Spindle Cell Carcinoma of Nasal Cavity- A Case Report
Priyank Mistry1, Abhishek Mittal2, Tapan Nagpal3
1 PG Resident, Department of ENT, Sumandeep Vidyapeeth, Vadodara, Gujarat, India.
2 PG Resident, Department of ENT, Sumandeep Vidyapeeth, Vadodara, Gujarat, India.
3 Professor, Department of ENT, Sumandeep Vidyapeeth, Vadodara, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priyank Mistry, PG Resident, Department of ENT, Dhiraj Hospital, Sumandeep Vidyapeeth, At & Po. Piparia, Tal-Waghodia, Vadodara-391760, Gujarat, India.
E-mail: priyankmistry_09@yahoo.co.in
Spindle Cell Carcinoma (SpCC), also known as Sarcomatoid Carcinoma, is a rare and peculiar biphasic malignant neoplasm that occurs mainly in the upper aero-digestive tract, mostly in larynx. SCC accounts for 3% of all squamous cell carcinomas (SCCs) in the head and neck region. It is a rare variant of SCC which shows spindled or pleomorphic tumour cells simulating a true sarcoma. We present a case report of SpCC nasal cavity in a 50-year-old female patient, presented with intermittent epistaxis from left nasal cavity. On physical examination, the patient had an ulcero-exophytic type of mass in the left nasal cavity and a smooth bulge on the left side of anterior hard palate. Patient underwent excision of nasal mass along with partial palatectomy by facial degloving approach and reconstruction of palate with naso-labial flap. The postoperative histopathological report showed SCC. Surgery forms the mainstay of treatment. Radiotherapy and Chemotherapy is warranted in order to improve treatment results. As only few cases have been reported, we report a case of this rare entity to contribute for better understanding and awareness of this rare malignancy.
Facial degloving, Naso labial flap, Radiotherapy and chemotherapy, Sarcomatoid carcinoma
Case Report
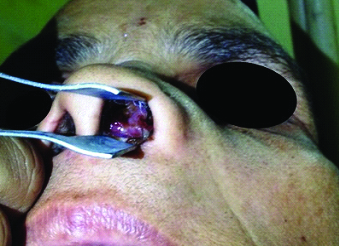
A 50-year-old female reported with the complaints of epistaxis since 1 year and left side nasal obstruction since 3 months. Epistaxis was only from left nasal cavity, intermittent, scanty in quantity, 3-5 episodes in a month. Nasal obstruction was progressive, bilateral, left more than right. There was no history of substance addiction. On anterior rhinoscopy, there was a single pale fleshy mass in left nasal cavity pushing the septum towards right [Table/Fig-1]. On throat examination, there was a smooth bulge on the anterior part of hard palate on left side measuring approximately 2cm x 2cm [Table/Fig-2]. On palpation, the mucoperiosteum over the bulge was intact but with bony erosion. There was no significant cervical lymphadenopathy.
On anterior rhinoscopy, fleshy mass present in left nasal cavity.
Smooth bulge present on anterior part of hard palate.

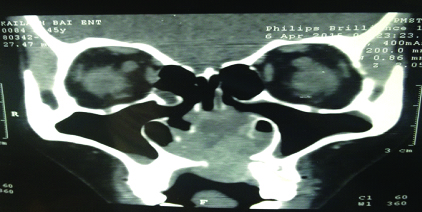
Computed Tomography (CT) of PNS with contrast showed heterogeneously enhancing soft tissue density mass in left nasal cavity with erosion of anterior half of the hard palate, anterior nasal spine and lower part of nasal septum anteriorly and abutting medial wall of left maxillary sinus [Table/Fig-3]. Preoperative biopsy showed the nasal mass to be spindle cell carcinoma.
CT PNS with contrast showing heterogeneously enhancing soft tissue density mass in left nasal cavity.
The patient underwent excision of nasal mass along with partial palatectomy by Facial degloving approach and reconstruction of palate with naso-labial flap under general anaesthesia. The mass was ulcerative, well- circumscribed, and fixed to mucoperiosteum of nasal septum extending to hard palate and left maxilla.
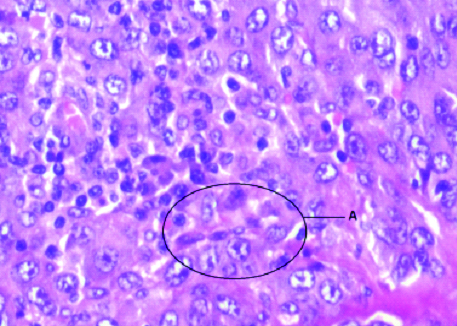
Postoperative histopathological report shows hyperplastic stratified squamous epithelium. Anaplastic cells arranged in spindly and sheet of cells configuration [Table/Fig-4]. Individual tumour cells shows nuclear atypia, pleomorphism, high N:C ratio, prominent nucleoli and mitotic figures.
Postoperative histopathological slide showing sheets of cells with spindly configuration (A).
