Effect of Seven Sessions of Posterior-to-Anterior Spinal Mobilisation versus Prone Press-ups in Non-Specific Low Back Pain – Randomized Clinical Trial
Shlesha G Shah1, Vijay Kage2
1 Assistant Professor, SPB Physiotherapy College, Surat, India.
2 Assistant Professor, KLE University’s Institute of Physiotherapy, Belgaum, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shlesha G Shah, SPB Physiotherapy College, Surat, Gujarat-395009, India.
E-mail: drsmvaidya@gmail.com.
Introduction
Low back pain is non-specific in 85% of population. Posterior-to-anterior (PA) mobilization and press-up exercises are common physical therapy interventions used to treat low back pain.
Aim
The purpose of this study was to investigate the effect of posterior-to-anterior spinal mobilization and prone press-ups in non-specific low back pain.
Materials and Methods
The study design was double blind randomized clinical trial. Forty participants reporting to Physiotherapy Out-patient department in hospital who were 18-45 years of age and had diagnosis of non-specific low back pain were included. Primary outcome measures were lumbar extension range, pain and physical function.
Results
Both interventions resulted in significant reduction in the average pain scores for both groups. Similarly, gain in total lumbar extension was significant in both the PA mobilization group and the press-up group. Functional scores significantly improved for both the groups. Both the groups significantly differed in terms of pain, lumbar extension and functional scores. PA mobilization proved to be a superior intervention.
Conclusion
PA mobilization and press-ups can be used as an effective intervention in non-specific low back pain.
Maitland mobilisation, Mckenzie exercises, Low back
Introduction
Non-specific low back pain is pain not attributed to a recognisable pathology. Low back pain is non-specific in 85% of population. Fear of movement and reinjures lead to inactivity and disability [1]. Low back pain is often associated with reduced spinal motion. Lumbar extension is frequently more restricted than flexion. Pain and stiffness can result in reduced spinal extension which can be general or segmental [2]. The conservative treatment of low back pain includes electrotherapy, exercise therapy and manual therapy. Manual therapy includes Maitland’s spinal mobilisation, Mulligan’s Mobilisation with Movement, soft tissue techniques like Muscle Energy technique, Positional Release therapy, myofascial release, neuromuscular technique [3]. Spinal mobilization and range-of-motion exercises improve spinal motion. Manual therapy techniques are delivered based on the assessment of limitation in active or passive joint motion [4,5].
Postero-anterior central vertebral pressure can be used to treat pain which is evenly distributed to both sides of lumbar spine. This technique is indicated when pain or muscle spasm is felt on movement in this direction but it is performed in such a way that pain or spasm is not provoked [5]. Wyke stated that all spinal mechanical pain is caused by mechanical deformation of soft tissues containing nociceptors [6].
Robin Mckenzie developed a new concept of diagnosis and treatment based on systematic analysis of patients with both acute and chronic back problem [7]. Mckenzie stated that all spinal mechanical pain can be classified into three syndromes: the postural, dysfunction and derangement syndrome. In Mckenzie approach to mechanical disorders, both diagnosis and treatment are based on the symptom behaviour observed during and after repeated movement-testing. The postural faults lead to soft tissue dysfunction being loss of lumbar extension. As a treatment, stretching procedures to the end available range are ideally performed in slow repeated fashion. McKenzie and May targeted general spinal motion in which a press-up exercise is used as a means of increasing spinal motion [8]. Extension exercises are frequently used to rehabilitate patients with back dysfunction [9]. Increased spinal mobility leads to low back pain improvement. Hence, spinal mobility exercises can be recommended to low back patients [10].
The previous study comparing the efficacy of single session of posterior-to-anterior mobilisation and prone-press ups revealed immediate effect on symptoms and lumbar motion in people with nonspecific low back pain. Long term gains in pain reduction and lumbar extension could not be assumed as only single session of intervention was studied [11]. Therefore there is lack of evidence for clinical effectiveness of postero-anterior spinal mobilisation and prone press-ups on lumbar extension in non-specific low back pain. Hence this study intend to prove the effect of postero-anterior mobilisation and prone press ups on non-specific low back pain after seven sessions and their clinical application.
Materials and Methods
Forty participants with low back ache in the age group of 18-45 years who reported to the Physiotherapy outpatient department were screened clinically for the evidence of non-specific low back pain. Participants who reported a recent onset of low back pain (duration of <3 months) and the following signs and symptoms were admitted over a period of one year from February 2011 to January 2012; localized low back pain at or above the waist level, decreased lumbar extension (assessed qualitatively while standing), and increased localized pain with lumbar extension during standing.
