Basal Cell Adenoma with Perplexity in Diagnosis – A Case Report
Priyanka Kardam1, Shweta Rehani2, Yulia Mathias3, Manish Wadhwa4
1 Senior Lecturer, Department of Oral Pathology & Microbiology, Sudha Rustagi College of Dental Sciences and Research, Faridabad, India.
2 Reader, Department of Oral Pathology & Microbiology, Sudha Rustagi College of Dental Sciences and Research, Faridabad, India.
3 Head of Department, Department of Oral Pathology & Microbiology, Sudha Rustagi College of Dental Sciences and Research, Faridabad, India.
4 Head of Department, Department of General Pathology, Sudha Rustagi College of Dental Sciences and Research, Faridabad, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priyanka Kardam, D-81, Ground Floor, Saket, New Delhi -110017, India.
E-mail: priyankakardam@gmail.com
Every salivary gland tumour irrespective of its benign or malignant nature or occurrence, exhibits certain unique and overlapping histopathologic features. Basal Cell Adenoma (BCA) is a rare salivary gland tumour and hence it becomes our responsibility to report every case with unique histopathologic features so that it can add to our present knowledge of this lesion. Often, the pathologists experience difficulty while diagnosing lesions like BCA which contain basaloid cells due to its similarity with other lesions of similar histological appearance. Hence, this paper discusses a case of BCA with rare histopathologic features along with the possible differential diagnosis.
Basaloid cells, Calcification, Monomorphic adenoma, Mucin
Case Report
A 36-year-old male patient reported to the Outpatient Department of Sudha Rustagi College of Dental Sciences and Research with a chief complaint of swelling in the left posterior region of mandible since last 2-3 months. Clinically, a small hard, movable swelling was seen on the left parotid region. The patient was referred for biopsy following which a soft tissue specimen was received in the oral pathology department which was cream in colour, soft in consistency and rough in texture.
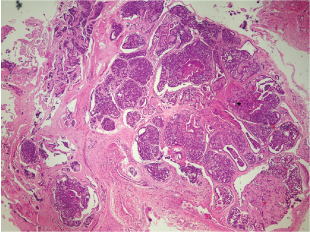
On histopathologic examination, the H&E stained soft tissue sections exhibited tumour cells arranged in various patterns, predominantly tubular and few areas of trabecular and membranous pattern [Table/Fig-1,2]. The tumour cells were basaloid and isomorphic with a hyperchromatic round to ovoid nucleus and scant eosinophilic cytoplasm and indistinct boundaries. Few islands exhibited peripheral palisading of tumour cells. Some islands exhibited areas of cystic degeneration. The stroma consisted of exuberant collections of eosinophilic mucoid insipissation with few foci of basophilic concentric calcifications. In combined Alcian Blue-PAS technique, exuberant amount of acidic mucins were observed predominantly within the tumour islands with some amount of acidic mucins in the areas surrounding these islands [Table/Fig-3]. Based on these histopathologic features, diagnosis of Basal cell adenoma (BCA) was made. Henceforth, the patient was subjected to surgical excision of the lesion as the treatment and has been kept under follow-up till date.
Scanner view of basal cell adenoma
Photomicrograph showing a scanner view of BCA; white asterisk = cribriform like areas, black asterisk = microcalcifications, red asterisk = mucoid secretion (H&E; 4X)
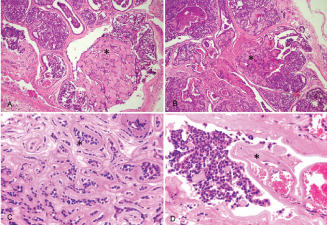
Unique features of the case.
Photomicrograph showing various unique features encountered in this case at low power: A= area showing exuberant mucoid secretion (asterisk) (H&E stain; 10X); B = area of mucoid secretion showing a basophilic tinge suggestive of microcalcifications (asterisk) (H&E stain; 10X); C= area showing membranous pattern (asterisk) of BCA (H&E stain; 40X); D = tumour cells in close vicinity of blood vessel (asterisk) (H&E stain; 40X)
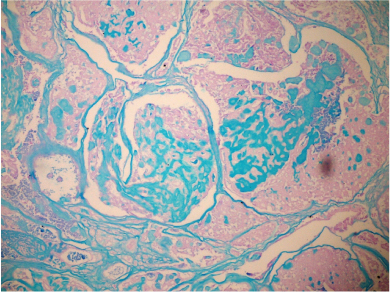
Distribution of acid mucins.
