Numerous epidemiological studies have documented dental caries as the major public health problem throughout the world. It is gradually increasing in the underdeveloped and developing countries especially in children due to increasing popularity of refined sugars [1,2]. A causal association between the production of strong acids from plaque in response to sucrose and caries activity has become well established since 1940’s by Stephan [3]. However, it has been now demonstrated that dental caries does not necessarily occur if there is a balance in net mineral loss and mineral gain at the plaque-tooth interface. The inorganic composition of dental plaque matrix work under the influence of ions-calcium, phosphorous and fluoride as a see–saw mechanism. The inorganic components in plaque mainly calcium and phosphorous which are primarily derived from saliva play an important role in maintaining balance between de and remineralisation [4]. The rate of dissolution of enamel hydroxyapatite is determined chiefly by the level of saturation with these ions in the oral environment and the level of pH. At a given pH, if the plaque fluid adjacent to the tooth is supersaturated with calcium and phosphate ions, the enamel certainly cannot undergo demineralisation at its surface [5].
Numerous studies have shown that increasing calcium and phosphate concentration, which thereby increases pH in the tooth environment favours remineralization [6–8]. But most of these preventive measures are either expensive or not easily reachable to a common man and not a realistic option for the poor.
Throughout the history of mankind many infectious diseases are known to be treated with herbal remedies [9]. Many traditional Indian folk remedies, without scientific substantiation have been used to prevent dental caries [10–12]. The World Health Organization reported that 80% of the world’s population rely primarily on traditional medicine and a major part of the traditional therapies involve the use of plant extracts or their active constituents [13]. Plant products have received special attention because of being non-chemical, non-synthetic, safe and reliable. Hence, there is an urgent need to promote traditional preventive measures that are acceptable, easily available, and cost-effective. Studies have demonstrated antimicrobial properties of many plant products. Tulsi extract at 4% has shown a maximum antimicrobial property against Streptococcus mutans [14].
Many invitro studies have shown anti-inflammatory, antioxidant, anticarcinogenic, antimicrobial potential of various plant products [15]. Subramaniam et al., determined the effect of aqueous and organic extracts of three types of tea (green, oolong, and black tea) on the growth of S. mutans. Authors found that all the three types of tea inhibited the growth of S. mutans [16]. Plant products as remineralizing agent yet needs substantial evidence.
