Dengue is a mosquito-borne disease affecting humans mainly in tropical and subtropical regions of the world [1]. It is an increasing public health concern in urban and suburban areas causing morbidity and mortality [2–4]. Globally, WHO has estimated that around 3 billion people reside in areas where there are risks of exposure to dengue virus and nearly 50 million people are infected with dengue virus every year [5–7]. Dengue virus is a RNA virus, consisting of four serotypes (1, 2, 3 and 4) all of which cause infection. Infection with one serotype does not confer cross-protection against the other serotypes, instead can cause a severe form of infection [1]. Recently a fifth serotype was identified [8]. Early diagnosis plays a crucial role in detecting an epidemic or outbreak and in undertaking effective vector control measures [9].
There are several laboratory methods available to diagnose dengue infection such as viral isolation, detection of RNA, antigen and antibody assays. However, both viral isolation and identifying viral RNA through RT-PCR are time-consuming and need a specialized laboratory with costly methods and well-trained personnel which may not be widely available in hospital settings [7,9]. In most of the cases, serologic tests are used to detect IgM and IgG antibodies by ELISA. During the acute phase, the presence of IgM antibodies indicates primary infection and it appears after viremia ends or after fever subsides [10]. However, in secondary infections, IgG antibodies rise to high levels within the first week of infection and reduce over 3 to 6 months [2]. Recently, detection of nonstructural protein 1 (NS1) antigen during the acute phase of disease in patients having primary and secondary infections has been studied in various laboratories across the world [9,11–13]. NS1 is a highly conserved glycoprotein for all the serotypes and produced in both cell membrane-associated and secreted forms [7,11,13]. It is essential for virus viability or replication, but has no biological activity and precise function has not yet been assigned to it [11,14]. It stimulates a strong humoral response [15]. NS1 antigen is detectable in blood from first day after the onset of fever up to day 9, and is also detectable in the presence of IgM antibodies and when viral RNA is negative by RT-PCR [12].
The aim of this study was to evaluate NS1 antigen assay as an alternative to RT-PCR for the early diagnosis of Dengue.
Materials and Methods
The comparative study was conducted in the Department of Microbiology in collaboration with the Departments of Medicine and Paediatrics, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry from January to November 2011. The study was approved by the institute research and ethics committees. Serum samples were collected from two groups. Group 1 was the test group which included all patients (both adults and children) with fever fitting into WHO revised classification of dengue during the study period [6]. Group 2 was the control group which included 30 patients (both adults and children) with fever due to other causes (laboratory confirmed). Details of the patients with suspected dengue fever were recorded using a structured proforma. It included age, sex and address of the patient, whether from the rural or urban area, clinical details, platelet count, date of blood collection Post Onset of illness.
Blood samples (2-5ml) preferably paired, were collected from each of these cases, one as soon after admission as possible and the second sample one week later or at the time of discharge or whichever is later after obtaining written informed consent from the patient or guardian. Serum was separated and stored at -800C till the tests were performed. The detection of NS1 antigen was done using Panbio Dengue Early ELISA kit (Inverness Medical Innovations, Australia). The detection of IgM antibodies was done using Dengue-IgM capture ELISA kit (National Institute of Virology, Pune). IgG antibodies detection by ELISA was done using Dengue IgG ELISA (SCIMEDX Microwell ELISA Dengue IgG kit, USA). Manufacturer’s instructions were followed for all the kits used.
