Follicular Variant of Papillary Carcinoma Arising in Struma Ovarii
M. Ananta Satya Narayana1, K. Praveen Kumar2, B.A. Rama Krishna3
1 Assistant Professor, Department of Pathology, Alluri Sita Ramaraju Academy of Medical Sciences, Eluru, West Godavari, Andhra Pradesh, India.
2 Assistant Professor, Department of Pathology, Alluri Sita Ramaraju Academy of Medical Sciences, Eluru, West Godavari, Andhra Pradesh, India.
3 Professor and Head of Department, Department of Pathology, Alluri Sita Ramaraju Academy of Medical Sciences, Eluru, West Godavari, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M. Ananta Satya Narayana, Assistant Professor, Department of Pathology, Alluri Sita Ramaraju Academy of Medical Sciences, Eluru, West Godavari-534005, Andhra Pradesh, India.
E-mail: ananthsvimspath@gmail.com
Struma Ovarii, papillary carcinoma, follicular variant
Sir,
A 47-year-old female presented with pain in the right iliac fossa and excess menstrual bleeding since five months. Pain was non-radiating, gradual in onset and of moderate intensity. She was obese and anaemic. Abdominal examination revealed a single, soft to cystic, slightly mobile and non-tender mass in the right iliac fossa measuring 12x10cm. Examination of other systems were nil remarkable. Her haemoglobin was 11 gm/dl, TC, DC, Platelet count and urine examination was with in normal limits. Viral markers (VDRL, H.I.V and HBsAg) were nonreactive. Ultrasound abdomen revealed bulky anteverted uterus with fibroid in the anterior wall near the fundus and large right ovarian cyst. She was posted for total abdominal hysterectomy and right salpingoopherectomy. During surgery, there were no signs of capsular invasion or metastasis. Postoperative recovery is good.
Gross examination revealed a 4cm size fibroid in the body of the uterus and right ovarian cyst of size 15x15x12cm. Cut section of right ovarian cyst showed grey brown solid area measuring 7x7x5cm and a unilocular cystic area filled with light brown colour fluid. Histopathology revealed follicular variant of papillary thyroid carcinoma arising from pre-existing struma ovarii of right ovarian cyst and interstitial leiomyoma of uterus [Table/Fig-1a-c]
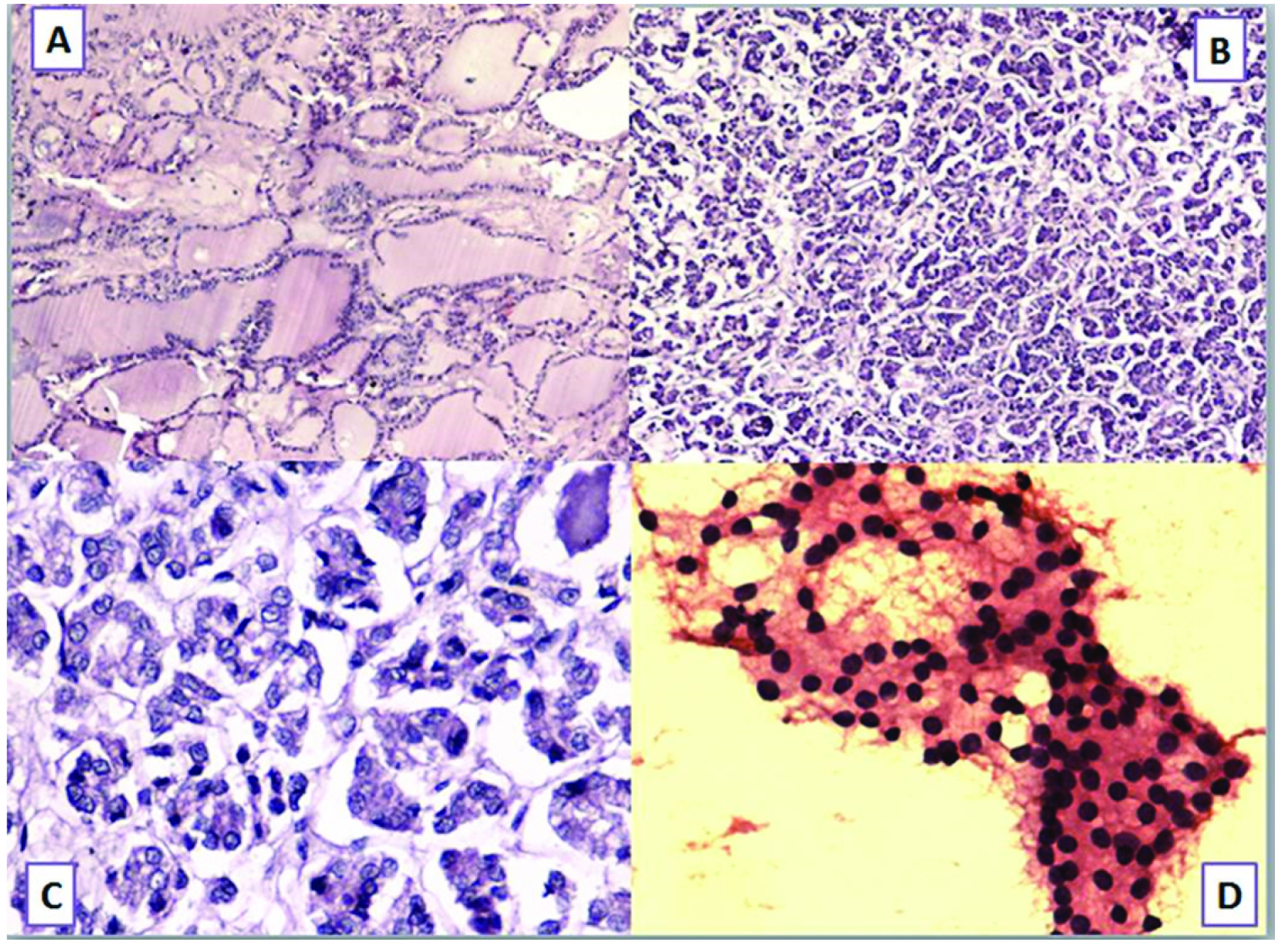
(a) Struma ovarii (H&E, X100)-Multiple variably sized colloid filled follicles lined by cuboidal follicular epithelium; (b-c) Thyroid type of papillary carcinoma (H&E, X100), (H&E, X400) - Microfollicles lined by cuboidal follicular epithelium displaying enlarged optically clear nuclei, prominent nucleoli, and longitudinal nuclear grooves. One of the follicle is filled with thick red colloid; (d) FNAC Thyroid (H&E, X100) - Honey comb sheet of thyroid follicles without any abnormality.
To rule out occult teratocarcinomas, alpha-fetoprotein (2.02ng/ml) and alpha-1-antitrypsin (1.56g/dl) levels were estimated postoperatively, they were with in normal limits. Thyroid profile was within normal limits. To rule out occult primary, ultrasound neck and FNAC of thyroid was done and it revealed adenomatous goitre [Table/Fig-1d] Serum thyroglobulin levels were estimated after 6 months of the surgery they were within normal limits (2.8ng/ml).