As CPP-ACP is now the known agent for remineralization it was used for comparison with other plant products in this study.
The aim of the study was to evaluate the effect of natural chewable products (Tulsi, sesame seeds, fennel seeds, coconut) and ACP-CPP chewing gum on plaque pH, calcium and phosphate concentration.
Materials and Methods
A randomized controlled trial, with a cross-over study design, was conducted to assess the effect of four natural plant products (Fennel seeds (1gm), Sesame seeds (1gm), Coconut (1gm), Tulsi (5 fresh leaves) and CPP-ACP chewing gum (1pellet) on human dental plaque [Table/Fig-1].
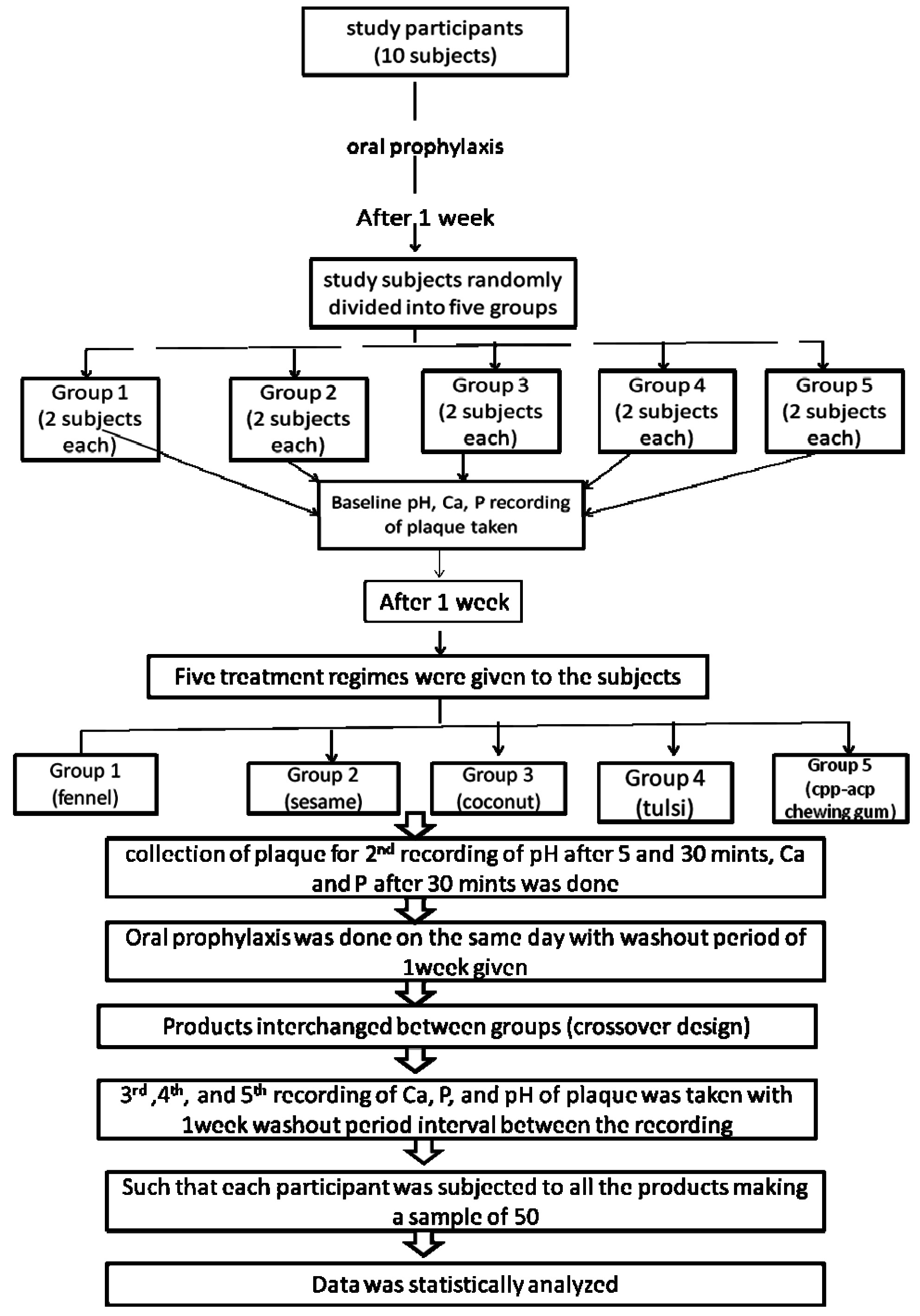
Prior to the conduct of study ethical approval was taken from the Institutional Ethical and Review Board withreference no.-KDCRC/IERB/10/2014/09. The study was carried on a total of ten subjects, age 15-17-year-old, who fulfilled the eligibility criteria. Those subjects who were healthy, caries-free and willing to participate, were included into the study while those who were on medications (antibiotics, anti-acids) having effect on plaque formation and who were undergoing orthodontic/periodontal procedures; were excluded from the study. The study protocol was explained to the subjects well in detail. They were informed that the study would long for a period of one & half month during which there should be no deviations from the routine dietary habits by the subjects. After taking their informed consent, oral prophylaxis was carried out for all the study participants one week before the baseline data recording; who were then instructed to refrain from oral hygiene practice for 48 hours prior to the sample (dental plaque) collection. Then the study sample was randomly divided into 5 groups (Fennel seeds, sesame seeds, coconut, Tulsi and CPP-ACP); 2 subject each. The baseline plaque pH was measured for all subjects at 4 sites (mesial surface of 16, distal surface of 26, mesial surface of 36 and distal surface of 46); using Beetrode pH Touch Electrode (World Precision Instruments, Inc.) connected to a display unit. To protect the cross contamination, the electrode was rinsed in distilled de-ionized water between each reading. Then equal amounts of pooled plaque samples were collected by removing all visible plaque from 1st and 3rd quadrants of the mouth using sterile blunt ended spatula avoiding obvious food debris. The plaque collection was standardized by taking equal volumes and plaque ionic calcium concentration was analysed using an electrode analyser (Spectrolab K) and inorganic phosphorus by the method of Chen & Toribara [17].
After the baseline estimation of plaque pH Ca and P; the subjects of the respective groups were asked to chew the equal quantity of products for 5 minutes and they were asked to swish their mouths with de-ionized water. Then pH was recorded at 5 and 30 minutes and Calcium and Phosphorus concentration was estimated after 30 minutes for second recording by a similar method.
