Dental caries is the most prevalent chronic disease affecting humans irrespective of age, sex, race and socioeconomic status [1]. As around 90% of school children and most of the adults have been affected by dental caries, hence it has been considered as the most important global oral health burden [2]. Epidemiological surveys are important for monitoring trends in dental caries and for assessing the dental needs [3]. According to the World Health Organization (WHO 1997), detection of dental caries in surveys has been performed at cavitation level because examiners frequently cannot reliably assess the non-cavitated lesions. However, the inclusion of non-cavitated caries lesions is necessary since these can be arrested through certain preventive measures and lowering the cost of restorative treatment [4]. Hence, especially in a population with low prevalence of dental caries, the introduction of a criterion which include non-cavitated caries with the purpose of improving the sensitivity of caries epidemiology and clinical trial are required [5].
The International Caries Detection and Assessment System (ICDAS), based on visual inspection, was developed for use in clinical research, clinical practice and for the epidemiological purpose [4]. The system was intended to be feasible for use in epidemiological surveys and to detect cavitated and non-cavitated lesions with acceptable reliability [6].
The aim of this study was to assess the prevalence of dental caries in school children using ICDAS II (International Caries Detection and Assessment System) criteria in Pallikkaranai (corporation zone 14) Chennai, India.
Materials and Methods
This study was carried out in the Department of Pedodontics and Preventive Dentistry from the period of February 2012 to January 2014, at Sree Balaji Dental College and Hospital, Chennai, Tamil Nadu, India.
There were total 15 zones in Chennai of which zone 14 was selected by random sampling method [Table/Fig-1]. The list of recognized schools in the corporation zone 14, Chennai corporation was obtained from the Pallikkaranai corporation office by the researcher. The researcher then visited each school individually and explained about the study and obtained consent along with the baseline data on a number of 6-14 year age group children enrolled from the school authorities. A self-administrated questionnaire (Based on WHO basic oral health survey form) and a consent form to participate in the study were given to the students, to be duly filled by the parents prior to the researchers visit to the school. The subjects only with parent’s consent on the day of an examination were included in the study and students absent on the day of examination, parents who declined their consent were excluded from the study.
Flow-chart showing the sampling methodology.

Dental examination of the subjects was performed in the schools during normal school hours, using a non-adjustable plastic chair under adequate natural light (Type III examination by ADA Specification) by a team headed by the researcher, who which trained for 15 days prior to the study. A detailed history of all children were recorded, which included their name, age, sex, class, religion, parents occupation, oral hygiene practice and teeth identification (FDI System). After recording history, the children were instructed to brush their teeth with a toothbrush. Teeth were isolated, quadrant by quadrant with the help of cotton rolls and then the crowns of the teeth were examined individually for the presence of dental caries using sterile mouth mirror and WHO periodontal probe. Suspected teeth with early lesions were further dried with the help of a chip blower and then coded as per the advanced ICDAS II criteria [7] [Table/Fig-2]. The observations were recorded in the separate assessment form, as given below-
Codes and description of ICDAS II.
| Codes | Criteria |
|---|
| 0 | Sound tooth surface, no evidence of caries after prolonged air drying (5 seconds) |
| 1 | First visual change in enamel: opacity or discolouration (white or brown) is visible at the entrance to the pit or fissure after prolonged air drying, which is not or hardly seen on a wet surface |
| 2 | Distinct visual change in enamel. opacity or discolouration distinctly visible at the entrance to the pit and fissure when wet, the lesion must still be visible when dry |
| 3 | Localized enamel breakdown due to caries with no visible dentine or underlying shadow: opacity or discolouration wider than the natural fissure/fossa when wet and after prolonged air drying |
| 4 | Underlying dark shadow from dentin, +/− Localised enamel breakdown |
| 5 | Distinct cavity with visible dentine: visual evidence of demineralisation and dentine exposed |
| 6 | Extensive distinct cavity with visible dentine and more than half of the surface involved |
A two-number coding system based on ICDAS CARS detection criteria was used on the teeth affected by secondary caries, in which the first digit indicated the restoration/sealants, while the following second digit represented the carious code. The suggested restoration/sealant coding system is as follows:
Caries-Associated with Restoration and Sealants (CARS) detection criteria [8].
0 = Sound: i.e. surface not restored or sealed (use with the codes for primary caries)
1 = Sealant, partial
2 = Sealant, full
3 = Tooth- coloured restoration
4 = Amalgam restoration
5 = Stainless steel crown
6 = Porcelain or gold or PFM (Porcelain Fused to Metal crown) crown or veneer or inlay or onlay or other restorative material
7 = Lost or broken restoration
8 = Temporary restoration
Results
The present study was undertaken to assess the prevalence of dental caries among school children in Pallikkaranai (corporation Zone 14, Chennai) using International Caries Detection and Assessment system (ICDAS II). A total of 2796 children with an average age ranging from 6-14 years were examined. There were 1405 males (50.3%) and 1391 females (49.7%). The prevalence of dental caries was 68.8% among the total sample studied which is highly significant [Table/Fig-3].
