Umbilical Sepsis Caused by Multidrug Resistant Strain of Kocuria kristinae in a New Born: A Case Report
Umadevi Sivaraman1, Pramodhini Subramanian2, Kalaivani Ramakrishnan3, K.S Seetha4
1 Professor, Department of Microbiology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth University, Pondicherry, India.
2 Associate Professor, Department of Microbiology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth University, Pondicherry, India.
3 Assistant Professor, Department of Microbiology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth University, Pondicherry, India.
4 Professor and Head of Department, Department of Microbiology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth University, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Umadevi Sivaraman, Professor, Department of Microbiology, Mahatma Gandhi Medical College and Research Institute, Sri Balaji Vidyapeeth University, Pondicherry, India.
E-mail: drumadevi@yahoo.co.in
Kocuria species were placed previously under the genus Micrococcus, are skin and oropharynx commensals in mammals, including man. A rare bacteria, Kocuria kristinae isolated from a new born with umbilical sepsis. Identification and antibiotic susceptibility was done by Vitek 2 compact system (Biomerieux). The isolate was sensitive to higher antibiotics like vancomycin, teicoplanin and linezolid. As this new pathogen resembles coagulase negative staphylococcus, it should not be misidentified.
Coagulase negative staphylococcus, Micrococcus, Vitek 2
Case Report
Here we report a case of umbilical sepsis caused by a rare bacteria, Kocuria kristinae. A new born baby of two-week-old was admitted in our hospital with umbilical sepsis. She was a term and quite healthy baby born by caesarean section due to non-progression of labour. Yellowish discolouration of the body most probably due to physiological jaundice, was noticed after two days of delivery and completely disappeared after phototherapy for sufficient period of time. All other parameters including vital signs were normal. There was no history of any congenital disorder or anomaly. A week later she was brought to hospital with complaints of fever and discharge from umbilicus. Pus sample was collected from the lesion and received in our laboratory for culture and sensitivity. Culture was done using Sheep Blood agar (SBA), Mac-conkey agar and Brain Heart Infusion broth, which showed smooth, small, moist, slightly convex, pale-pink colonies in SBA after overnight incubation [Table/Fig-1]. In gram staining it appeared as Gram positive cocci in cluster. It showed positive reaction for catalase, Coagulase negative, Furazolidone susceptibility and growth in 6% Nacl. Identification of the organism was confirmed as Kocuria kristinae by automation method using Vitek 2compact system (Biomerieux).
Kocuria kristinae colonies in SBA and Mac conkey agar.

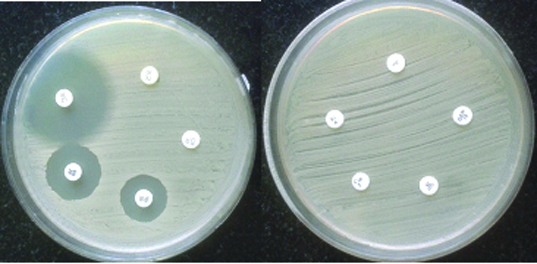
Antibiotic susceptibility testing was performed by routine disc diffusion as per CLSI guideline for Staphylococcus and also by Vitek 2 compact (Biomerieux) using GP AST card. Same type of sensitivity pattern was observed in both methods. Organism was sensitive to Vancomycin, Teicoplanin and Linezolid, but resistant to Penicillin, Oxacillin, Tetracycline, Cotrimoxazole, Erythromycin, Ciprofloxacin and Gentamicin [Table/Fig-2]. In addition to these drugs, sensitivity to Rifampicin, Daptomycin and Levofloxacin were also tested by vitek 2. It was found that organism was sensitive to Rifampicin and Daptomycin, but resistant to Levofloxacin. Patient was treated with parenteral vancomycin for a week and repeat sample did not yield any organism.
Sensitivity pattern of Kocuria kristinae showing sensitivity to Vancomycin, Teicoplanin & Lenezolid.
Discussion
Kocuria species belongs to Micrococcaceae family, were placed previously under the genus Micrococcus which are skin and oropharynx commensals in mammals, including man. They are also environmental organisms inhabiting the soil and several other ecological niches [1]. There are different species of Kocuria reported as pathogen from various clinical specimen considering as emerging newer pathogen. Documented cases of infections due to Kocuria spp are limited [2].
Among the Kocuria species isolated from various samples, K. kristinae, K. marina and K. rhizophila have been observed to cause infections in humans. As Kocuria kristinae (formerly Micrococcus kristinae) is one of the pathogenic species, which frequently colonizes the skin, human oropharynx and mucosa, so the source of infection could be from any one of the site. So far limited cases have been reported, majority from adult patients or older children. But there was a case reported from Delhi by Mapary Lakshmi kanth et al., that K.kristinae isolated from a newborn with bacteraemia and the baby was born by vaginal delivery which gives the explanation of contact with vaginal mucosa [3]. A review article by Vincenzo et al., mentioned that Kocuria appears to mostly affect immunocompromised hosts suffering from haematological malignancies, solid tumours or metabolic disorders [4]. Most of the cases reported already were associated with predisposing disorder, but in our case there was no immunosuppression or any congenital disorder observed except being a newborn. In general newborns have immature immune system, so that they are more vulnerable for any type of infection. A very healthy baby with unusual bacterial agent causing umbilical sepsis could be due to some close association with the organism in the maternal flora. This organism is normally present in the mucosa, but in our case the baby was born by Caesarean section not through normal birth canal. Possibilities of acquiring this unusual pathogen are either from hospital environment after delivery during the hospital stay or from maternal skin while taking care of the baby after discharge from hospital.
