Hyperlipidemia is a major cause of atherosclerosis and atherosclerosis associated conditions, such as coronary heart disease (CHD), ischaemic cerebrovascular disease and peripheral vascular disease. CHD causes more death (25-30%), disability and incurs great economic costs than any other illness in the developed world [1,2]. It is estimated that there were approximately 29.8 million patients with CHD in India during the year 2003 [3]. Compared to all other countries, India suffers the highest loss in potentially productive years of life, due to deaths from CHD in people aged 35-64 years [3]. The prevalence of CHD is reported to be 2-3 times higher in the urban population as compared to the rural population. These statistics illustrate the importance of identifying and managing risk factors of CHD [3].
Hypercholesterolaemia and low levels of high-density-lipoprotein cholesterol (HDL-C) are the major causes of increased atherogenic risk [1]. The association between the elevated serum cholesterol and atherosclerotic disease was first reported in 1930 [4]. In the Multiple Risk Factor Intervention Trail (MRFIT) [5], the relationship between serum cholesterol level and subsequent CHD was found to be continuous graded and strong. As opposed to the atherogenic potential of IDL and LDL, HDL particles are protective against atherosclerotic plaque formation. High HDL-C levels are associated with lower incidence of CHD. This is as a result of capacity of HDL, to act in clearing cholesterol from peripheral tissues to the liver for elimination and locally as anti-inflammatory and anti-oxidative mediator. Both genetic factors (Lipoprotein lipase deficiency, apoprotein deficiency, etc.), and lifestyle (sedentary behaviour and diets high in calories, saturated fat and cholesterol) contribute to the dyslipidemia seen in countries around the world.
Aggressive cholesterol reduction in patients with CHD or other atherosclerotic disease is now the standard of care, as agreed upon in a joint statement issued by the American Heart Association (AHA) [6]. Aggressive lipid lowering will reduce the number of acute coronary events and coronary intervention. A large number of angiographic trials have consistently demonstrated that cholesterol reduction resulted in slowing of progression of coronary disease compared with the control group. Several secondary prevention clinical trials have confirmed that cholesterol reduction in established CHD is highly effective in preventing future cardiovascular events and reducing total mortality [7].
In addition to life style modification, all patients of secondary prevention, and patients of primary prevention group with risk factors (Diabetes mellitus, Hypertension, Low HDL, Family history of CHD and LDL≥ 130 mg/dl) need lipid lowering drug therapy. Drug therapy of dyslipidemia is a safe and effective method of decreasing the risk of CHD and total mortality. Relative risk of CHD can be reduced by 25-30% by treating dyslipidemias with lipid lowering drugs [8]. Currently available hypolipidemic drugs like Statins (Ex: Atorvostatin), bile acid sequestrants (Ex: Cholestipol), nicotinic acid, fibrates all have their own adverse effects like myopathy and increase in hepatic transaminase with statins, flushing and dyspepsia with niacin, so we are still searching for more safer and efficacious drugs [1]. Silymarin a mixture of flavonolignans obtained from an edible plant ‘milk thistle’ (Silybummarinum) has been used as a herbal medicine for the treatment of liver related disorders for more than 2000 years. Silymarin consists of four flavonolignan isomers, namely silybin, isosilybin, silydianin and silychristin [9]. All these compounds are polyphenolic substances. Among them, silybin (50-60% of silymarin) is the most active substance and is largely responsible for the claimed benefit of silymarin. It causes inhibition of hepatotoxin binding to receptor site on the hepatocyte, reduction in glutathione oxidation, has antioxidant activity, stimulation of ribosomal RNA polymerase and subsequent protein synthesis, leading to enhanced hepatocyte regeneration [10]. Silymarin has metabolic and cell-regulating effects, namely carrier-mediated regulation of cell membrane permeability, inhibition of the 5-lipoxygenase pathway, scavenging of reactive oxygen species (ROS) of the R-OH type with an action on DNA-expression via suppression of nuclear factor (NF)-k B [9]. Silymarin a powerful antioxidant is said to protect liver cells and other cells in the body and brain. Various animal studies have reported that silybin’s antioxidant effect helps protect skin against photocarcinogenesis and renal tissue against cisplatin induced nephrotoxicity. Animal studies have shown silybin to have hypolipidemic property [11] and hence the present study was done to explore the hypolipidemic effect of silybin and its possible mechanisms of action in rats fed on hypercholesterolaemic diet.
