Impacted Central Incisor with Dilacerated Root-Treat with Ease
Navneet Singh1, Tulika Tripathi2, Priyank Rai3, Shilpa Kalra4, Neha5
1 Senior Resident, Department of Orthodontics and Dentofacial Orthopaedics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
2 Professor and Head, Department of Orthodontics and Dentofacial Orthopaedics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
3 Professor, Department of Orthodontics and Dentofacial Orthopaedics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
4 Senior Resident, Department of Orthodontics and Dentofacial Orthopaedics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
5 Senior Research Associate, Department of Orthodontics and Dentofacial Orthopaedics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Navneet Singh, Senior Resident, Department of Orthodontics, Maulana Azad Institute of Dental Sciences, M.A.M.C Complex, B Z Marg, New Delhi-110002, India.
E-mail: dr.navneetgujjar@gmail.com
Dilacerated Impacted Central Incisor, Disimpaction, Removable Appliance
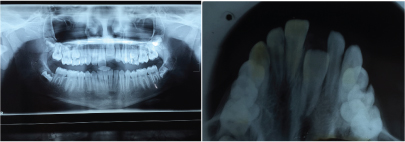
A 12-year-old female patient reported to the Department of Orthodontics of Maulana Azad Institute of Dental Sciences, New Delhi with chief complaint of missing upper front tooth. On clinical examination it was found that maxillary left central incisor (21) was missing [Table/Fig-1]. No significant history of trauma or premature/delayed shedding of primary left central incisor was reported. Panoramic and maxillary occlusal view revealed impacted left central incisor with dilacerated root [Table/Fig-2,3]. Since the contralateral central incisor had erupted fully in the mouth and the root formation of the impacted central incisor was almost complete, it was decided to disimpact the tooth (21). Disimpaction was planned by surgical exposure followed by elastic traction with the help of removable appliance. Since the patient had well aligned upper and lower arches in good occlusion, it was decided to use a modified removable appliance for extrusion of 21. A removable appliance with modified labial bow was fabricated. Labial bow in the anterior region was fabricated with 22 gauge wire and helices were incorporated in the labial bow adjacent to left central incisor region. Retention was provided by the acrylic coverage in the palatal region and by well formed retentive clasps. Surgical exposure of left central incisor was performed by open exposure technique. A bondable button was placed onto the labial surface of exposed left central incisor crown [Table/Fig-4]. Patient was trained to use elastic in triangular fashion to engage button on 21, and two helices of the labial bow, which resulted in an extrusive force of 20 grams for disimpaction of 21[Table/Fig-5] [1]. Patient was advised to change the elastic daily and was reviewed every three weeks. At the end of six months, complete disimpaction of 21 was achieved with the tooth in its optimal alignment into the upper dental arch and in good relation with lower teeth [Table/Fig-6,7]. Post disimpaction panoramic view reveals tooth 21 in the optimal position with respect to maxillary occlusal plane [Table/Fig-8].
Pretreatment intraoral maxillary occlusal photograph showing missing maxillary left central incisor.

Pretreatment panoramic and maxillary occlusal view showing vertically impacted maxillary left central Incisor with dilacerated root.
Intraoral frontal photograph after surgical exposure and with bonded attachment on labial surface of 21.

Intraoral frontal photograph showing mechanics for extrusion of 21 with elastic traction force.

Post treatment intraoral frontal and maxillary occlusal photographs showing 21 in alignment and good occlusion.

Post treatment panoramic view.

In young patients, absence of maxillary anterior teeth has a major impact on esthetics, phonetics, mastication and psychosocial well being. Impaction of maxillary permanent central incisor due to dilaceration in the root is a rare condition which is associated with trauma to primary anterior tooth early in life leading to dilaceration of permanent succedaneous tooth [2]. Depending on the severity of dilacerations, decision is usually taken to either expose and align the maxillary central incisor or extract and replace it with prosthesis. Although prognosis of disimpaction of dilacerated central incisor is questionable but orthodontic alignment was preferred in this case due to two reasons. Following extraction of a tooth, the alveolar ridge becomes deficient both vertically and labiolingually which makes it unsuitable for prosthetic implant. Also, the region becomes unaesthetic for conventional prosthetic bridge placement. Any fixed prosthesis for replacement of missing central incisor cannot be given before 18 year of age to allow for completion of alveolar bone growth in growing children [3]. The removable appliance treatment chosen for this patient was a convenient treatment option with less chair side involvement with the patient. Moreover it reduces the overall treatment time required for fully bonded fixed appliance therapy since traction could be applied to the impacted tooth immediately after removable appliance insertion. Also, one of the major advantages of using this simple appliance is that it overcomes the detrimental effects encountered with fixed appliances such as demineralization and difficulty in maintenance of oral hygiene [4].
Orthodontic extrusion of an impacted tooth is usually carried out by a trained specialist by using fixed mechanics. A modified removable appliance with bonded attachment and elastic traction has been used to successfully disimpact and align maxillary central incisor in this case. Such an appliance can be fabricated and used by even a general practitioner with basic knowledge about optimal force delivery.
[1]. Philip P, Rao A, Orthodontic extrusion of an impacted tooth with a removable appliance and a bonded attachment: a case report with relevant biomechanicsJ Inter Discip Dentistry 2014 4:46-49. [Google Scholar]
[2]. Chadwick S M, Millet D, Dilaceration of a permanent mandibular incisorBritish Journal of Orthodontics 1995 22:279-81. [Google Scholar]
[3]. Paola C, Alessandra M, Roberta C, Orthodontic treatment of an impacted dilacerated maxillary incisor: a case reportJ Clin Pediatr Dent 2005 30:93-97. [Google Scholar]
[4]. Sukontapatipark W, el-Agroudi MA, Selliseth NJ, Thunold K, Selvig KA, Bacterial colonization associated with fixed orthodontic appliances. A scanning electron microscopy studyEur J Orthod 2001 23:475-84. [Google Scholar]