Study participants were subjected to oral prophylaxis once again and then given a wash out period of one week after which similar procedure was repeated using cross-over design i.e.; by interchanging the product group allocation for 3rd, 4th and 5th recording, respectively. It was ensured that each study participant was subjected to all the products making a effective sample of 50. The data was statistically analysed. Difference in mean plaque pH values between the groups and at different time intervals were statistically analysed using One-way ANOVA and compared using post hoc test.
Results
Data on the mean of pH at baseline, after 5 minutes and 30 minutes and mean of calcium and phosphate at baseline and after 30 minutes among all the five study groups are showed in [Table/Fig-2,3 and 4].
Mean plaque pH values before and after chewing coconut, tulsi, sesame, fennel and recaldent at baseline, 5 minutes and 30 minutes.
| BaselinepH(mean) | 5 minpH(mean) | 5 minpH(p value) | 30 minpH(mean) | 30 minpH(p value) |
|---|
| Coconut | 6.65 | 6.81 | .008* | 6.80 | .071 |
| Tulsi | 6.62 | 6.87 | .001* | 6.92 | .001* |
| Sesame | 6.66 | 6.83 | .001* | 6.93 | .001* |
| Fennel | 6.66 | 6.69 | .677 | 6.80 | .029* |
| recaldent | 6.66 | 6.89 | 0.01* | 7.04 | 0.01* |
*statistically significant when compared with baseline pH using t-test
Mean calcium concentration values before and after chewing coconut, tulsi, sesame, fennel and recaldent at baseline and 30 minute interval using paired-t Test.
| coconut | tulsi | sesame | fennel | Recaldent |
|---|
| Baseline Ca | 2.37 | 2.25 | 2.29 | 2.18 | 2.36 |
| Post Ca | 2.72 | 2.50 | 2.73 | 2.75 | 2.83 |
| diff | 0.35 | 0.25 | 0.44 | 0.57 | 0.47 |
| p-value | .004* | .006* | .000* | .008* | .001* |
*Statistically significant when compared with baseline pH using t-Test
Mean phosphate concentration values before and after chewing coconut, tulsi, sesame, fennel and recaldent at baseline and 30 minute interval using paired-t Test.
| coconut | tulsi | sesame | fennel | Recaldent |
|---|
| Baseline phosphate | 2.42 | 2.22 | 2.31 | 2.17 | 2.37 |
| Post phosphate | 2.59 | 2.45 | 2.54 | 2.36 | 2.90 |
| diff | 0.17 | 0.23 | .23 | 0.18 | .53 |
| p-value | 0.049* | 0.025* | 0.016* | 0.042* | .001* |
*statistically significant
The mean pH in all the study groups increased after 5 minutes and 30 minutes compared to baseline and it was statistically significant, except for coconut group at 30 minutes and fennel group at 5 minutes. Recaldent group showed a highest increase in plaque pH after 5 minutes and 30 minutes.
A statistically significant rise in post calcium and post phosphate was found among all 5 groups. The highest increase in plaque calcium concentration was found in fennel group followed by recaldent and sesame, respectively. Whereas, the highest increase in plaque phosphate was found in recaldent group followed by sesame group and fennel group respectively. [Table/Fig-5] represents statistical analysis using Anova, used to compare between the five study groups. [Table/Fig-6] represents Post-hoc analysis showing significant pairs as obtained from [Table/Fig-7,8].
Comparison of mean of pH, calcium and phosphate at different time intervals in five groups using ANOVA.
| | Mean Square | F | p-value | |
|---|
| Pre-pH | Between Groups | .003 | .112 | .978 | |
| Within Groups | .026 | | | |
| pH after 5 mints | Between Groups | .062 | 3.564 | .013 | significant |
| Within Groups | .017 | | |
| pH after 30 mints | Between Groups | .103 | 4.695 | .003 | significant |
| Within Groups | .022 | | |
| Pre- calcium | Between Groups | .063 | 1.339 | .270 | |
| Within Groups | .047 | | | |
| Post - calcium | Between Groups | .382 | 4.020 | .007 | significant |
| Within Groups | .095 | | |
| Pre - phosphates | Between Groups | .100 | 1.449 | .233 | |
| Within Groups | .069 | | | |
| Post- phosphates | Between Groups | .420 | 4.678 | .003 | significant |
| Within Groups | .090 | | |
Post-hoc test for significant pairs for ph, calcium and phosphate
| Ph after 5 min | pH after 30 min | Post calcium | Post phosphate |
|---|
| Coconut vs fennel | Fennel vs tulsi | Fennel vs recaldent | Fennel vs recaldent |
| Fennel vs sesame | Fennel vs recaldent | Tulsi vs recaldent | Tulsi vs recaldent |
| Fennel vs tulsi | | | Sesame vs recaldent |
| Fennel vs recaldent | | | |
pH values using post-hoc test
| Pre pH(mean) | 5 min pH(mean) | 30 min pH(mean) | p-value5 min | p-value30 mint |
|---|
| Coconut | 6.65 | 6.81 | 6.80 | .008 | .071 |
| Tulsi | 6.62 | 6.87 | 6.92 | .001 | .001 |
| Sesame | 6.66 | 6.68 | 6.93 | .001 | .001 |
| Fennel | 6.66 | 6.69 | 6.80 | .677 | .029 |
| recaldent | 6.66 | 6.89 | 7.04 | 0.01 | 0.01 |
Calcium & phosphate values using post-hoc test.
