Congenital Absence of Internal Carotid Artery with Rare Type of Intercavernous Anastamosis and Ruptured Cerebral Aneurysm
Anand Alurkar1, Lakshmi Sudha Prasanna Karanam2, Sagar Oak3, Smita Kori4
1 Chief, Department of Neurointervention, King Edward Memorial Hospital, Pune, Maharashtra, India.
2 Consultant, Department of of Neurointervention, King Edward Memorial Hospital, Pune, Maharashtra, India.
3 Consultant, Department of of Neurointervention, King Edward Memorial Hospital, Pune, Maharashtra, India.
4 Consultant, Department of of Radiology, King Edward Memorial Hospital, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lakshmi Sudha Prasanna Karanam, Consultant, Department of Neurointervention, KEM Hospital, Rasthapeth, Pune-411011, India.
E-mail: drklsp@gmail.com
Congenital absence of Internal Carotid Artery (ICA) is a rare anomaly seen in <0.01% of the population. Various collateral circulations develop in these cases to maintain adequate cerebral perfusion. High incidence of aneurysms is reported in these cases. Complete evaluation is required to detect other abnormalities usually seen in these patients. We report a case of congenital absence of right ICA in a 39-year-old female who presented with Subarachnoid Haemorrhage (SAH) and had a Middle Cerebral Artery Aneurysm (MCA). The right MCA got supply from the intercavernous communication from the left internal carotid artery. Skull base Computed Tomogram (CT) confirmed the congenital absence of right ICA. She underwent successful surgical clipping for the aneurysm. The high incidence of aneurysms, collateral circulations, embryological development and postulated mechanisms of this anomaly were discussed. The exact aetiology behind the absence of ICA remains unclear. It is important to differentiate this condition from acquired stenosis/occlusion due to atherosclerosis and carotid dissection. Recognising the anomaly is important and gains even more significance during surgical planning in cases of direct aneurysm clipping, carotid endarterectomy and transphenoidal surgeries.
Carotid agenesis, Cerebral perfusion, Collaterals
Case Report
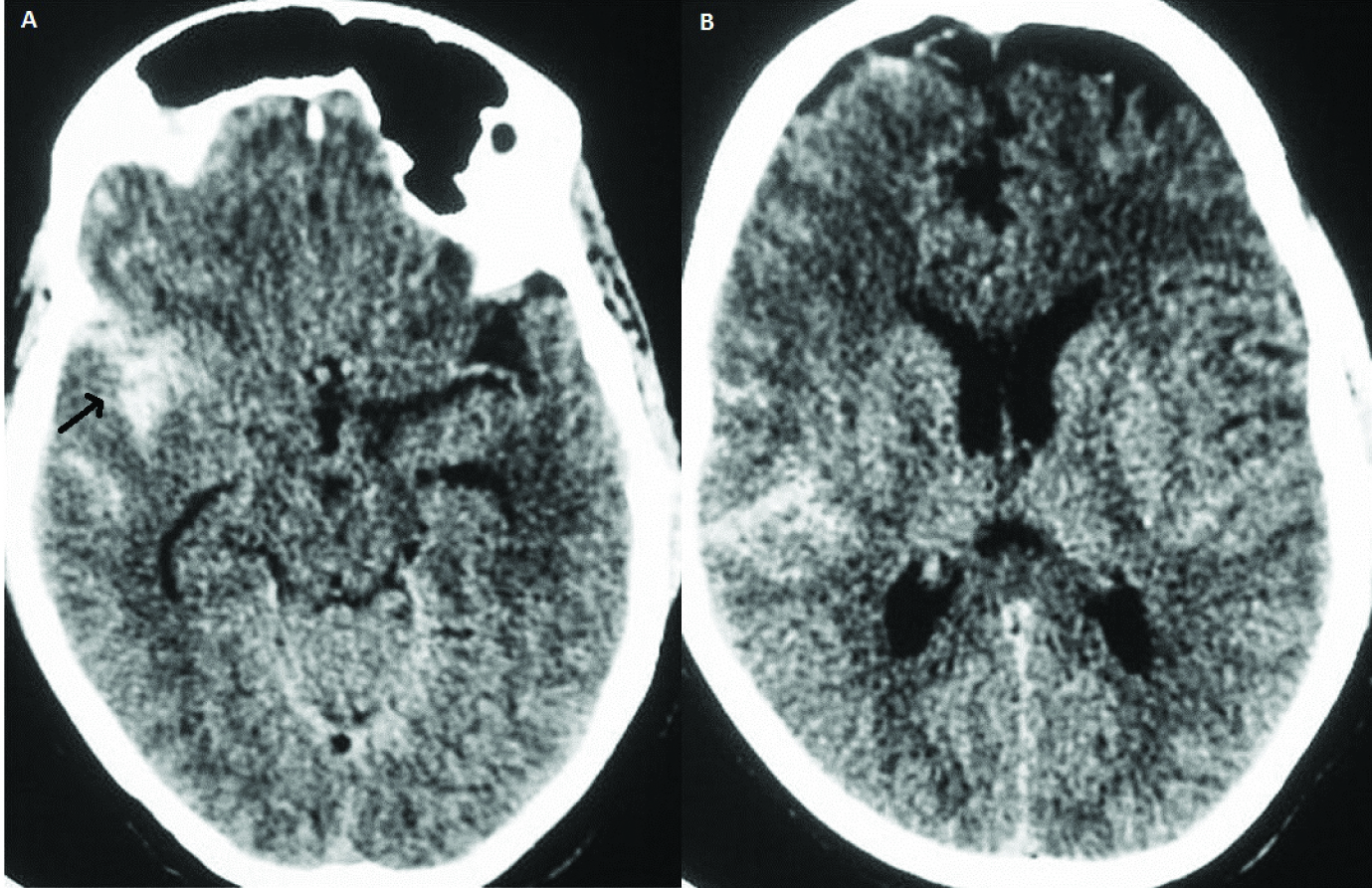