Struma ovarii is a monodermal variant of ovarian teratoma, which was composed of more than 50% of thyroid tissue. Malignant transformation of struma ovarii occurs rarely. Papillary and follicular thyroid carcinomas are the most frequent types of malignancy to occur in struma ovarii, whereas anaplastic and medullary carcinomas occur rarely [1].
A new variant of follicular carcinoma i.e. highly differentiated follicular carcinoma of ovarian origin (HDFCO) has been described by Roth and Karseladze which has an innocuous appearance, resembling that of nonneoplastic thyroid tissue in both the ovary and sites of dissemination [2]. Strumal carcinoid is a distinctive form of ovarian teratoma characterized by a mixture of thyroid tissue and carcinoid. Thyroid-type carcinoma can occur in strumal carcinoid [3].
Follicular variant of papillary thyroid carcinoma arising in struma ovarii exhibit diffuse positivity for CK19 and HBME-1(hector battifora mesothelial cell-1) which is similar to follicular variant of papillary carcinoma in cervical thyroid. Molecular analysis has revealed activating mutations of BRAF, NRAS, KRAS, RET/PTC and NTRK1 in approximately 70% of all follicular cell–derived thyroid carcinomas [1].
Surgical treatment includes total abdominal hysterectomy, plus bilateral salpingo-oophorectomy with omentectomy in postmenopausal women, or in premenopausal women who have completed childbearing [1]. Young women, with unilateral lesion without evidence of capsular invasion or gross metastasis, unilateral oophorectomy or strumectomy (cystectomy), should be performed for preservation of fertility [1]. Adjuvant therapy includes radioactive iodine ablation, external radiotherapy and chemotherapy. Radioactive iodine is the first-line therapy for treatment of recurrent disease [1].
Prognostic factors such as tumour size, extensive adhesions, capsular invasion, peritoneal dissemination, lymph nodal metastasis and solid histologic architecture were associated with an increased incidence of recurrence or metastasis. Anaplastic carcinoma is the most aggressive tumour type, followed by follicular, papillary and HDFCO is the least aggressive [4].
[1]. Zhang X, Axiotis C, Thyroid-Type Carcinoma of Struma OvariiArch Pathol Lab Med 2010 134:786-91. [Google Scholar]
[2]. Roth LM, Karseladze AI, Highly differentiated follicular carcinoma arising from struma ovarii: a report of 3 cases, a review of the literature, and a reassessment of so-called peritoneal strumosisInt J Gynecol Pathol 2008 27:213-22. [Google Scholar]
[3]. Pelosi G, Sonzogni A, Rosai J, Thyroid-type papillary microcarcinoma in ovarian strumal carcinoidInt J Surg Pathol 2008 16:435-37. [Google Scholar]
[4]. Robboy SJ, Krigman HR, Donohue J, Scully RE, Prognostic indices in malignant struma ovarii: clinicopathologic analysis of 36 patients with 20+ year follow-upMod Pathol 1995 8:95A [Google Scholar]