Materials and Methods
The study was undertaken at Central Animal House, in a Tertiary Care Hospital, Tamil Nadu, India. All studies were conducted in accordance with the National Institute of Health “Guide for the care and use of Laboratory Animals” (NIH, 1985). The study was approved by the Animal Ethical Committee {Registration No 160/1999/ (CPCSEA)} Tamil Nadu, India (Proposal No.880, dated10.01.2012). Adult male Wistar rats (Rattus norvegicus) of 150-200g were used for this study. They were purchased from the Central Animal House, Rajah Muthiah Medical College and Hospital, Annamalai University, Annamalai Nagar, Tamil Nadu, India.
Animals were housed in polypropylene cages of dimensions 28cm x 22cm x 14cm, in groups of eight under controlled environmental conditions (Temp-23±20C, Humidity 65-70% and 12 hours light/dark cycles). The diet was standard pellet diet (VRK Nutritional Solutions, Baramati Agro Limited, Sangli, Maharashtra, India) and water ad libitum. Silybin (siliphos) was purchased from Swanson Health Products (Indena S.p.A., Italy) U.S.A. Each 300mg capsule of siliphos contained 89–109 mg of Silybin. The other ingredients were microcrystalline cellulose (plant fiber), gelatin, magnesium stearate and silica. Biochemical and enzymatic kits for measuring lipid peroxides and antioxidants enzymes were obtained from Sigma Aldrich chemicals. Cholesterol and sodium cholate in powder form were obtained from Hi Media chemicals.
Experimental induction of Hypercholesterolaemia
Hypercholesterolaemia in rats was induced by administration of high cholesterol. Diet (1%cholesterol, 0.5% sodium cholate, 1% coconut oil) for 60 days in standard rat chow diet. The rats were divided into four groups of eight each. The animals were housed in the animal house for 60 days.
Group-I (Normal control) - Treated with normal diet only.
Group-II (Experimental control) - High cholesterol diet (1% cholesterol, 0.5% sodium cholate, 1% coconut oil).
Group-III (High cholesterol diet+ Silybin 300mg/kg orally once daily).
Group-IV (High cholesterol diet+ Silybin 600mg/kg orally once daily).
Since, we do not know the exact mechanism of action by which silybin acts as hypolipidemic agent, we did not compare it with standard hypolipidemic drug instead we have compared it with the control group.
The animals in all the groups were fed with standard pellet diet and water ad libitum during the experimental period. Silybin was mixed with normal saline and administered through oral intragastric tube to groups III and IV. The dose of the silybin was arrived by a pilot study. At the end of 60 days the animals in all the groups were subjected to overnight fasting. Blood samples were drawn by retro-orbital puncture under intramuscular ketamine (CPCSEA guidelines-24mg/kg body weight) for biochemical analysis. The faecal matter was collected from all the groups during the last five days of the experimental study and processed for biochemical analysis.
Statistical Analysis
Values of Biochemical analyses were expressed as means ± S.D for eight rats in each group. The data were analysed by ANOVA followed by Duncan’s multi range test. Statistical analyses were performed using a software package SYSTAT 12. A value of p≤0.05 was used as the criterion for statistical significance.
Chemical method analysis
Total cholesterol was estimated by the method of Parekh and Jung [12]. Triglycerides were estimated by the method of Foster and Dunn [13]. The HDL cholesterol was estimated by the heparin-manganese chloride precipitation method [14]. VLDL was calculated using the formula.

Liver tissue from rats of all the groups were sliced into pieces and homogenised in appropriate buffer in cold condition (pH 7.0) to give 20% homogenate (w/v). The homogenates were centrifuged at 1000 rpm for 10 min at 0°C in cold centrifuge. The supernatant was separated and used for various biochemical estimations. The faecal bile acids were estimated according to the method of Grundy et al., [15].