A 39-year-old female presented with sudden onset of severe headache to the Emergency department. On examination she did not have any focal neurological deficit. Computed topography scan done revealed SAH [Table/Fig-1] predominantly in the right sylvian fissure. She underwent subsequent Digital Subtraction Angiogram (DSA) which showed Right MCA bifurcation aneurysm filling on left ICA angiogram via the intercavernous communication.
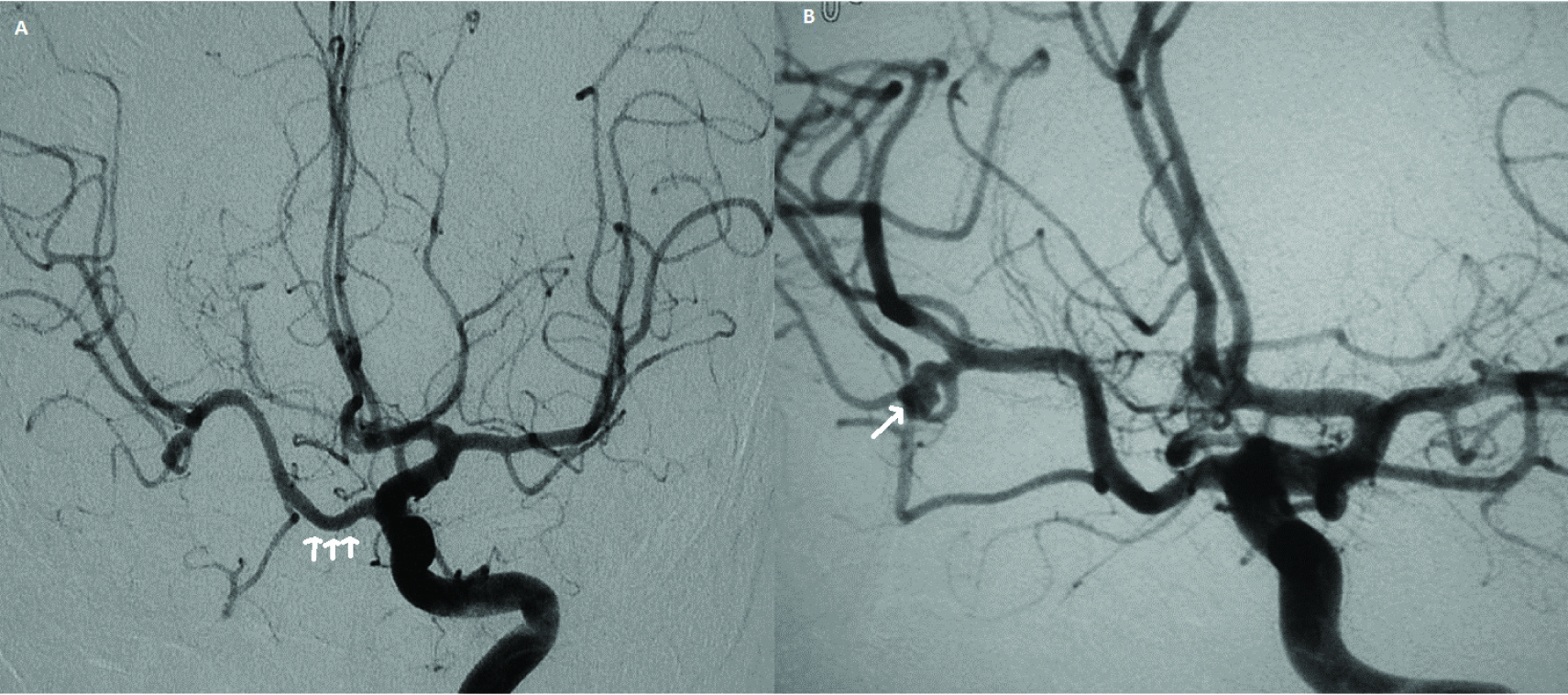
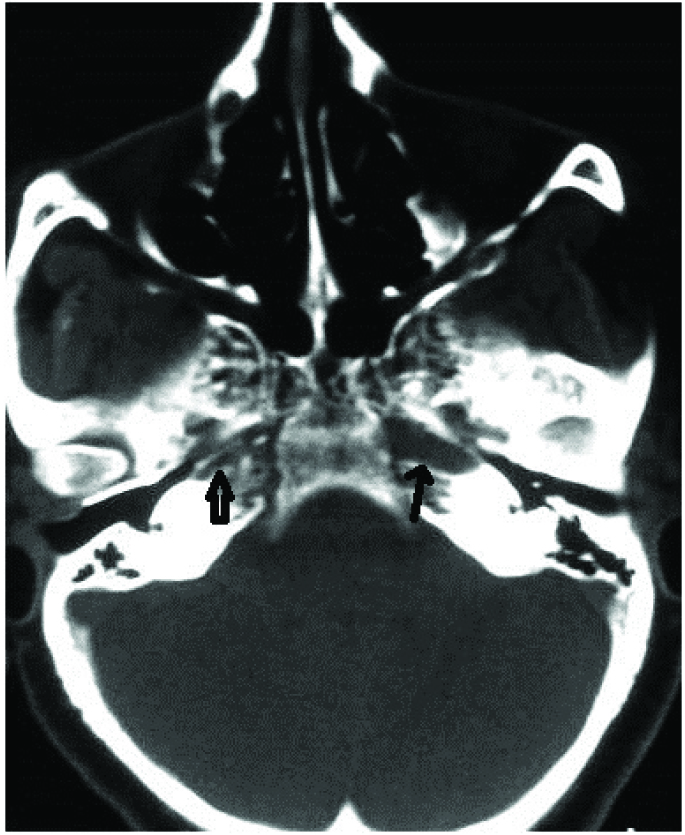
Aortogram [Table/Fig-2] showed direct origin of a small calibre right common carotid artery from the arch terminating in External carotid artery. Left ICA angiogram showed normal left intracranial ICA, MCA and Anterior Cerebral Artery (ACA). The right ACA is filling via Anterior Communicating artery (Acom). The right supraclinoid ICA, MCA is supplied via enlarged intercavernous communication from the left ICA. An inferiorly directed narrow necked aneurysm is seen in the right MCA bifurcation [Table/Fig-3]. High resolution CT scan of the base of the skull [Table/Fig-4] showed dimunitive right carotid canal and a normally developed left carotid canal. Patient underwent surgical clipping via the pterional approach with an uneventful postoperative course.