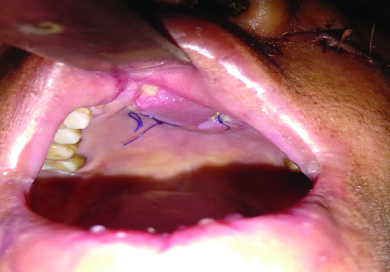
Routine follow up examination at 1 month showed no recurrence of growth and naso-labial flap was also well taken up [Table/Fig-5,6].
Postoperative image showing healthy suture site on follow up.

Postoperative image showing healthy flap in situ on follow up.
At last follow up, at 6 months, patient had complaints of watering from left eye probably due to obstruction of normal drainage through left naso-lacrimal duct at the level of left inferior turbinate, due to wide surgical excision. Patient was advised left endoscopic dacryocystorhinostomy for the same.
Discussion
Spindle cell carcinoma (SPCC) is a biphasic tumour, composed of a SCC, could be insitu and/or invasive. It could also show malignant spindle cell appearance, with a mesenchymal appearance, but, it is of epithelial origin. Out of all SCC in head and neck region, it accounts only for 3% [1]. Sarcomatoid tumour has been classified (according to WHO classification of tumours of the oral cavity and oropharynx) under malignant epithelial tumours of Squamous Cell Carcinoma (SCC) and labelled it “Spindle cell carcinoma” (SpCC) [2]. Histopathologically, sarcomatoid carcinoma is a mixture of both carcinoma and sarcoma consisting of differential mesenchymal tissues. SPCC of nasal cavity is observed more commonly in the age group of fifth to sixth decade, with male preponderance (85%) and strongly associated with smoking and alcohol consumption [3]. Our case was of 50-year-old female with no history of addiction to any substance.
The common sites of involvement are larynx (particularly the vocal cords) and hypo pharynx [4]. Less common sites include the oropharynx, sinuses, and nasal cavity [5–7]. In our case patient had spindle cell carcinoma of nasal cavity.
Clinically they tend to present at locally advanced stage, with most tumours being T3 or T4 at presentation and pursuing an aggressive course [8]. At the time of presentation our patient had T3 tumour with no cervical lymphadenopathy.
Review of literature shows such type of tumour to be managed by wide local excision along with radiotherapy and/or chemotherapy [9,10]. We removed the nasal mass by wide excision, partial palatectomy by facial degloving approach and reconstruction with naso-labial flap.
If the patient presents at advanced stage, then surgery is not feasible. In such cases alternative treatment plan would be chemotherapy or radiotherapy. Cisplastin based chemotherapy could be tried as a part of newer alternative strategy [11].
Conclusion
SpCC is a rare yet aggressive tumour associated with poor prognosis. Literature does not show any definite treatment protocols. Our experience is that surgical excision of such tumour should be done followed by radiotherapy or chemotherapy if required to improve overall treatment results.
[1]. Viswanathan S, Sarcomatoid (spindle cell) carcinoma of the head and neck mucosal region: a clinicopathologic review of 103 cases from a tertiary referral cancer centreHead Neck Pathol 2010 4(4):265-75. [Google Scholar]
[2]. Parikh N, Desai N, Spindle cell carcinoma of the oral cavity: A case report of a rare entity and by review of literatureJ academy Adv Dental Research 2011 2:31-36. [Google Scholar]
[3]. Thompson LD, Wieneke JA, Miettinen M, Heffner DK, Spindle cell (sarcomatoid) carcinomas of the larynx: a clinicopathologic study of 187 casesAm J Surg Pathol 2002 26:153-70. [Google Scholar]
[4]. Oktay M, Kokenek-Unal TD, Ocal B, Saylam G, Korkmaz MH, Alper M, Spindle cell carcinoma of the tongue: a rare tumor in an unusual locationPathol Res Int 2011 2011:572381:1-6. [Google Scholar]
[5]. Leventon GS, Evans HL, Sarcomatoid squamous cell carcinoma of the mucous membranes of the head and neck: a clinicopathologic study of 20 casesCancer 1981 48:994-1003. [Google Scholar]
[6]. Lewis JE, Olsen KD, Sebo TJ, Spindle cell carcinoma of the larynx: review of 26 cases including DNA content and immunohistochemistryHum Pathol 1997 28:664-73. [Google Scholar]
[7]. Ellis GL, Langloss JM, Heffner DK, Hyams VJ, Spindle-cell carcinoma of the aerodigestive tract. An immunohistochemical analysis of 21 casesAm J Surg Pathol 1987 11:335-42. [Google Scholar]
[8]. Howard SN, Bond WR, Hong IS, Foss RD, Right maxillary sinus sarcomatoid carcinoma (sarcomatoid/spindle cell carcinoma)Otolaryngol Head Neck Surg 2007 137:355-57. [Google Scholar]
[9]. Ahluwalia H, Gupta SC, Gupta SC, Pathology in focus: spindle-cell carcinoma of the nasal septumJ Laryngol Otol 1996 110:284-87. [Google Scholar]
[10]. Terada T, Kawasaki T, Spindle cell carcinoma of the nasal cavityInt J Clin Oncol 2011 16:165-68. [Google Scholar]
[11]. Sadaba LM, García-Layana A, Garcia-Gomez PJ, Salinas-Alaman A, Sarcomatoid carcinoma and orbital apex syndromeEur J Ophthalmol 2006 16:608-10. [Google Scholar]