Results
Serum Lipid Profile
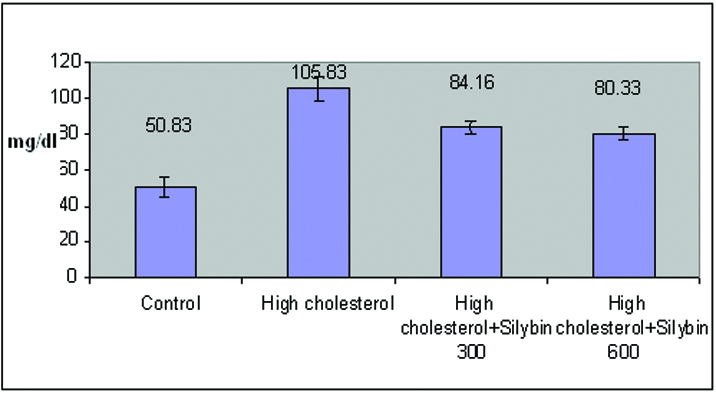
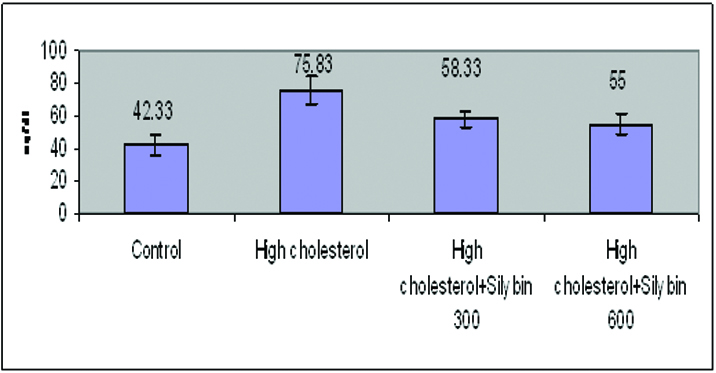
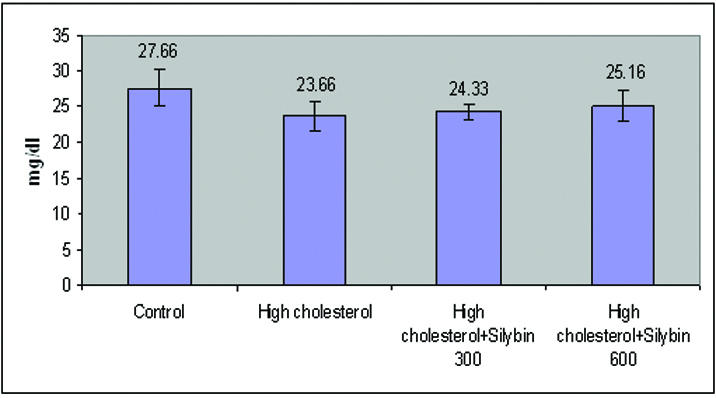
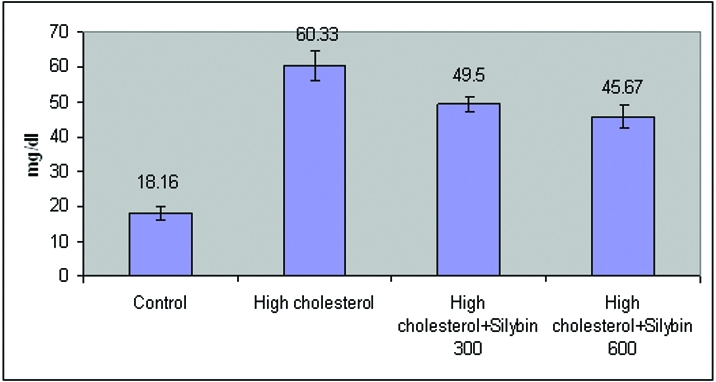
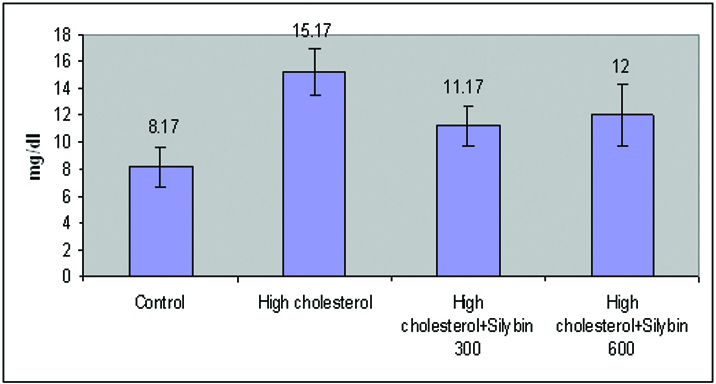
From [Table/Fig-1,2,3,4,5 and 6], it was observed that high cholesterol diet produced significant increase in (p<0.05) Total cholesterol, Triglycerides, VLDL-C, and LDL-C. High cholesterol diet also reduced HDL-Cholesterol significantly (p<0.05). Treatment with Silybin (300mg/kg) resulted in significant decrease of Total cholesterol (20%), Triglycerides (23%), VLDL-C (26%), and LDL-C (18%) and increase of HDL-C (3%). Silybin at 600mg/kg dose had resulted in further reduction in of Total cholesterol (24%), Triglycerides (27%), and LDL-C (24%). The effect of Silybin at 600mg/kg on the levels of VLDL-C and HDL-C was almost equal as that of Silybin at 300mg/kg.