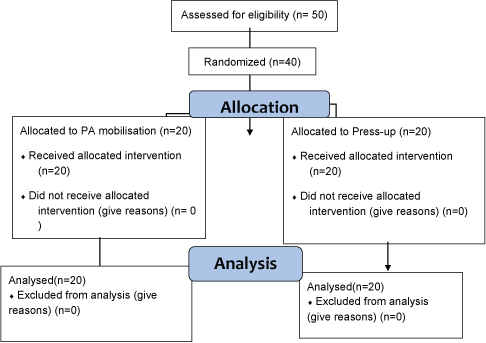
Exclusion criteria included history of spinal surgery, subjects administered epidural injection, Low Back Pain because of any specific pathology, any clinical condition that contraindicates Mobilization, subjects with neurological deficits, knee and ankle pathology causing limitation of motion, subjects with psychological low back pain, subjects with mental disorders, any history of injury in past 3 months, hyper-mobility and neurological impairments. Participants signed consent form approved by institutional review committee of KLE University. Simple randomisation was employed using computer generated table of random numbers. One investigator managed the assignment scheme and provided the assignment to the treating physiotherapists in a series of consecutively numbered opaque envelopes. Allocation was concealed from the outcome assessor and participants at all times and from the physiotherapist until the point of treatment. Both the groups received the selected treatment for seven consecutive days [Table/Fig-1].
Flow diagram depicting entire procedure of the study.
Measurements
Outcome measures included pain measured by Visual Analogue scale which is a 10 cm straight line with numbers 0 to 10 where 0 symbolises no pain and 10 symbolises the worst tolerable pain [12]. Participants were asked to mark a point on this line as per the severity of pain which indicates present pain level. Lumbar extension range measured by modified Schober method. With the participant in standing position, examiner marks a mark approximately at fifth lumbar vertebra, then one finger 10cm above the mark and another 5 cm below the mark [13]. Then the participant was asked to bend backwards with hands on hips. The reduction in distance between the two points is measured by a measuring tape. The function was assessed by Modified Oswestry Disability Questionnaire. Each item was scored from 0-5. The maximum score was therefore 50. The obtained score can be multiplied by 2 to produce a percentage score [14]. Outcome measures were assessed prior to intervention, immediately after the first session of intervention and at the end of seven sessions of intervention.
Intervention
Participants assigned to group A were first put prone on treatment table with pillow under abdomen. First, the investigator applied PA pressure to the spinous process of each lumbar vertebra using small amplitude movements (grade I). The pressure should reproduce the discomfort experienced while bending backward in standing. If no pain was reproduced with grade 1 of mobilisation then further higher grades were used (grades II–IV). Once the vertebral level where discomfort similar to bending backward in standing was identified, session of mobilisation was initiated. Initially, the most painful lumbar segment was treated with graded posterior-to-anterior oscillations. Three bouts of 40-second oscillations were applied to this segment at a frequency of 1 to 2 Hz and at the amplitude tolerated by the patient. Following mobilization of the most painful segment, 2 bouts of 40-second oscillations (up to grade IV but short of symptom reproduction) were administered to each of the remaining lumbar vertebral levels. The total time for the PA mobilization intervention was approximately 10 minutes [6]. Participants assigned to Prone press-ups were asked to perform a press-up manoeuvre as far as possible without reproducing lumbar pain with standing extension. Initially the participants were prone on a treatment table with pillow under abdomen. The participant pressed the top half of the body upward into spinal extension, while the pelvis remained on the treatment table. The participant was instructed to move to maximum pain-free lumbar extension. The end-range position was held for 5 seconds. Ten repetitions were performed. For each repetition, the participant moved slightly higher, within the limits of discomfort. If the participants could successfully complete 10 repetitions without increase in discomfort then a second and third series of press-up manoeuvres were performed. All participants completed 30 repetitions. Approximate time taken for the entire session was 10 minutes [8].
Statistical Analysis
Paired t-test was used for within group comparisons and unpaired t-test for between group comparisons, p-value set at less than 0.05. All power calculations were based on an alpha level of 0.05 for a one-tailed test.