Photomicrograph showing distribution and amount of acid mucins (Blue) within and surrounding the tumour islands. (Combined Alcian Blue – PAS stain; 40X)
Discussion
Clinical classification and categorization of BCA is controversial and has been discussed by numerous authors; hence this article does not focus on this aspect [1]. Rather, we have emphasized on the unusual and typical histopathologic features of BCA. Histopathologically, the predominant cell population of BCA consists of small basaloid cells with round hyperchromatic nuclei and scant cytoplasm. However, literature has also mentioned that two populations of basaloid cells i.e. dark cells and light cells can be seen. These tumour cells can be present in various patterns like solid, trabecular, tubular and membranous with the most common type being the solid variant [2]. The tumour usually shows predominance of any one of these patterns; however a mixture of patterns can also be seen [3]. Our case, predominantly exhibited tubular pattern with some areas of membranous pattern.
In the solid type, basaloid cells are present in the form of solid masses which may show peripheral palisading creating a jigsaw puzzle like appearance. The trabecular type exhibits narrow or broad trabeculae which may get interconnected with each other creating a reticular pattern. In the tubular type, numerous tubules consisting of a central lumen and an outer single layer or double layered lining of cuboidal and basaloid cells is seen. The lumen often contains an eosinophillic secretion/mucin which is PAS positive in nature [4]. In the present case also, there were areas of eosinophillic mucin pooling and for characterisation of these mucins combined Alcian Blue-PAS technique was used as Alcian Blue-PAS sharply differentiates between acid mucins and neutral mucins [5]. In the present case this technique demonstrated acid mucins within the tumour islands and some amount surrounding these islands.
The histochemical differentiation of mucins in normal and pathological tissues is of ever-increasing importance in investigations as its composition and distribution is altered during the progression of disease [6,7]. However, there is no adequate literature which quotes the effect of these mucosubstances on prognosis and longevity of the neoplastic diseases till date.
A few of the mucin pooled areas in the present case exhibited a basophilic tinge towards the centre which was suggestive of dystrophic calcification. Some authors have already reported the presence of dystrophic calcification in cases of basal cell adenomas. Till date, there are only four reported cases of BCA with microcalcifications [8,9]. Hence the presence of areas suggestive of calcifications adds to the exclusivity of our case. It has already been hypothesized that inspissated mucoid secretions may undergo dystrophic calcification [8]. The membranous pattern of BCA exhibits tumour islands but these islands are surrounded by an eosinophilic, abundant, PAS positive, hyaline basal lamina material as observed in this case. Authors have quoted that this hyaline material may even get insinuated in between the tumour cells in form of tumour droplets [4].
It has also been reported that some BCAs may have cribriform patterns, pseudocysts of amorphous, basophilic material resembling adenoid cystic carcinoma (ADCC), which leads to confusion in diagnosis [3]. The most reliable distinguishing features between BCA with cribriform areas (cBCA) and cribriform type of ADCC are good circumscription and lack of invasive properties in BCA with cribriform areas. Also, there is absence of staining for MMP9 and laminin in the cells around the cribriform spaces in cBCA, and of calponin, SMA, or S100 in the cribriform areas in contrast with ADCC [10]. In the present case, ADCC was ruled out from the diagnosis due to lack of perineural invasion and cribriform areas.
Besides ADCC, other salivary gland tumours which exhibit basaloid cells are pleomorphic adenoma, canalicular adenoma, basal cell adenocarcinoma, basaloid squamous cell carcinoma and sialoblastoma [11]. Basal cell adenocarcinoma was ruled out because of lack of pleomorphism and absence of mitotic figures. Other differential diagnoses have been discussed in detail in [Table/Fig-4].