Effect of Silybin on Plasma Lipid Profiles in Hypercholesterolaemic Rats.
| GROUPS | Total Cholesterol (mg/dl) | TGL (mg/dl) | HDL (mg/dl) | LDL (mg/dl) | VLDL (mg/dl) |
|---|
| Control | 50.83 ±5.41a | 42.33 ±6.12a | 27.66 ±2.58c | 18.16 ±1.94a | 8.17 ±1.47a |
| High Cholesterol | 105.83 ±6.82d | 75.83 ±8.70d | 23.66 ±2.06a | 60.33 ±4.41d | 15.17 ±1.72c |
| High cholesterol + Silybin300 mg/kg | 84.16 ±3.54c | 58.33 ±4.84c | 24.33 ±1.03b | 49.50 ±2.07c | 11.17 ±1.47b |
| High cholesterol + Silybin600 mg/kg | 80.33 ±3.72b | 55.00 ±6.78b | 25.16 ±2.13b | 45.67 ±3.266b | 12.00±2.28b |
Values are expressed as means ± S.D. for eight mice in each group. -Values not sharing a common superscript differ significantly at p=0.001 (Tukey’s range test).
Effect of Silybin on Plasma Total Cholesterol in Hypercholesterolaemic Rats.
Effect of Silybin on Plasma TGL in Hypercholesterolaemic Rats.
Effect of Silybin on Plasma HDL in Hypercholesterolaemic Rats.
Effect of Silybin on Plasma LDL in Hypercholesterolaemic Rats.
Effect of Silybin on Plasma VLDL in Hypercholesterolaemic Rats.
Hepatic Lipid Profile
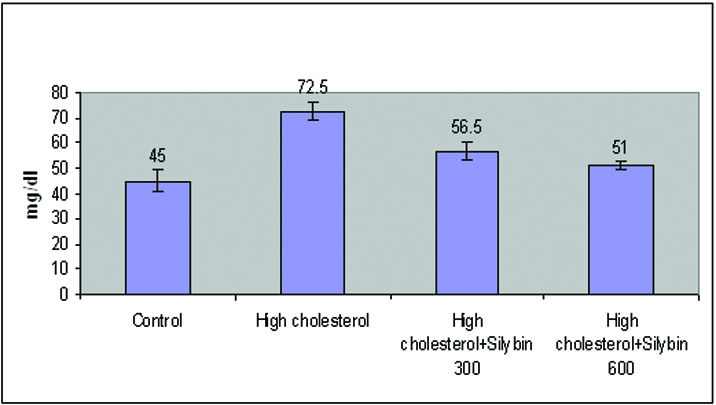
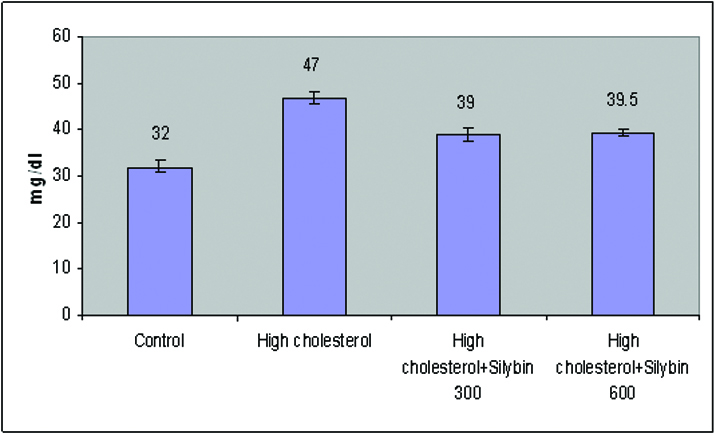
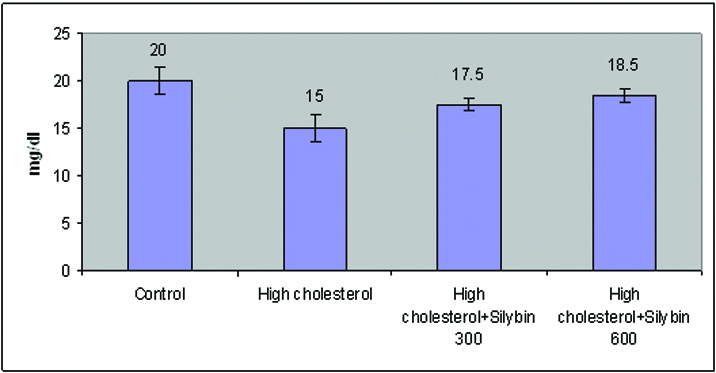
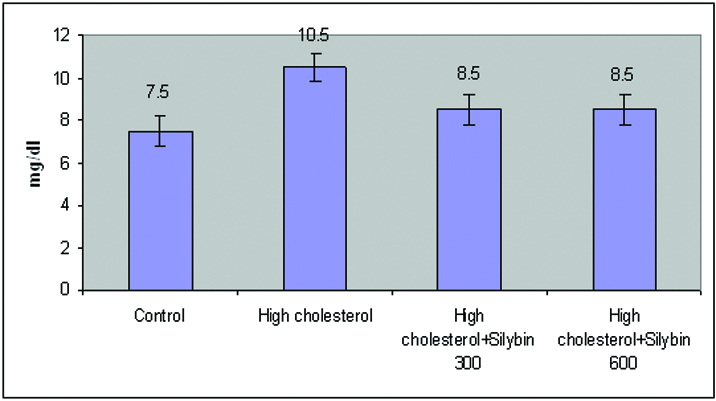
From [Table/Fig-7,8,9,10 and 11], it was observed that Hepatic Total cholesterol, Triglycerides, VLDL-C, and LDL-C were significantly increased (p<0.05) in high cholesterol diet fed rats. Hepatic HDL-C was also reduced significantly (p<0.05). Silybin at (300 & 600mg/kg) had significantly reduced hepatic Total cholesterol, Triglycerides, VLDL-C, and LDL-C (p<0.05). Silybin treatment had also increased the HDL-cholesterol significantly (p<0.05).
Effect of Silybin on Hepatic Lipid Profiles in Hypercholesterolaemic Rats.
