Microleakage in Sub-Gingival Class II Preparations Restored Using Two Different Liners for Open Sandwich Technique Supplemented With or Without Ultrasonic Agitation: An In Vitro Study
Hitesh Chandar Gyanani1, Naveen Chhabra2, Nimisha Chinmay Shah3, Pratik Subash Jais4
1 Post Graduate Student, Department of Conservative Dentistry and Endodontics, K.M. Shah Dental College and Hospital, Sumandeep Vidyapeeth, India.
2 Reader, Department of Conservative Dentistry and Endodontics, K.M. Shah Dental College and Hospital, Sumandeep Vidyapeeth, India.
3 Professor and Head, Department of Conservative Dentistry and Endodontics, K.M. Shah Dental College and Hospital, Sumandeep Vidyapeeth, India.
4 Post Graduate Student, Department of Conservative Dentistry and Endodontics, K.M. Shah Dental College and Hospital, Sumandeep Vidyapeeth, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hitesh Chandar Gyanani, Post-Graduate Student, Department of Conservative Dentistry and Endodontics, K.M. Shah Dental College and Hospital, Sumandeep Vidyapeeth Vadodara-391760, India.
E-mail: hiteshgyanani89@gmail.com
Introduction
Probability of bond failure at sub-gingival cavosurface margin is high in class II cavity designs especially when margins are located in cementum or dentin. Previous researches have proved ultrasonics to be a beneficial tool in improving the marginal adaptation of the restorative material. Therefore, the effect of ultrasonic activation of the lining material at the gingival cavosurface margin was tested in the present research.
Aim
The study aimed to evaluate the cervical micro-leakage in class II preparations with gingival margin located below cemento enamel junction and restored using open sandwich technique using two different liners and supplemented with or without ultrasonic agitation.
Materials and Methods
Forty recently extracted human molars were collected, disinfected and stored in 0.9% saline solution. Standar dized class II cavities were prepared with gingival margin located 1mm below the cemento-enamel junction. Teeth were randomly divided into four groups (n=10) and restored using open sandwich technique as follows - Group A: Resin Modified Glass Ionomer Cement as liner and Beautifil II as coronal restoration; Group B: Same as group A supplemented with ultrasonic agitation; Group C: Beautifil Flow Plus as liner and Beautifil II as coronal restoration; Group D: Same as Group C supplemented with ultrasonic agitation. Prepared samples were subjected to thermo cycling, followed by immersing in 0.5% methylene blue dye solution. After 24 hours they were cleaned and sectioned in mesio-distal direction using diamond disc and evaluated for microleakage. Obtained scores were statistically analysed using one way ANOVA test and Post Hoc test.
Results
Group B showed least microleakage amongst all groups but the results were statistically insignificant (p value > 0.05).
Conclusion
Marginal adaptation of liner with ultrasonic activation was somewhat better however, the results were statistically insignificant.
Dental leakage, Liner, Methylene blue
Introduction
Despite recent advances in adhesive materials, poor adaptation and dental leakage remain the prime reasons for the restoration failure. The probability of bond failure is high especially when the gingival margin is located in cementum or dentin due to incomplete penetration of the bonding agent and polymerisation shrinkage stresses [1].
Several approaches have been suggested to overcome such problems which include modification in both material as well as technique. Incremental layering technique, soft start or ramp curing and sandwich technique are to name a few [2–4].
Sandwich technique, introduced by Mclean, is mainly indicated in large class I, II III, IV and V direct composite restorations. It can either be open or closed [5]. Both types of sandwich techniques differ as in open method all restorative materials are exposed to oral cavity at the proximal margins as compared to the closed variant. The chief reason for failure of open sandwich technique was the continuous loss of base material (primarily GIC) [6]. To counteract this various hybrid ionomers have been introduced which include resin modified glass ionomer and giomer [6–8].
Giomer is based on the pre-reacted glass technology and is commercially available in two types either Surface Pre-Reacted Glass (S-PRG) or Full Pre-Reacted Glass (F-PRG) as nano-sized multifunctional fillers. Giomers bear the advantages of both composite resin and glass ionomers. Like composite they have excellent aesthetics, good polishability, and biocompatibility and on the other side they exhibit glass ionomer like properties as well, like fluoride release and fluoride recharge potential [9]. Proper seal against bacterial micro leakage and minimal mechanical and chemical irritation of the pulp are the other advantages of giomers [10]. According to the manufacturer, commercially available S-PRG based Giomer (Beautifill Flow plus®, Shofu Inc., Kyoto, Japan) combines the delivery of a flowable composite and the strength of conventional hybrid composite resin, durability and aesthetics equal to or better than leading hybrid composites and is approved for restoration of all types of defects including the occlusal surface and proximal margins [11]. Beautifil II® (Shofu Inc., Kyoto, Japan) is yet another material with excellent properties including filler structure that has been developed to simulate the internal structure of natural teeth with ideal light transmission and optical characteristics [12].
