Concomitant Vesicouterine Rupture with Avulsion of Ureter: A Rare Complication of Vaginal Birth after Cesarean Section
Nalini Sharma1, J Lalnunnem Thiek2, Stephen Sialo3, Santa Singh Ahanthem4
1 Assistant Professor, Department of Obstetrics and Gynaecology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
2 Senior resident, Department of Obstetrics and Gynaecology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
3 Associate Professor, Department of Urology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
4 Professor and Head Department of Obstetrics and Gynaecology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr Nalini Sharma, B 1 D, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya-793018, India.
E-mail: nalinisharma100@rediffmail.com
Uterine rupture is the most serious and life threatening complication and occurs in 0.7-0.9% of vaginal birth after lower segment caesarean section. Cases of bladder rupture along with uterine rupture have been rarely reported and avulsion of ureter, required ureteric implantation is even rarer. This case report describe a very rare case of vesicouterine rupture with avulsion of ureter following vacuum assisted delivery in a grandmulti with previous lower segment cesarean section (LSCS). Haematuria is the most common presentation of bladder rupture. Antenatal counseling regarding this entity is recommended if woman opted for vaginal birth after cesarean section. Intrapartum and postpartum high index of suspicion are important in clinching the diagnosis.
Bladder rupture, Haematuria, Uterine rupture
Case Report
A 33-year-old P7L5A1 was referred to our hospital with complaints of severe pain abdomen and bleeding per vaginum following ventouse assisted delivery 2 hours back. Past obstetric history revealed caesarean section in the fifth pregnancy which was done for transverse lie with hand prolapsed. She had one vaginal birth after caesarean section (VBAC). The patient gives a history of spontaneous onset of labour with no undue prolongation of labour. Immediately following delivery she had severe pain in lower abdomen with bleeding per vaginum.
On examination, pallor was present. Her pulse rate was 100/min and BP was 80/50mmHg. Per abdomen examination revealed 24 weeks size uterus, not well-contracted. There was severe tenderness in suprapubic region. On per vaginum examination Clear fluid (urine) was seen coming out through the vagina but there was no active bleeding. Catheterization was done and frank haematuria was noted. Urgent ultrasound was performed which showed discontinuity in lower part of anterior wall of uterus and bladder was not visualized. With a provisional diagnosis of rupture uterus with rupture bladder the patient was taken to Operation Theater.
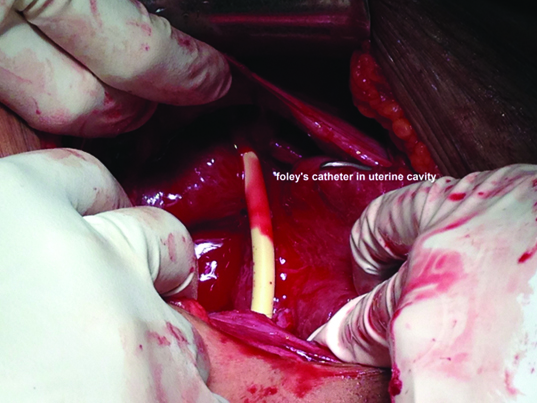
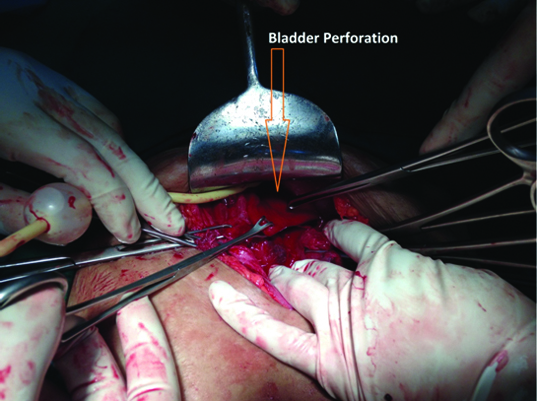
Intraoperatively, haemoperitoneum of approx.300 ml was noted. Uterine rupture was seen in the lower segment along the previous scar measuring approximately 10cm. A vertical tear was also seen in the lower segment (towards the right) extending up to the vagina. Foley’s catheter was seen in uterine cavity [Table/Fig-1]. A long transverse tear of >10 cm with ragged margins was seen in the posterior wall of the bladder [Table/Fig-2] involving the trigone with avulsion of right ureter.
Showing Foley’s catheter in uterine cavity.
Showing bladder perforation.
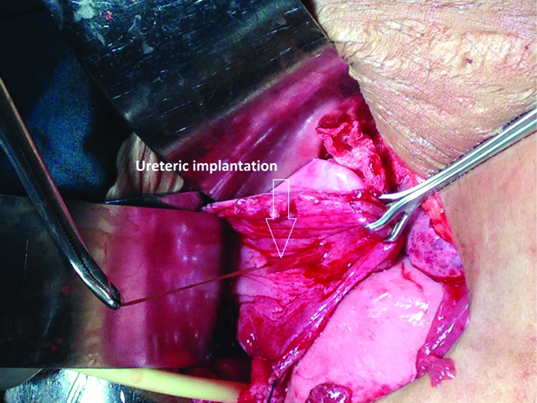
The bladder was adhered to the lower uterine segment. Bladder separation was done by sharp dissection. Repair of uterine rupture and repair of colporrhexis was done. The right ureteric orifice could not be traced. Repair of bladder and re-implantation of right ureter (ureteroneocystostomy) was done [Table/Fig-3]. Infant feeding tube was inserted in each ureteric orifice which was taken out through the urethra and Foley’s catheter was kept in situ. Patient received 2 units PRBC intra-op. Catheter was removed on 14th postoperative day. Patient was discharged well on 16th postoperative day.