| GROUPS | LIVERTotalCholesterol(mg/g) | LIVERTGL(mg/g) | LIVERHDL(mg/g) | LIVERLDL(mg/g) | LIVERVLDL(mg/g) |
|---|
| Control | 45.00 ±4.24a | 32.00 ±1.41a | 20.00 ±1.41c | 26.5±3.53a | 7.50±0.70a |
| High Cholesterol | 72.50±3.53d | 47.00 ±1.41c | 15.00 ±1.41a | 48.00±2.82c | 10.50 ±0.70c |
| High cholesterol +Silybin 300 mg/kg | 56.50 ±3.53c | 39.00 ±1.41b | 17.50 ±0.70b | 41.00±1.41b | 8.50 ±0.70b |
| High cholesterol +Silybin 600 mg/kg | 51.00±1.41b | 39.50 ±0.70b | 18.50 ±0.70b | 41.00 ±2.82b | 8.50±0.70b |
Values are expressed as means ± S.D. for eight mice in each group. -Values not sharing a common superscript differ significantly at p=0.001 (Tukey’s range test).
Effect of Silybin on Liver Total Cholesterol in Hypercholesterolaemic Rats.
Effect of Silybin on Liver TGL in Hypercholesterolaemic Rats.
Effect of Silybin on Liver HDL in Hypercholesterolaemic Rats.
Effect of Silybin on Liver VLDL in Hypercholesterolaemic Rats.
Faecal Bile Acids [Table/Fig-12]
Effect of Silybin on Faecal Bile Acids in Hypercholesterolaemic Rats.
| GROUPS | Cholic acid (mg/g faeces) | Deoxycholic acid (mg/g faeces) |
|---|
| Control | 0.22±0.01 | 0.17±0.01 |
| High Cholesterol | 0.5±0.02 | 0.5±0.01 |
| High cholesterol + Silybin 300 mg/kg | 0.89±0.02 | 0.84±0.02 |
| High cholesterol + Silybin 600 mg/kg | 0.92±0.03 | 0.89±0.02 |
High cholesterol diet fed rats showed increased excretion of bile acids through faeces. The levels of cholic acid and deoxycholic acid in faeces of silybin treated rats were much higher than the rats of high cholesterol fed.
Faecal Lipids
The levels of total cholesterol and triglycerides were increased in faeces of high cholesterol diet fed rats. Silybin treated group did not show change in total cholesterol and triglycerides in faeces compared to the cholesterol diet fed rats but significant increase as compared to control group of rats.