| Pre cal(mean) | Post cal(mean) | Pre phosp | Postphosp | p-valuecal | p-valuephosp |
|---|
| Coconut | 2.37 | 2.72 | 2.42 | 2.59 | .004 | .049 |
| Tulsi | 2.25 | 2.50 | 2.22 | 2.45 | .006 | .025 |
| Sesame | 2.29 | 2.73 | 2.31 | 2.54 | .001 | .016 |
| Fennel | 2.18 | 2.75 | 2.18 | 2.36 | .038 | .042 |
| recaldent | 2.36 | 2.83 | 2.37 | 2.90 | .000 | .001 |
Discussion
Plant products have stood the test of time for their safety, efficacy, cultural acceptability and lesser side effects in contrast to the synthetics that may be harmful to human and environment [18,19]. In addition to their health benefits very few studies have documented their rational of use in dentistry. In this study four commonly available plant products as fennel seeds, tulsi leaves, sesame seeds and coconut were compared with CPP-ACP containing chewing gum for their effect on dental plaque.
Fennel seeds, scientifically known as foeniculum vulgare are a shout, tall, aromatic herb. It is grown extensively all over Europe, Middle East, China and Turkey. They are concentrated source of minerals and vitamins. Its mineral and vitamin contents are calcium, phosphorous, iron, sodium, potassium, thiamine, riboflavin, niacin and vitamin C [20].
Koudela and Petrikova suggested the monitored parameters of potassium, sodium, manganese and calcium in fennel as 504.6, 29.45, 23.55 and 20.95 mg/100 g and trace amount of iron and zinc, correspondingly [21]. The results of the present study revealed that fennel chewing led to an increase in plaque pH, calcium and phosphate concentration. This shows that the diffusion of calcium and phosphate into plaque has occurred which may be due to the leaching of calcium from fennel seeds due to chewing which increases salivary flow and hence increases pH and calcium and phosphate concentration of plaque.
Shirahatti RV et al., evaluated the effect of fennel seeds on plaque and salivary pH and found that these seeds increased pH at 5 minutes, although it was not significant [22]. Ajithkrishnan CG et al., found a statistically significant rise in salivary pH immediately after chewing fennel seeds [23].
Tulsi, queen of herbs, scientifically known as Ocimum sanctum is a medicinal herb used in Ayurvedic medicine since ancient times. Some of the main chemical constituents of Tulsi are: Oleanolic acid, ursolic acid, rosmarinic acid, eugenol, carvacrol, linalool, β-caryophyllene (about 8%), β-elemene (11.0%), and germacrene D (about 2%) [24]. Our results revealed a significant increase in plaque pH after 5 minutes and 30 minutes and a significant increase in calcium and phosphate concentration after chewing tulsi leaves. Studies have shown Tulsi to inhibit the plaque biofilm formation by reducing the adhesion of microbial pathogens to the tooth surface, which is a primary event in the initiation of dental caries [25,26]. This property of inhibition of biofilm formation is due to the antimicrobial compounds in it such as antibiotics, cell wall degrading enzymes [27]. These results in inhibition of many pathogenic organisms which inturn increases pH and hence can decrease the caries activity. It has maximum antimicrobial potential at the 4% concentration level [28]. Due to non-availability of such similar studies in the literature the exact mechanism of action of these plant products on plaque pH and calcium and phosphate concentration is inconclusive.