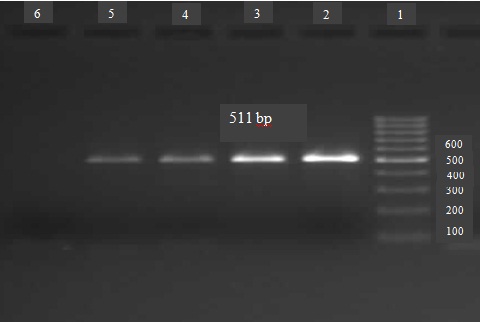
RT-PCR: The RNA from the samples was extracted using the commercial QIAmp Viral RNA Mini kit (QIAGEN, USA) according to the manufacturer’s instructions. The PCR was performed using 1μl of reverse transcriptase enzyme (Ambion, USA). The primer sequences used were as described by Lanciotti et al., [16]. The reaction mixture consisted of enzyme mix 1 μl, forward primer D1 0.1 μl, reverse primer D2 0.1 μl, RT-PCR buffer 12.5 μl and remaining RNAase free water for total reaction volume 25 μl with 5 μl of extracted RNA. For serotyping, the reaction mix was same except for reverse primer TS1, TS2, TS3 and TS4 0.1 μl were added for Den-1, Den-2, Den-3 and Den-4 respectively. Amplification products were separated by electrophoresis through 1.8% agarose gel (Agarose Low EEO, Bangalore genei, Bangalore, India) in 0.5 x Tris-borate-EDTA at 80 V for 45 min and were visualized by ethidium bromide staining under UV light for bands of DNA of expected size of 511 bp. The serotype-specific bands characteristic of each dengue virus, 482 bp for Den-1, 119 bp for Den-2, 290 bp for Den-3, and 389 bp for Den-4 were tested.
Sequence analysis: Two of the representative amplified products were sequenced to confirm the identity of the genes for dengue virus (Merck pharmaceuticals, Bangalore, India).
Statistical Analysis
Fisher’s exact test was performed using GraphPad Instat3 Software. p-value less than 0.05 was considered significant. Sensitivity, specificity, positive predictive value and negative predictive value of NS1 antigen assay against RT-PCR were calculated.
Results
Of the total 112 clinically suspected dengue cases, 94 were laboratory-confirmed dengue cases (positive by one or more of the following tests - IgM ELISA, NS1 antigen ELISA and RT-PCR). Though results of IgG were available for these 94 cases, the diagnosis could not be based on IgG detection alone as titres could not be determined with the test available. The control group consisted of 30 cases, which included patients with febrile illnesses confirmed by laboratory investigations as malaria (6 cases), enteric fever (6 cases), leptospirosis (6 cases), chikungunya (4 cases) and other flavivirus infections like hepatitis C (8 cases).
Most common age group affected was 0-12 years of age (35/94 – 37.2%), followed by young adults in the age group 13-24 years (26/94 - 27.7%). Females (57.5%) were affected more than the males with a male to female ratio of 1:1.35. The majority of patients were from urban areas (71/94, 75.5%). Of these, 51 cases were from the town of Puducherry. The majority of cases occurred during the month of November (46.8%) followed by October (34%). Most of the patients in case group had fever as the presenting feature (93/94, 98.9%). Other clinical presentations were vomiting (64%), headache (37%), rash (21%) and abdominal pain (12%). Bleeding and fluid accumulation which are the signs of warning and severe dengue were seen in 19.1% (18/94) and 20.2% (19/94) of cases. According to WHO revised classification, most of the cases came under dengue without warning signs criteria 51 (54.3%) and 10 (10.6%) had severe dengue. Thrombocytopenia (platelet count below 1 lakh) was seen in all cases of severe dengue, 90.9 % of dengue with warning signs and 78.4 % of dengue without warning signs.
Of the three assays used to confirm the diagnosis of dengue, NS1 had the highest positive detection rate of 80.9%, followed by RT-PCR with 68.1% and IgM ELISA with 47.9%. Both NS 1 and IgM ELISA were negative among the control group. IgG was found to be least specific as positivity was higher in controls (66.7%) than in cases (34%). Using a combination of the tests, NS1 and IgM had the highest positive detection rate of 97.8% followed by RT-PCR and IgM with 95.7% of positive detection rate [Table/Fig-1]. In patients where IgM was negative, 47/49 (95.9%) and 45/49 (91.8%) were positive by NS1 and RT-PCR respectively. Whereas, in patients where IgM was positive, 29/45 (64.4%) and 19/45 (42.2%) were positive by NS1 and RT-PCR respectively.