Discussion
Dyslipidemia including hypercholesterolaemia and low levels of HDL-C are the major causes of atherosclerosis and atherosclerosis induced conditions, such as coronary heart disease (CHD), ischaemic cerebrovascular disease and peripheral vascular disease. Atherosclerosis remains the major cause of death and premature disability in developed societies. In India, atherosclerotic CHD is expected to be the single most important cause of death by the year 2015. Genetic factors and unhealthy dietary practices contribute to the dyslipidemias seen in countries around the world. Number of human epidemiological studies and animal studies show that consumption of saturated fats, refined carbohydrates, as well as low consumption of vegetables and fruits tend to elevate the plasma cholesterol levels. Large epidemiological studies such as seven countries study [16] and the Framingham heart study [17] confirmed the strong relationship between the elevated serum cholesterol and subsequent atherosclerosis and atherosclerotic related CHD.
Since, hypercholesterolaemia constitutes one of the major risk factors for the development of CHD, a large number of animal experiments are being carried out to understand the better relationship between disorders in cholesterol metabolism and atherogenesis and to evaluate possible treatments. A great number of animal models, such as rabbits, mice, rats, chickens, swine, cats and dogs have been tested [18,19]. The most commonly used method to evaluate antihyperlipidemic drugs and antiatherosclerotic drugs is “Cholesterol diet induced hyperlipidemia in rats”. Rats fed on high cholesterol diet for thirty days show significant increase in serum and hepatic total cholesterol, LDL-C, VLDL-C, Triglyceride levels and decrease in HDL-C level [9,10].
In the present study also male wistar rats were used and hypercholesterolaemia was induced. At the end of 60 days it was observed that the rats fed on high cholesterol diet showed significant increase in serum total cholesterol, Triglycerides, LDL-C and VLDL-C. High cholesterol diet also reduced serum HDL-C. High cholesterol diet also significantly increased hepatic total cholesterol (61%), Triglycerides (46%), LDL-C (81%) and VLDL-C (40%). Rats treated with high cholesterol diet also showed reduced hepatic HDL-C (33%). Treatment with Silybin significantly decreased serum total cholesterol (24%), Triglycerides (21%), LDL-C (24%) in a dose dependent manner. Silybin treatment also reduced VLDL-C (26%) but the reduction was same at both the doses (300 and 600 mg/kg). HDL-C was also increased significantly (6%) in Silybin treated rats. Rats treated with Silybin (300 and 600 mg/kg) showed significant increase in hepatic HDL –C and decrease in other lipid profiles.
Silymarin a complex mixture of four flavonolignan isomers, namely silybin, isosilybin, silydianin and silychristin (with silybin being the most active) has been widely used from ancient times to treat human liver disorders [20]. The biochemical analyses of bile acids and lipids in faecal matter of hypercholesterolaemic rats showed an increased excretion. In silybin treated rats the fecal excretion of bile acids was increased but fecal lipid excretion was same as that of high cholesterol fed rats. Normally 95% of bile acids are reabsorbed. Enhanced excretion of faecal bile acids by Silybin depletes the pool of bile acids, and hepatic bile acid synthesis increases. As a result, hepatic cholesterol declines, stimulating the production of hepatic LDL receptors leading to enhanced clearance of plasma LDL, IDL and indirectly that of VLDL. This could be a possible mechanism of hypolipidemic effect of Silybin. This mechanism resembles that of the bile-acid sequestrants [21]. This result also showed that Silybin did not interfere with the absorption of cholesterol as there was no change in excretion of faecal lipids. Thus, biochemical analyses of plasma and hepatic lipid profiles, faecal bile acids and faecal lipids showed that Silybin had hypolipidemic activity and its hypolipidemic action could be due to enhanced endogenous cholesterol conversion to bile acids.
Conclusion
Unhealthy dietary practices and genetic factors contribute to the development of dyslipidemia which is the major cause of atherosclerosis and atherosclerosis induced conditions like coronary heart disease and ischaemic cerebrovascular disease. Atherogenesis is initiated by LDL-C oxidation. As a corollary to this hypothesis, antioxidant that inhibits lipid peroxidation should limit atherosclerosis and its clinical manifestations. Silybin, probably, by increasing the endogenous cholesterol conversion to bile acid ameliorated the hyperlipidemia in high cholesterol diet fed rats.
Its easy availability and low cost are added advantages. Hence Silybin, as anhypolipidemic can be utilized in conjunction with other antiatherogenic medicines.