Conclusion
Burkitt lymphoma is one of the fastest growing cancer of humans and is considered to be medical emergencies requiring immediate diagnostic and therapeutic intervention. Initial clinical presentation can bring diagnostic dilemma as it mimicked other syndromes. So careful workup is important to initiate right treatment and investigation of choice for Burkitt lymphoma remains the pathologic and immunohistochemistry testing.
[1]. Bishop BC, Koneti RV, Wilson WH, Burkitts Lymphoma:molecular pathogenesis and treatmentCancer invest 2000 18:574-83. [Google Scholar]
[2]. Blum KA, Lozanski G, Byrd JC, Adult Burkitt Leukemia and LymphomaBlood 2004 104:3009-20. [Google Scholar]
[3]. Kian TC, Miriam T, Richard Q, Clinical characteristics, prognostic factors and outcomes of Burkitt lymphoma in adult AsiansLeuk Lymphoma 2008 49:824-27. [Google Scholar]
[4]. Ferry JA, Burkitts lymphoma: clinic pathological features and differential diagnosisOncologist 2006 11:375-83. [Google Scholar]
[5]. Dunning K, Mattei P, Burkitts lymphoma presenting as colonic ischaemia and overwhelming sepsisJ Pediat Surg 2007 42:e15-17. [Google Scholar]
[6]. Fuat I, Yahya C, Gunnur G, Umit B, An uncommon Burkitt’s Lymphoma form with ileocecal localisation that presents as appendicular massInsight Surgery 2015 1(1):1-3. [Google Scholar]
[7]. Sharath KKL, Abhishek V, Ramya Y, Mallikarjuna MN, Ileocaecal intussusception secondary to Burkitt’s LymphomaInternational Journal of Biomedical and Advance Research 2013 4(5):275-79. [Google Scholar]
[8]. Verma SK, Neha Burkitt lymphoma: Thorax to PelvisAustin J Clin Case Report 2014 1(9):1044 [Google Scholar]
[9]. Goncalves JP, Cerqueira A, Antunes H, Maia I, Carvalho S, Ileocaecal Burkitt’s lymphoma presenting as acute appendicitis: A case reportInternational Journal of Case Reports and Images 2012 3(11):32-34. [Google Scholar]