Prevalence of dental caries in the study population.
| Caries Status | Count | % |
|---|
| Present | 1923 | 68.8 |
| Absent | 873 | 31.2 |
| Total | 2796 | 100.0 |
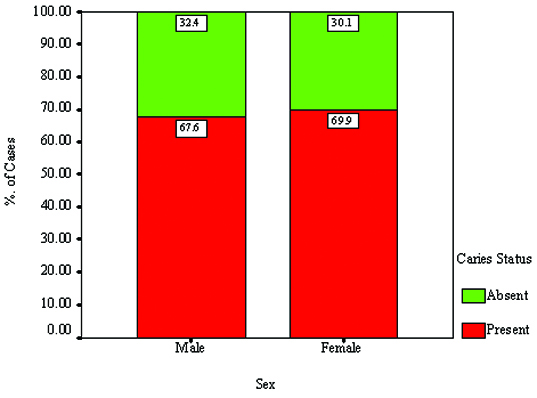
The gender wise comparison revealed that caries prevalence was higher in females (69.9%) than males (67.6%) which were not statistically significant [Table/Fig-4]. No significant relationship was found between dental caries and gender.
Showing graphical representation of dental caries based on gender.
The distribution of caries code in the study population was assessed and analysed according to ICDAS II criteria. Code 2 and 3 were the highest amongst the population, which represented non-cavitated/early lesions in the enamel [Table/Fig-5].
Distribution of Caries pattern as per ICDAS codes.
| Codes | No.of teeth present | % |
|---|
| Code 0 | 58873 | 87.97 |
| Code 1 | 463 | 0.69 |
| Code 2 | 2889 | 4.32 |
| Code 3 | 2760 | 4.13 |
| Code 4 | 918 | 1.37 |
| Code 5 | 680 | 1.02 |
| Code 6 | 337 | 0.50 |
[Table/Fig-6] shows the distribution of CARS (Caries Associated with Sealants and Restorations) in the surveyed population, which was about 1.4%.
Distribution of Secondary caries by ICDAS II (CARS Criteria).
| CARS | Count | % |
|---|
| Absent | 2757 | 98.61 |
| Present | 39 | 1.39 |
| Total | 2796 | 100.0 |
Discussion
On a worldwide basis, there has been an increase in the prevalence of caries along with emerging economies. Whereas prevalence is decreasing in developed countries due to improved oral hygiene practice and implementation of community level prevention programs [9]. However, the increase in caries prevalence is mostly due to lack of oral health care system, because this systems mostly focus on curative care, but there is no periodical implementation of community health prevention and oral health promotion [10].
Dental caries is a common dental disease occurring during childhood and it continues to be a major public health problem [11]. The World Health Organization (WHO) has ranked it as number three among all chronic non-communicable diseases that require worldwide attention for prevention and treatment [12]. ICDAS (International Caries Detection and Assessment system) is a universally accepted system to evaluate the prevalence of dental caries, in which estimation of early enamel lesions, helps in planning early treatment and monitoring caries pattern at the population level [13]. The present study was conducted in schools at Pallikkaranai (Chennai corporation zone 14) to assess the prevalence of dental caries among 6-14-years-old children using ICDAS II (International Caries Detection and Assessment System) method.
The researcher visited each school and obtained consent from the concerned school authorities. The student who gave the consent along with the filled-in questionnaire was allowed to participate in this study. The total sample comprised of 2796 students (1405- males, 1391-females) in the age of 6-14 years. Every child was assessed by the researcher who recorded the caries status using the ICDAS II criteria in the proforma and then later tabulated it for statistical analysis.
The prevalence of dental caries among the 2796 children examined for prevalence of dental caries, 1923 subjects were observed with having caries, with a prevalence rate of 68.8%. The results of this study are similar to the studies done by Joyson et al., Prabhu S et al., Alamoudi et al., and Naomi L et al., who showed the prevalence rate in the range of 61.2% to 67.2% for children between the age group of 5-15 years [14–17]. Studies reported by Mahesh KP et al., and Rajesh et al., showed higher caries prevalence (77% to 80%) in the age group of 5-12 years [18,19]. All the above mentioned studies followed DMFT/deft index to assess the dental caries prevalence, in which the early enamel lesions had not been included, whereas in the present study even including the early enamel lesion using ICDAS II, the result showed almost equivalent rate of prevalence of dental caries. This suggests that our region has a lesser prevalence of dental caries compared to other regions of Tamil Nadu and Chennai. This could be due to the role played by the dental institution situated in this region (Pallikkaranai) in creating dental health awareness camps and education along with various preventive and therapeutic measures.