Positivity by NS1, IgM, IgG ELISA and RT-PCR in Laboratory confirmed Dengue cases.
| Tests | No. of casesn=94 (%) |
|---|
| NS1 | 76 (80.9%) |
| IgM | 45 (47.9%) |
| RT-PCR | 64 (68.1%) |
| NS1 and/or IgM | 92 (97.8%) |
| IgM and/or RT-PCR | 90 (95.7%) |
| NS1 and/or RT-PCR | 78 (82.9%) |
| IgG alone / in combination with other tests | 32 (34%) |
NS1 antigen positivity was seen as early as on day 1 of days post onset of illness (DPO), and it was detectable on day 12 in another case, with maximum positivity from day 2 to 5 post onset of illness (57/76, 75%). RT-PCR was also detectable on day 1 and positivity was seen on day 8 in another case, while maximum positivity was seen from day 2 to 5 post onset of illness (55/64, 85.9%) [Table/Fig-2]. For IgM, most of the positive cases were seen between 4th to 7th day post onset of illness (31/45, 68.9%). In early stages of dengue, considering the first 7 days post onset of illness, NS1 antigen detection had the highest positivity (76.6%) and in later stages (8 to 14 days) IgM antibody detection had highest positivity (14.9%) [Table/Fig-3].
Agarose gel electrophoresis of amplicons of common serotypes.
Lane 1: Molecular weight marker; Lane 2: Positive control; Lane 3,4,5: Positive test samples; Lane 6: Negative control.
Positivity of NS1, RT-PCR and IgM in Early (1 to 7 days) and Late (8 to 14 days) stages of Laboratory confirmed Dengue cases.
| Day post onset of illness (DPO) | NS1 | RT-PCR | IgM |
|---|
| 1 to 7 days | 72/94 (76.6%) | 63/94 (67%) | 31/94 (33%) |
| 8 to 14 days | 4/94 (4.3%) | 1/94 (1.1%) | 14/94 (14.9%) |
Based on Fisher’s exact test, the two–sided p-value was < 0.0001, considered extremely significant. Considering RT-PCR results as the reference standard, the diagnostic efficiency of NS1 antigen ELISA used in this study had 96.8% sensitivity, 53.3% specificity, 81.6% positive predictive value, 88.9% negative predictive value and 2.1 Likelihood ratio [Table/Fig-4].
Results of samples tested with NS1 antigen compared to RT-PCR.
| RT-PCR |
|---|
| Positive (n=64) | Negative (n=30) |
|---|
| NS1 antigen | Positive (n=76) | 62 | 14 |
| Negative (n=18) | 2 | 16 |
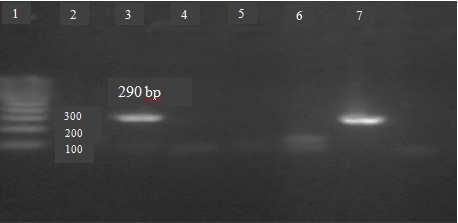
Serotyping: Of the RT-PCR positive cases, serotyping was done for 24 randomly selected samples which were distributed throughout the study period and not confined to the outbreak alone. All were found to be DEN-3 [Table/Fig-5].
Agarose gel electrophoresis of amplicons of DEN-3.
Lane 1: Molecular weight marker; Lane 2,5: Blank; Lane 3: Positive control; Lane 4: Negative control; Lane 6: Negative test samples; Lane 7: Positive test samples.
Discussion
Dengue virus infection most commonly affects tropical and subtropical regions of the world. Epidemics of dengue infection are showing an increasing trend in recent years. To date, there is no specific treatment for dengue virus infection. However, early diagnosis will help in the timely implementation of appropriate treatment, thereby greatly improving the outcome of the disease and also for effective public health control of dengue outbreaks [7]. There are various methods available for diagnosis of dengue virus infection. Virus detection by tissue culture and immunofluorescence gives definitive identification of the dengue virus serotype. Virus isolation, even though considered the “gold standard” for the diagnosis of dengue infections, requires early acute sample (0-5 days post onset), requires expertise and appropriate facilities, time-consuming, expensive and laborious [15].