Plain CT scan images (A and B) showing subarachnoid haemorrhage predominantly in the right sylvian fissure as shown by the arrow.
Arch angiogram showing direct origin of right common carotid artery from the aorta which is uniformly small in calibre.

Anteroposterior view of the Left internal carotid angiogram (ICA) showed intercavernous collateral communication as shown by white arrows (3A). Right MCA bifurcation aneurysm is shown on the enlarged anteroposterior view of the left ICA (3B).
High Resolution CT scan of the base of skull shows the normally developed left carotid canal (single arrow) and a dimunitive one on the right side (double arrow)
Discussion
Verbiest first reported a case of ICA agenesis on angiogram in 1954 [1]. Congenital absence of ICA is usually unilateral and more common on the left side [2,3] and usually associated with other vascular abnormalities [4,5] . Congenital absence of ICA include agenesis, aplasia and hypoplasia and are often used as interchangeable [5]. The postulated aetiology of this anomaly include mechanical stress due to the pressure effects and excessive folding of cephalic portion of embryo [5] and amniotic bands. ICA development starts from first, third aortic arches and dorsal aorta at 4mm embryonic stage and completes by 6 weeks of foetal life [6].
Primitive pathways of collateral circulation [7] which include intercavernous anastamoses as in the present case usually form if disruption occurred before completion of circle of willis development (7-24mm stage of embryo). Skull base formation begins at 5-6 weeks of fetal life and hence congenital absence of ICA is always associated with carotid canal dimunition [6]. This documentation of skull base is important and confirms the diagnosis of congenital anomaly as opposed to acquired stenosis or occlusion [8]. Congenital anomalies of ICA are very rare occurring in <0.01% [6,9]. This anomaly is incidentally detected and these patients generally remain asymptomatic because of the good collateral circulation in spite of the absence of ICA.
Tsuruta and miyazaki classified three types of collateral circulations in these cases [9]. Lie first described six pathways of collateral circulation in association with absence of ICA [3,10] which are named as type A to type F as below.
Type A - Unilateral absence of the ICA with collateral circulation to the ipsilateral ACA through a Anterior Communicating Artery (ACOM) and to the ipsilateral MCA from the hypertrophic posterior communicating artery (PCOM), Type B - Unilateral absence of ICA with collateral flow to the ipsilateral ACA and MCA across a patent ACOM artery, Type C - Bilateral ICA agenesis with supply to the anterior circulation via carotid-vertebrobasilar anastomoses and through hypertrophic PCOM, Type D - Unilateral agenesis of the cervical portions of the ICA with collateral from an intercavernous communication from the cavernous segment of contralateral ICA, Type E - Bilateral hypoplastic ICAs supplying ACA and the MCAs are supplied by enlarged PCOMs, Type F - Flow to ICA across transcranial anastomoses from the branches of the ECA system, the so-called rete mirabile.
The collateral circulation in our case is type D variety of Lies classification. This intercavernous communication is proposed to develop because of the fusion between the two primitive trigeminal arteries that lost communication with the basilar artery [3,11].
In the presence of this type of collateral communication there will be associated hypoplasia or aplasia (as in our case) of ipsilateral A1 segment of Anterior Cerebral Artery (ACA) with patent Acom supplying the distal ACA territory. Thus, ipsilateral MCA is only supplied by intercavernous communication with no other alternate routes of collateral supply.