Salient histopathologic features helpful in differential diagnosis of BCA.
| BCA with cribriform areas | Cribriform Adenoid Cystic Carcinoma |
|---|
| Similarity: Basaloid cells arranged in cribriform pattern |
| √ Circumscription and lack of invasive properties.√ Exhibits positivity for nuclear beta-catenin, CK5/6, CD117 and S-100. | √ Exhibits acellular matrix spheres and branching matrix tubules.√ Negative for MMP9 and laminin in cells around the cribriform spaces and for calponin, SMA in the cribriform areas. |
| Solid BCA | Solid ADCC |
| Similarity: Basaloid cells arranged in form of solid masses | |
| √ Stromal material often surrounds the neoplastic cells√ Matrix material can be hyalinised√ Prominent peripheral palisading of the outer layer √ Numerous endothelial-lined channels | √ Cells almost always surround stroma√ Matrix material typically transparent√ Lack peripheral palisading of outer layer√ Lack of vascularity in microcystic areas |
| Solid BCA | Pleomorphic adenoma |
| Similarity: Basaloid cells present in form of solid masses |
| √ More uniform pattern and does not show melting of basaloid cells into stroma. | √ Chondromyxoid stroma seen |
| BCA | Basal cell adenocarcinoma |
| Similarity: Basaloid cells arranged in patterns like solid, tubular, trabecular and membranous |
| √ Encapsulated growth√ No perineural or vascular invasions | √ Invasive, unencapsulated growth into adjacent soft tissue√ Often with associated perineural or vascular invasion.√ More mitotic figures (more than 4 per 10 HPF) √ Ki 67 staining of 5% of the cells. |
| BCA with myoepithelium derived stroma | Pleomorphic adenoma |
| Similarity: Presence of myoepithelial cells |
| √ Basaloid cells are sharply demarcated from the stroma.Stroma tends to be scanty in BCA. | |
| Membranous BCA | Dermal cylindroma |
| Similarity: Nests of cells arranged in a ‘jigsaw’ pattern |
| √ Nests of BCA are more rounded | |
Conclusion
It is important to be careful while diagnosing basal cell tumours because their prognosis varies widely, for instance BCA is considered to be a non recurrent tumour with a good prognosis, basal cell adenocarcinoma is a low-grade malignancy with an excellent prognosis, while ADCC is a clinically aggressive cancer that usually requires a more extensive surgical management. So, the histopathological diagnosis of such rare lesions should be made with utmost precision in order to prevent the patient from agony of an inappropriate treatment.
[1]. Siddaraju A, Giraddi GB, Hemamythily P, Bhatt G, Nayaknur VA, Basal cell adenoma of palate- Report of a rare lesionAOSR 2013 3:51-55. [Google Scholar]
[2]. Junquera L, Gallego L, de Vicente JC, Fresno MF, Bilateral parotid basal cell adenoma: An unusual case report and rewiev of the literatureJ Oral Maxillofac Surg 2010 68:179-82. [Google Scholar]
[3]. Nagao G, Matsuzaki O, Saiga H, Sugano I, Shigematsu H, Kaneko T, Histopathologic Studies of Basal Cell Adenoma of the Parotid GlandCancer 1982 50:736-45. [Google Scholar]
[4]. Augustine D, Sekar B, Reddy VK, Gopal S, Patil S, Tubular basal cell adenoma of submandibular salivary gland: A rare case report with an unusual presentationJournal of Advanced Clinical & Research Insights 2015 2:33-35. [Google Scholar]
[5]. Naag S, Adi R, Histochemical Study Of Salivary Mucins In Normal And Neoplastic Salivary GlandsJCDR 2010 4:3450-58. [Google Scholar]
[6]. Subbuswamy SG, Pattern of mucin secretion in human intestinal mucosaJ Anat 1971 108:291-93. [Google Scholar]
[7]. Gad A, A histochemical study of human alimentary tract mucosubstances in health and disease. Normal and tumoursBr J Cancer 1969 23:52-63. [Google Scholar]
[8]. Gupta S, Rehani S, Mehendiratta M, Kumra M, Gupta R, Jain K, An unusual case report of basal cell adenoma: A Diagnostic EnchanterJ Clin Exp Dent 2014 6:599-601. [Google Scholar]
[9]. Nakamura C, Kawakami T, Hasegawa H, Shigeo EDA, Light and Electron Microscopic Studies of Microcalcifications Appearing in Monomorphic of Microcalcifications AdenomasMatsumoto Shigaku 1987 13:329-36. [Google Scholar]
[10]. Li BB, Zhou CX, Jia SN, Basal cell adenoma of salivary glands with a focal cribriform pattern: clinicopathologic and immunohistochemical study of 19 cases of a potential pitfall for diagnosisAnn Diagn Pathol 2014 18:5-9. [Google Scholar]
[11]. Gupta N, Jadhav K, Ahmed MB, Amberkar VS, Basal cell adenoma in a relatively rare siteJ Oral Maxillofac Pathol 2009 13:101-04. [Google Scholar]