Regarding the sensitivity pattern, our strain was showing multidrug resistance which is uncommon for kocuria species. As per the report from Italy by Vincenzo et al., most strains of Kocuria were sensitive to doxycyclin, ceftriaxone, cefuroxime, amikacin, amoxicillin with clavulanic acid, ampicillin, vancomycin, Teicoplanin and erythromycin [4]. A study from Delhi reported resistance to penicillin, amikacin, ampicillin, vancomycin, ceftriaxone, clindamycin, cefazolin, erythromycin, levofloxacin minocycline and nitrofurantoin. Such resistant strain was isolated from a catheterised patient, but in same study strains isolated from a neonate and a five-year-old boy showed sensitivity to levofloxacin and minocycline [3]. Variable susceptibilities to β-lactams, quinolones, lincosamides and cotrimoxazole have been observed. Pathogenic Kocuria species are highly susceptible to broad-spectrum antibiotics [5]. In our case also isolate was sensitive to glycopeptide and Linezolid. Most of the reports showed the K.kristinae isolates were sensitive to vancomycin [6,7]. Resistance to many other group of antibiotics will be a major problem in managing the case.
Accurate identification of the organism is necessary as, such rare pathogens have been emerging, especially this organism is very much close to coagulase negative staphylococcus. Though previous study [8] explained about misidentification of coagulase negative staphylococcus as kocuria species by vitek 2 compact system, now with the help of new GP ID cards of Biomerieux it is possible to get accurate identification of kocuria species [9].
Conclusion
Now-a-days there are many newer bacterial agents emerging as pathogen in humans. One of the common organisms isolated in microbiology laboratory and considered as commensal is Micrococcus. But now it is very essential to differentiate coagulase negative staphylococcus from Micrococcus by performing few biochemical tests. Otherwise Coagulase negative Staphylococcus must be identified upto species level. Kocuria species especially K.kristinae have been reported from different regions as well as from different clinical specimens irrespective of their normal habitat which shows its expanding clinical spectrum. Most significant issue is the resistance pattern of these bacteria; in our case also it was found to be resistant to common drugs. So such emerging newer pathogens especially resistant strains become a challenge in the treatment are more dangerous (alarming).
[1]. Altuntas F, Yildiz O, Eser B, Gündogan K, Sumerkan B, Cetin M, Catheter- related bacteraemia due to Kocuria rosea in a patient undergoing peripheral blood stem cell transplantationBMC Infect Dis 2004 4:62 [Google Scholar]
[2]. Basaglia G, Carretto E, Barbarini D, Moras L, Scalone S, Marone P, Catheter related bacteraemia due to Kocuria kristinae in a patient with ovarian cancerJ Clin Microbiol 2002 40:311-13. [Google Scholar]
[3]. Mapary L, Verma D, Chander Y, Is Kocuria kristinae an upcoming pathogen?Int J Curr Microbiol App Sci 2015 4(4):885-89. [Google Scholar]
[4]. Vincenzo S, Chiara C, Gioviana M, Daniela A, Andrea B, Azaira B, Drug sensitivity and clinical impact of members of the genus Kocuria. ReviewJournal of Medical Microbiology 2010 59:1395-402. [Google Scholar]
[5]. Shashikala P, Rajagopalan S, Prashanth K, Narayanan K, Johny A, SheelaDevi C, Satish Kumar A, The expanding spectrum of human infections caused by Kocuria species: a case report and literature reviewEmerging Microbes and Infections 2013 2:1-8. [Google Scholar]
[6]. Marko F, Slobodan J, Dejana R, Velimir P, Nikola R, Predrag N, Synovitis and periarticular bursitis of the coxofemoral joint caused by Kocuria kristinae: A case reportScientific Journal of the Faculty of Medicine in Niš 2010 27(1):51-54. [Google Scholar]
[7]. Hsin-Mao C, Hsin C, Nan-Chang C, Fu-Yuan H, Kocuria kristinae: A true pathogen in pediatric patientsJournal of Microbiology, Immunology and Infection 2015 48:80-84. [Google Scholar]
[8]. Ben-Ami R, Navon-Venezia S, Schwartz D, Schlezinger Y, Mekuzas Y, Carmeli Y, Erroneous reporting of coagulase-negative staphylococci as Kocuria spp. By the Vitek 2 systemJ Clin Microbiol 2005 43:1448-50. [Google Scholar]
[9]. Wallet F, Loïez C, Renaux E, Lemaitre N, Courcol RJ, Performances of VITEK 2 Colorimetric cards for identification of gram-positive and gram-negative bacteriaJ Clin Microbiol 2005 43(9):4402-06. [Google Scholar]