Results
Average pain scores were lower after intervention than before intervention in both the groups. Subjects in the PA mobilization group reported a post-treatment pain score of 1.6±1.0, which did differ significantly from the post-treatment pain score of 3.2±1.43 reported by subjects in the press-up group. Average lumbar extension was greater after intervention than before intervention across both the groups. On an average subjects in PA group demonstrated 5.1±0.7 cm of lumbar extension which differed significantly from post-treatment lumbar extension of 3.2±1.1 as demonstrated by press-up group. Average disability scores were lower after intervention than before intervention in both the groups. Subjects in PA group reported post-treatment score of 5.3±6.1 which differed significantly to post-treatment score of 18.6±7.4 as reported by press-up group [Table/Fig-2,3].
Intra-group comparison of outcome measures using paired t-test.
| Outcome Measure | Group A | p | Group B | p |
|---|
| Pre | Post | Post-7day | Pre | post | Post -7 day |
|---|
| VAS (cm) | 6.9±1.4 | 3.8±1.4 | 1.6±1.0 | <0.05 | 6.6±1.2 | 4.6±1.2 | 3.2±1.43 | <0.05 |
| MODQ | 40.7±11.5 | 27.5±10.7 | 5.3±6.1 | <0.05 | 38.1±11.1 | 34.2±10.6 | 18.6±7.4 | <0.05 |
| ROM (cm) | 1.8±0.7 | 3.8±0.8 | 5.1±0.7 | <0.05 | 1.6±0.8 | 2.6±1.1 | 3.2±1.1 | <0.05 |
Inter-group comparison of outcome measures using unpaired t-test.
| Outcome Measure | Group A | Group B | p | Group A | Group B | p |
|---|
| Pre-Post | Pre-Post | Pre-Post 7 days | Pre-Post 7 days |
|---|
| VAS (cm) | 3.11 | 2.03 | <0.05 | 5.91 | 3.38 | <0.05 |
| MODQ | 13.21 | 3.90 | <0.05 | 35.42 | 19.52 | <0.05 |
| ROM (cm) | 2.01 | 0.97 | <0.05 | 3.34 | 1.60 | <0.05 |
Discussion
The age group of the participants was in range of 18 to 45 years. Participants above 45 years of age experience low back pain due to degenerative changes in lumbar spine. Hence participants above 45 years of age have not been included in the study as the study involves nonspecific low back pain. In present study age distribution and anthropometric variables showed no statistical difference in the groups which represents the homogeneity of participants.
Sample size of present study consisted of 27 females and 13 males that are 65.5% females and 34.5% males. This concludes females are more prone than males for developing low back pain and correlates with findings reported in several other studies [15]. Significant relief of pain was noted in both groups over sessions for 7 days. In the present study, pain was measured by Visual Analogue scale. Oloagan et al., compared reliability of rating low back pain with Visual Analogue Scale and Semantic Differential Scale, concluded that Visual Analogue Scale had superior reliability and validity in rating low back pain [12]. Both the interventions showed statistically significant improvement in terms of pain. Posterior-to-anterior spinal mobilisation proved to be superior in terms of reduction of pain. In the present study reduction in pain level, as quantified by the Visual Analogue Score (VAS), with the application of both postero-anterior mobilisation and prone press-ups is consistent with the findings of previous studies indicating both the techniques reduced low back pain. On average total lumbar extension increased by 3.9 cm following PA mobilisation and 1.6 cm following press-ups. The gain in spinal motion was higher after seven sessions as compared to single session. Several studies have proved short term effects of single session of spinal mobilisation. Moreover, single session of spinal mobilisation, as seen in previous studies has shown statistically significant improvement in extension range but not clinically relevant improvements. Hence, this proves that several sessions of spinal mobilisation are necessary to produce clinically relevant results.
Both the interventions have mechanical and neuro-physiological effect. Passive motion selectively stretches contracted tissues there by increases motion [16]. Muscle spindle afferents and Golgi tendon organ afferents are stimulated by spinal manipulation. Spinal manipulation corrects the altered biomechanics resulting in sensory modulation. Numerous studies show that spinal manipulation increases pain tolerance or its threshold. Painful stimuli will evoke reflex parasympathetic activity. Manipulation has the ability to remove noxious mechanical or chemical stimuli from paraspinal tissues and hence modulate central sensory processing. Spinal manipulation is also thought to affect reflex neural outputs to both muscle and visceral organs. Literature reveals that spinal manipulation elicits paraspinal muscle reflexes and increases motor neuron excitability producing increased recruitment of these musculature [17]. Moreover, repetitive movements enhance the distribution of synovial fluid over the articular cartilage and disk, resulting in less resistance to motion [18]. With the reduction in resistance, movement becomes smooth leading to reduction in pain.