NS1 antigen during the acute phase of the illness will be present in high titres in patient’s sera. [9,11]. It can be detected both in primary and secondary infections, but detection rate is higher in acute primary than in acute secondary infections [17–19]. NS1 is detectable in blood from the first day up to day 9 to 18 after the onset of symptoms [7,9,12,20,21]. In the present study, it was detectable on all 5 samples collected on day 1, and it was detectable on day 12 in another sample. NS1 antigen levels range from 0.004 to 2μg/ml in acute phase serum, to only 0.004μg/ml or less in convalescent-phase serum samples [22]. High levels of antigenaemia correlates with the development of DHF [13,14]. In the present study, a total of 22 DHF/DSS cases were NS1 positive, of which 18 were DHF and 5 were DSS cases. The optical density values of NS1 antigen ELISA among these cases were very high (average OD value-2.039), which could be taken as indirect evidence of high antigenaemia.
In the present study, using the combinations of 3 assays, a total of 94 cases were confirmed as dengue out of 112 clinically suspected cases. When taken alone, NS1 antigen detection had the highest positive detection rate of 80.9 % and IgM had least 47.9%. As these 2 markers appear at 2 different phases of the study, a combination of these tests could be expected to yield the highest positive detection rate. This was true in the present study, with 92 out of 94 cases being diagnosed as dengue using the combination of NS1 antigen and IgM ELISA.
There are several reports in the literature assessing the usefulness of different diagnostic tests in dengue. A study from Malaysia by Kassim et al., showed 69.2% of acute sera from suspected patients were positive for dengue based on IgM antibody ELISA (Panbio), IgG antibody ELISA (Panbio), NS1 antigen ELISA (Bio-rad) and PCR. Sensitivity of NS1, PCR, IgM and IgG were 32.2%, 38.5%, 40.9% and 36.1% respectively. In a combination of tests, PCR and dengue antibody and NS1 antigen and dengue antibody had the sensitivity of 65.9% and 62.0% respectively [7]. Another prospective study from Malaysia by Chua et al., tested 558 patients with clinical diagnosis of dengue and found 34.1% were laboratory-confirmed acute dengue. The sensitivities were 91.6%, 58.9%, 48.4% 40.5% for Platelia NS1 antigen-capture ELISA (Bio-Rad, USA), real-time RT-PCR, conventional RT-PCR and virus isolation respectively and authors have concluded that NS1 antigen-capture ELISA was the most sensitive, virus isolation was the least sensitive and real-time RT-PCR was significantly more sensitive than the conventional RT-PCR [1]. Pal et al., evaluated different NS1 antigen ELISA and rapid kits using virus isolation as the standard method. They have got 89.4% sensitivity with BioRad, 95.9% sensitivity with InBios, 85.5% sensitivity with Panbio NS1 antigen ELISA and overall sensitivity of rapid diagnostic tests (BioRad, InBios, Panbio and SD Bioline) varied from 71.9% to 79.1% [23]. Using a monoclonal antibody to a purified NS1 antigen, Lee J et al., recently developed and evaluated a rapid diagnostic test. They found this test to be more sensitive than other commercial ICT based NS1 antigen assays when tested against a panel of control sera [8].
Limitations
In the present study, NS1antigen ELISA was evaluated using RT-PCR as the reference standard. The specificity of NS1 was low as it was based on the assumption that the 12 cases detected by NS1 but not RT-PCR were false positive. The possibility that negative RT-PCR could have been due to the presence of PCR inhibitors should also be kept in mind, especially as no attempt was made to look for such inhibitors in this study and this is one of the limitations of the study. Other limitations were paired serum samples could not be collected from all the cases, it was not possible to classify dengue cases as primary and secondary as quantitative IgG assay was not performed and serotyping could not be done for all the samples, due to a limited fund available.
Conclusion
Dengue is the most common mosquito-borne viral infection in Pondicherry occurring in both endemic and outbreak forms with DEN-3 being the currently circulating serotype. Although there is no specific treatment available for dengue, early diagnosis has a role in individual case management as well as planning and implementing control strategies. Of the three different tests used to diagnose dengue, NS1 antigen detection had the highest sensitivity in the early stages while IgM detection was more sensitive in the later half of the illness. Both NS1 and RT-PCR are useful for early dengue diagnosis, although in terms of cost, ease of performance and rapidity, NS1 is superior to RT-PCR. Hence, NS1 in combination with IgM assay offers the most sensitive and cost-effective diagnostic modality for dengue.