Observation and comparison of the distribution of dental caries among gender in this study of 1405 males and 1391 females, showed that 950 males, and 973 females had caries. Females had a slightly higher prevalence of caries (2.3%) than males, which was not statistically significant. This result is comparable to the studies done by Kumar et al., Grewal et al., and Shingare et al., who observed higher caries prevalence in females than males with the following percentage differences of 7.1,4.16 and 1.70 respectively in the age group between 3-14 years [9,18,20]. Most of the Indian studies show more caries prevalence in females than males which could be attributed to the negative attitude of parents towards oral care for females. Ismail et al., found gender to be a dental caries predictor, with boys being more affected than girls, and this variation could be attributed to the different age group and geographic locations of that study [21].
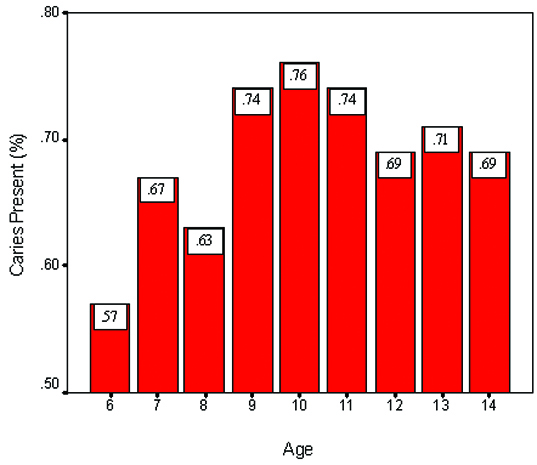
Comparing age-wise prevalence of dental caries in 6-14 year old children, this study shows an age related increase in the prevalence of dental caries until 10 years of age (from 57% to 76%) with the highest prevalence of 76% occurring at 10 years, but the caries prevalence decreased to 69% by the age of 14 years [Table/Fig-7]. This was in agreement with the studies done by Grewal et al., Goyal et al., and Dash et al., where the increase in prevalence occurred till nine years of age, after which there was a decrease in the caries prevalence until the age of 12 and 15 years [20,22,23]. They suggested higher caries prevalence with advancing age could be due to the susceptibility of newly erupted teeth to become decayed in the existing poor oral hygiene conditions. However, the reason suggested for decrease in caries prevalence after the age of 10 years was due to increase in the level of manual dexterity of the child improving the oral hygiene, increased awareness about oral health and the caries deciduous first and second molars being replaced by newly erupted premolars by the age of 12 years. Other suggested reason was the increase in the salivary IgA immunoglobulin around eight years of age [16], which inhibits the attachment and adherence of oral bacteria to the epithelial and tooth surfaces and neutralizes the bacterial exotoxins and enzymes that contribute to disease process. This same reason can even be attributed to the results of our study.
Describes the age-wise prevalence of dental caries in the studied population
The distribution of caries code in the study population was assessed and analysed according to ICDAS II. In the sample of 2796 subjects 66,900 teeth were assessed and coded by ICDAS II criteria. Among the teeth assessed 58,873 were coded 0, which is about 87.97%, while remaining 8047(12.03%) teeth were coded between 1 to 6 with values of 0.69% for code 1, 4.32% for code 2, 4.13% for code 3, 1.37% for code 4, 1.02% for code 5, 0.50% for code 6. The highest coding percentage was seen in code 2. The code 2 represents non-cavitated/early lesions in the enamel as per the ICDAS criteria, which implies the need for preventive treatment modalities so as to prevent the progression of dental caries to this study group.
In this study, there were only 39 children (1.4%) with secondary caries, which was detected by CARS (Caries Associated with Restoration and Sealants) detection criteria.
Limitation
Ideally one school should have been taken from each zone, representing the entire Chennai population but it could not be taken due to Logistic reasons, Author will be taking up a new study in which school from every zone will be taken and data from the current study will be used in the form of pilot study. Although the recordings were done by only one trained investigator, studies with inter-examiner reproducibility are also required.
Conclusion
The surfaces with early caries lesion (ICDAS code 2) are more common in the surveyed population. Careful monitoring and the preventive program could decrease the risk for dental caries and minimize the need for invasive and painful treatment procedures in the latter part of their life.
Recommendations
The recommendations to decrease the prevalence of dental caries are directed towards, improvement of brushing habits, diet modification and dental health education programs at school level. Students affected by dental caries should undergo a periodic follow up for treatment and maintenance.