Showing ureteric implantation.
Discussion
Vaginal birth after a low transverse cesarean section is considered safe and effective management to elective repeat Lower Segment Cesarean Section (LSCS) [1]. Although up to 60-80% women have successful vaginal delivery [2]. But potentially serious maternal and fetal complication occasionally follow trial of labour and Vaginal Birth After Cesarean section (VBAC).
Uterine rupture is the most serious and life threatening complication and occurs in 0.7-0.9% of vaginal birth after lower segment caesarean section [3]. it may necessitate blood transfusion, reparative surgeries and even hysterectomy. The most common Predisposing factor leading to uterine rupture is prior cesarean section [2]. Other factors are abruption placentae, mullerian anomaly, multigravida, multiple gestation, obstructed labour, uterotonic, obstetric manipulations and external trauma.
Incidence of bladder rupture associated with uterine rupture was 8-15% in various studies [2,4]. It is mostly found during cesarean section after failed VBAC [5]. Few cases are reported in which simultaneous uterine and bladder ruptured at delivery [6,7]. The clinical presentation of simultaneous uterine and bladder rupture at the time of VBAC are varied. It may be abnormal fetal heart tracing, loss of presenting part, change in uterine contour, cessation of uterine contraction, abdominal pain vaginal bleeding and shock. Gross haematuria is the most common sign of uterine rupture associated with bladder rupture [8]. Other presentation are oligouria, vernixuria, meconium stained urine, urinary incontinence [9,10]. Our patient was a grandmulti with previous one cesarean section and one VBAC. Indication of cesarean was transverse lie with hand prolapsed. It was an emergency cesarean for obstructed labour. In such setting scar healing may be poor and scar is prone for rupture during trial. Although she had one VBAC but this time she had concomitant bladder, uterine, cervical and vaginal rupture with avulsion of right ureter. Our patient did not have abnormal fetal heart tracing or intrapartum haematuria. Most probably rupture occurred during second stage. She had haematuria, incontinence of urine and severe lower abdominal pain, bleeding per vaginum following ventouse assisted delivery. Bladder and ureter involvement may be due to rupture of dense adhesions between bladder and uterus [10]. Management of these patients is surgical. It may be reparative and or hysterectomy depends on surgical findings.
Conclusion
Attending personnel should keep in mind that patient of VBAC can have bladder rupture with or without ureteric involvement along with uterine rupture. Haematuria is the most common presentation of bladder rupture. Antenatal counseling regarding this entity is recommended if a woman opted for VBAC. Intrapartum and postpartum high index of suspicion are important in clinching the diagnosis.
[1]. ACOG Practice bulletin no. 115Vaginal birth after previous cesarean deliveryObstet Gynecol 2010 116:450-41. [Google Scholar]
[2]. Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP, Risk of uterine rupture during labor among women with a prior cesarean deliveryN Engl J Med 2001 345(1):3-8. [Google Scholar]
[3]. Yap OWS, Kim ES, Laros RK, Maternal and neonatal outcomes after uterine rupture in labourAm J Obstet Gynecol 2001 184:1576-61. [Google Scholar]
[4]. Shipp TD, Zelop CM, Repke JT, Intrapartum uterine rupture and dehiscence in patients with prior lower uterine segment vertical and transverse incisionsObstet Gynecol 1999 94:735-40. [Google Scholar]
[5]. Alison GC, Molly JS, David MS, Risk factors for bladder injury in patients with a prior hysterotmyObstet Gynecol 2008 112(1):116-120. [Google Scholar]
[6]. Webb JC, Gilson G, Gordon L, Late second stage rupture of the uterus and bladder with vaginal birth after cesarean section:A case report and review of literatureJournal of Maternal –Fetal Medicine 2000 9(6):1-3. [Google Scholar]
[7]. Forsnes EV, Browing JE, Gherman RB, Bladder rupture associated with uterine rupture.A report of two cases occurring during vaginal birth after cesareanJ Reprod Med 2000 45(3):240-42. [Google Scholar]
[8]. Klutkee JJ, Klutke CG, Simultaneous bladder and uterine rupture at the time of attempted vaginal birth after cesarean sectionInt Urogynecol 1992 3:83-86. [Google Scholar]
[9]. John Patrick O, Prefontaine M, Hoffman DE, Vernixuria: Another sign of uterine ruptureJournal of perinatology 2003 23:351-52. [Google Scholar]
[10]. Ho SY, Chang SD, Liang CC, Simultaneous uterine and urinary bladder rupture in an otherwise successful vaginal birth after cesarean deliveryJ Chin Med Assoc 2010 73(12):655-59. [Google Scholar]