Sesame seeds, scientifically known as Sesamum indicum is considered to be the oldest oilseed crop known to humanity. It has been utilized for over 5,000 years and may be one of the most potent, nutrient-dense medicinal foods still used today. The seeds are especially high in calcium, phosphate, potassium, manganese, sodium, iron and low amounts of zinc [29].
After chewing sesame seeds subjects showed a significant increase in plaque ph after 5 and 30 mints which could be because of chewing effect which increases salivary flow and hence increases plaque pH. Asokan S et al., in their study found a significant reduction in the S. mutans count in plaque and saliva of children after oil pulling with 1 teaspoon (5ml) of sesame oil [30]. Rise in calcium and phosphate concentration could be due to presence of these ions in sesame seeds. Due to the scarcity of similar studies exact mechanism describing the increase in the concentration of calcium and phosphate concentration and pH after chewing sesame is yet to be proven.
Coconut, scientifically called as Cocos nucifera, belongs to the large palmaceace family of palm trees. It has excellent source of minerals [31]. Coconut oil extracted from dry nut is an excellent emollient agent. It contains lauric acid which is a bacteria whooping ingredient. It inhibits S mutans to adhere on the tooth surface and hence inhibits dental caries [32]. Thaweboon et al., in their study have found that 5ml of coconut oil exhibited antimicrobial activity against S. mutans and C. albicans whereas 5ml of sesame oil had activity against S. mutans [33].
Results after chewing coconut showed a significant rise in calcium and phosphate concentration but plaque pH raised only after 5 minutes which slowed down after 30 minutes, although the drop in pH was not much. The increase in calcium and phosphate concentration could be due to the increase of these ions in saliva due to chewing which increases salivary flow and hence increases pH and calcium and phosphate concentration of plaque.
Chewing gum in various forms is as popular as ever. Numerous studies have demonstrated anticariogenic potential of Casein phosphopeptide amorphous calcium phosphate (CPP–ACP) nanocomplexes [34–36]. The anticariogenic property of CPP-ACP has been attributed to the ability of CPP to localize amorphous calcium phosphate at the tooth surface, maintaining a state of supersaturation with respect to enamel mineral, thereby depressing enamel demineralisation and enhancing remineralization [37]. Our results showed a highest rise in the mean plaque pH after 5 minutes and 30 minutes which were statistically significant. Rise in the phosphate concentration in this group was highest. However, calcium concentration was highest in fennel group than CPP-ACP. RECALDENT™ (CPP-ACP) is a revolutionary ingredient that stabilises and delivers high quantities of calcium and phosphate, which are the essential building blocks for teeth [38]. Santhosh BP et al., observed a significantly increase in the salivary calcium and phosphate concentration after chewing CPP-ACP containing chewing gum [8]. But there are reports in the literature where children have swallowed chewing gums causing gastrointestinal problems in them [39]. Hence, cannot be recommended below 4 years. Also people with milk protein allergy need to avoid such products [40,41]. In addition, CPP-ACP containing chewing gums are costly and not easily reachable to rural areas. On the contrary, the plant products used in this study are excluded from such side effects. As in if swallowed they possess more beneficial than harmful effects.
The increase of calcium in fennel group than CPP-ACP chewing gum could be due to some intrinsic factors like texture, nature and difference in the composition and intrinsic variations among subjects. A thorough knowledge of this difference is to be studied at a molecular level.
Sesame and fennel seeds are often used in India as mouth fresheners and aids in digestion after meals. They have unlimited health benefits. Authors have described the use of fennel seeds because of their nutritional value, easy availability and common use [42]. Apart from the general health benefits from chewing these seeds, our study has shown their benefits towards dental health also. Benefits in terms of their composition, longer storage of fennel seeds, fennel seeds can be consumed in combination with sesame seeds and are easily accessible to the poorest.
Limitation
Due to the lack of similar clinical trials in the literature, enough supporting articles could not be used in our discussion.
Conclusion
A need to explore and promote the use of such locally available and accessible methods gave us the opportunity to evaluate the dental plaque pH and calcium and phosphate concentration. Caries progression control, especially in its initial clinical stages, may be favoured by chewing such plant products. These can be considered as the measures for remineralization beyond fluoride. Taking more advantage of the composition and the nutritional value of such natural plant products in improving oral health, we can serve our patients better. Further studies on the effect of these plant products on oral cavity and caries prevention are recommended.
*statistically significant when compared with baseline pH using t-test
*Statistically significant when compared with baseline pH using t-Test
*statistically significant