Joint mobilisation reduces dorsal horn activation from a painful stimuli [19]. Several authors have reported elevated pain threshold levels with passive movements to spine [20,21] or the extremities [22–24].
Press-ups manoeuvre might have resulted in decreased muscle guarding leading to increased motion. Mobilisation is known to cause transient inhibitory effect on alpha motor neurons leading to reduced muscle guarding [25]. Pain reduction reported in the present study following PA mobilisation was 78.5% which was consistent with findings of other studies. Chiradejnant et al., reported a 36% reduction in pain following two 1-minute bouts of spinal mobilization in subjects with nonspecific low back pain [16]. Goodsell et al., reported an average pain reduction of 33% following PA mobilisation in subjects with non-specific low back pain [26]. There was 50% pain reduction following press-ups in the present study. Above studies failed to report significant increase in lumbar extension. This is in contrast to the present study in which mobilisation significantly increased lumbar extension range. McCollam and Benson, reported a 7.1% increase in lumbar extension on application of three 1 minute bouts of posterior-to-anterior mobilisation at L3, L4 and L5 [17]. Christopher P, performed a clinical trial on non-specific low back pain and compared the effect of single session of postero-anterior spinal mobilisation and prone press-up. There was significant reduction in the average pain scores for both groups. Similarly, total lumbar extension significantly increased in both the PA mobilization group and the press-up group. However, percentage increase in lumbar extension was greater in mobilisation group [11].
The UK evidence report on the effectiveness of Manual Therapies reviewed the literature and concluded that spinal manipulation/mobilization has moderate quality positive evidence supporting its utilization in the treatment of acute low back pain and high quality positive evidence in treatment of chronic low back pain [27]. Fritz JM reported that Modified Oswestry Disability Questionnaire showed higher levels of test-retest reliability and responsiveness as compared to Quebec Back Pain Disability Scale in subjects with low back pain [14]. In the present study, when the means of Modified Oswestry Disability Questionnaire (MODQ) were analysed, statistically significant improvement was found in both groups and has shown reduced MODQ scores which represent reduction in pain and an improvement in range of motion and functional activities. Mobilisation proved to be superior in reducing functional disability as compared to press ups. Low back pain presents a serious health care problem and produces a huge burden on society. Simple, safe, physical treatment procedures such as posterior-anterior spinal mobilisation and prone press-ups combined with other simple non-invasive intervention such as moist pack could be of great value. This provides a low cost, easy means of treatment in subjects with non-specific low back pain.
Limitations
Several limitations of this study need to be addressed. The findings of this study cannot be generalised to all low back pain patients as subjects with only non-specific low back pain were considered. There is lack of control group in the study so placebo effect that might have occurred due to any of these interventions cannot be commented upon. The subjects have not been followed up to see the long term sustenance of improvement due to both interventions. These limitations need to be addressed in future investigations.
Conclusion
Participants in both groups reported significantly less pain with bending backward in standing. Lumbar extension significantly improved with both PA mobilization and the press-up exercise. There were significant differences in pain and lumbar extension between the two interventions studied. PA mobilisation proved to be superior in reducing pain and increasing lumbar extension resulting in improved functional outcome.