Incidence of intracranial aneurysms in these cases has been reported as 24-67% as compared to the 2-4% seen in general population [3,5,12]. Increased haemodynamic stress due to increased blood via collaterals and altered flow direction predisposes to aneurysm development [12,13]. Aneurysms ipsilateral to the aplastic ICA, as in the present report, are due to the congenital abnormality rather than altered haemodynamics [3].
Conclusion
Congenital absence of ICA is very rare and needs to be differentiated from the acquired stenosis and occlusion due to secondary causes. We reported one such rare case of congenital absence of ICA with intercavernous base of skull carotid anastamoses and MCA bifurcation aneurysm. Incidental detection of this anomaly should alert the clinician for close clinical follow up because of the high incidence of aneurysms in these patients. Further evaluation and work up is needed in these patients to rule out other vascular abnormalities and to detect the presence of collateral pathways. Thorough knowledge of collateral pathways is essential especially for surgical planning in these cases.
[1]. Verbiest H, Radiologic findings in a case with absence of the left internal carotid artery and compression of several cranial nerve roots in the posterior fossa by the basilar arteryMed Contemp 1954 71:601-09. [Google Scholar]
[2]. Florio F, Balzano S, Nardella M, Strizzi V, Cammisa M, Bozzini V, Congenital absence of the internal carotid arteryCardiovascular and Interventional Radiology 1999 22:74-78. [Google Scholar]
[3]. Given CA, Huang-Hellinger F, Baker MD, Chepuri NB, Morris PP, Congenital absence of the internal carotid artery: Case reports and review of the collateral circulationAJNR Am J Neuroradiol 2001 22:1953-59. [Google Scholar]
[4]. Ito S, Miyazaki H, Iino N, Shiokawa Y, Saito I, Unilateral agenesis and hypoplasia of the internal carotid artery: a report of three casesNeuroradiology 2005 47:311-15. [Google Scholar]
[5]. Lee JH, Oh CW, Lee SH, Han DH, Aplasia of the internal carotid arteryActa Neurochir (Wien) 2003 145:117-25. [Google Scholar]
[6]. Czarnecki EJ, Silbergleit R, Mehta BA, Sanders WP, Absence of the supraclinoid internal carotid artery in association with intracranial aneurysmsNeuroradiology 1998 40:11-14. [Google Scholar]
[7]. Cali RL, Berg R, Rama K, Bilateral internal carotid agenesis: a case study and review of the literatureSurgery 1993 113:227-33. [Google Scholar]
[8]. Worthington C, Olivier A, Melanson D, Internal carotid artery agenesis: Correlation by conventional and digital subtraction angiography, and by computed tomographySurg Neurol 1984 22:295-300. [Google Scholar]
[9]. Tsuruta J, Miyazaki Y, A case of complete absence of theinternal carotid artery associated with an aneurysm of the anterior communicating arteryNo Shinkei Geka 1977 5:895-900. [Google Scholar]
[10]. Lie TA, Congenital Anomalies of the Carotid Arteries 1968 AmsterdamExcerpta Medica:35-51. [Google Scholar]
[11]. Chen CJ, Chen ST, Hsieh FY, Wang LJ, Wong YC, Hypoplasia of the internal carotid artery with intercavernous anastomosisNeuroradiology 1998 40:252e4 [Google Scholar]
[12]. Amano T, Inamura T, Matsukado K, Ruptured saccular aneurysm of a dolichoectatic internal carotid artery in a patient with agenesis of the contralateral internal carotid artery: case reportNeuro Med Chir (Tokyo) 2004 44:20-23. [Google Scholar]
[13]. Ide M, Jimbo M, Yamamoto M, Posterior cerebral artery aneurysm associated with unilateral internal carotid artery agenesis Case reportNeurol Med Chir (Tokyo) 1995 35:825-29. [Google Scholar]