[1]. Bigos S, Bowyer O, Braen G, et al. Acute Low Back Problems in Adults. Clinical Practice Guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD: Agency for Health Care Policy and Research, Public Health Service, U.S. Department of Health and Human Services. December 1994 [Google Scholar]
[2]. Mellin G, Decreased joint and spinal mobility associated with low back pain in young adultsJ Spinal Disord 1990 3(3):238-43. [Google Scholar]
[3]. Anderson G, The epidemiology of spinal disorders. In: Frymoyer JW, editorThe adult spine: principles and practice 1997 2nd editionPhiladelphiaLippincott-Raven [Google Scholar]
[4]. Beurkens AJ, Efficacy of traction for non-specific low back pain. 12 week and 6 months results of a randomized clinical trialSpine 1997 22(23):2756-62. [Google Scholar]
[5]. Maitland GD, Maitland’s Vertebral Manipulation 2005 7th editionLondon, UKButterworth-Heinemann [Google Scholar]
[6]. Wyke BD, Neurological aspects of low back painThe lumbar spine and low back pain 1976 LondonSector Publishing Ltd:198-237. [Google Scholar]
[7]. Mckenzie R, May S, The Lumbar Spine: Mechanical Diagnosis & Therapy 2003 Waikanae, New ZealandSpinal Publications New Zealand Ltd [Google Scholar]
[8]. McKenzie RA, The Lumbar SpineMechanical Diagnosis and Therapy 1981 1st ed [Google Scholar]
[9]. Stankovic R, Johnell O, Conservative treatment of acute low back pain. A prospective randomised trial: Mckenzie method of treatment versus patient education in “mini back school”Spine 1990 15(2):120-23. [Google Scholar]
[10]. Van Wijmen M, The management of recurrent low back painModern manual therapy of the vertebral column. Ed. Grieve GP Ch 73 1986 :756-776. [Google Scholar]
[11]. Powers CM, Effect of single session of Posterior to Anterior Spinal Mobilisation and Press-Up Exercises on Pain Response and Lumbar Spine Extension in People with Non-Specific Low Back PainPhys Ther 2008 88(4):485-49. [Google Scholar]
[12]. Olaogun MOB, Adedoyin RA, Ikem IC, Anifaloba OR, Reliability of rating low back pain with a Visual Analogue Scale and Semantic Differential ScalePhysiotherapy Theory and Practice: An International Journal of Physiotherapy 2002 20(2):135-42. [Google Scholar]
[13]. Beattie P, Rothstein JM, Lamb RL, Reliability of attraction method for measuring lumbar spine backward bendingPhys Ther 1987 67:364-69. [Google Scholar]
[14]. Fritz JM, Irrgang JJ, A comparision of a modified Oswestry Disability Questionnaire and the Quebec Back Pain Disability SclePhys Ther 2001 81:776-88. [Google Scholar]
[15]. Schneider S, Randoll D, Buchner M, Why do women have back pain more than man? A representative prevalence study in the federal republic in GermanClin J Pain 2006 22:738-47. [Google Scholar]
[16]. Chiradejnant A, Latimer J, Maher CG, Stepkovitch N, Does the choice of spinal level treated during Postero-anterior mobilization affect treatment outcome?Physiother Theory Prac 2002 18(4):165-74. [Google Scholar]
[17]. McCollam R, Benson C, Effects of postero-anterior mobilization on lumbar extension and flexionJournal of Manual and Manipulative Therapy 1993 1:134-41. [Google Scholar]
[18]. Twomey L, Taylor J, Exercises and spinal manipulation in treatment of low back painSpine 1995 20(5):615-19. [Google Scholar]
[19]. Malisza KL, Stroman PW, Turner A, Gregorash L, Foniok T, Wright A, Functional MRI of rat lumbar spinal cord involving painful stimulation and effect of peripheral joint mobilizationJ Magn Reson Imaging 2003 18:152-59. [Google Scholar]
[20]. Paungmali A, O’Leary S, Souvli ST, Vicenzino B, Naloxone fails to antagonize initial hypoalgesic effect of manual therapy treatment for lateral epicondylalgiaJ Manipulative Physiol Ther 2004 27(3):180-85. [Google Scholar]
[21]. Dhondt W, Willaey ST, Verbruggen LA, Pain threshold in patients with rheumatoid arthritis and effect of manual oscillationsScand J Rheumatol 1999 28:88-93. [Google Scholar]
[22]. Moss P, Sluka K, Wright A, The initial effects of knee joint mobilization on Osteoarthritis hyperalgesiaMan Ther 2007 12(2):109-18. [Google Scholar]
[23]. Paungmali A, O’Leary S, Souvli ST, Vicenzino B, Hypoalgesic and sympathoexcitatory effects of mobilization with movement for lateral epicondylalgiaPhysTher 2003 83:374-83. [Google Scholar]
[24]. Vicenzino B, Paungmali A, Buratows Ki J, Wright A, Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesiaMan Ther 2001 6:205-12. [Google Scholar]
[25]. Dishman JD, Bulbulian R, Spinal reflex attenuation associated with spinal manipulationSpine 2000 25:2519-24. [Google Scholar]
[26]. Goodsell M, Lee M, Latimer J, Short-term effects of lumbar postero-anterior mobilization in individuals with low-back painJ Manipulative and Physiol Ther 2000 23(5):332-42. [Google Scholar]
[27]. Bronfort G, Haas M, Evans R, Leininger B, Triano J, Effect of manual therapies: The UK evidence reportChiropractic and Osteopathy 2010 18:3 [Google Scholar]