Literature search reveals that the ultrasonic energy has been used during the curing of GIC with promising results. Ultrasonically activated GIC showed increased hardness, decreased surface soft layer and better marginal adaptation [13]. However, to the best of our knowledge there is no research in which ultrasonic activation has been tested along with resin modified glass ionomer and giomer in obtaining better gingival margin adaptation.
Aim
The present study aimed to evaluate cervical microleakage in class II preparations with gingival margin located below cemento-enamel junction and restored using open sandwich technique with or without application of ultrasonic activation. The null hypothesis for the present study stated that ultrasonic activation of lining material shall have no effect on microleakage.
Materials and Methods
This in vitro study was conducted in the Department of Conservative Dentistry and Endodontics, K. M. Shah Dental College and Hospital, Piparia, Vadodara. Prior permission from the institutional ethics committee was taken before the commencement of the study (Ethical Approval number - SVIEC/ON/Dent/SRP/15045). The study duration was six months from the date of obtaining ethical approval till the completion of the same.
Sample description: The sample sizes of 40 (10 per group) was decided for the present study. The total sample of 40 tooth specimens achieved 80% power to detect differences among the means versus the alternative of equal means using an F test with a 0.05000 significance level. The size of the variation in the means was represented by their standard deviation which was 3.00. The common standard deviation within a group was assumed to be 0.50.
Formula – (Zα+Zβ)2*√(n*delta2/2kS2)
Z alpha and Z beta are valued from normal tables; Delta is mean difference between groups; S is standard deviation and K is number of groups.
Where Z alpha=1.96
Z beta=0.84
Delta= 3.00; Mean Difference
S = Common Standard deviation= 0.50
K= Degree of Freedom = n-1=3
n= Total Number of Groups=4
Methodology Proper: Forty recently extracted intact human molars indicated for extraction were collected and cleaned using ultrasonic scaler and disinfected by immersing them in 0.5% chloramine T solution for 15 days. Thereafter the teeth were stored in distilled water until use. Class II cavities (3mm wide, 6mm high and 2mm deep) were prepared on the proximal surfaces with the help of straight fissure bur with gingival margin located 1mm below cemento-enamel junction. Dimensions of class II cavities were calibrated using digital Vernier’s calliper. The prepared teeth were mounted between two dummy teeth using silicone impression putty to reproduce proximal contact. Pre-contoured transparent matrix bands and light transmitting wedges were used to establish proper proximal contact and contour of the restoration. Teeth were then randomly divided into four groups (n=10) and restored as per group protocol [Table/Fig-1].
Description of restorative procedures.
| Group | Description |
|---|
| Group A | Dentin conditioner applied for 20 seconds followed by application of resin modified glass ionomer cement as a liner in 1mm increment which was light cured (LEDition, Ivoclar Vivadent, Europe) according to manufacturer’s instructions. Bonding agent was applied on the surface of glass ionomer base, (Beautibond®, Shofu Inc., Kyoto, Japan) light cured according to manufacturer’s instructions and subsequent restoration was carried out with Beautifil II® (Shofu Inc., Kyoto, Japan) using the incremental layering technique. |
| Group B | Dentin conditioner was applied for 20 seconds followed by application of resin modified glass ionomer cement (Fuji II LC, GC, Japan - used as a liner) in 1mm increment which was ultrasonically activated and then light cured according to manufacturer’s instructions followed by subsequent restoration as for group A. |
| Group C | Two consecutive coats of bonding agent (Beautibond®, Shofu Inc., Kyoto, Japan) were applied onto the cavity walls and light cured for 10 seconds. Beautifil Flow Plus F 03® (Shofu Inc., Kyoto, Japan) was placed as liner in 1mm increment using syringe delivery system which was light cured according to manufacturer’s instructions followed by subsequent restoration of remaining preparation as for group A. |
| Group D | Two consecutive coats of bonding agent (Beautibond®, Shofu Inc., Kyoto, Japan) were applied onto the cavity walls and light cured for 10 seconds. Beautifil Flow Plus F 03® (Shofu Inc., Kyoto, Japan) was placed as a liner in 1mm increment using syringe delivery system which was then ultrasonically activated and light cured according to manufacturer’s instructions, followed by subsequent restoration of remaining preparation as for group A. |
Restored teeth were finished, polished and stored in distilled water at 37°C for seven days. The teeth were then subjected to thermo cycling for 500 cycles (5°C & 55°C, dwell time 15 seconds). Each tooth was covered with two coats of nail varnish except for the area 1mm away from gingival margin of the restoration. Thereafter, all the samples were immersed in 0.5% methylene blue dye solution for 24 hours. The samples were then cleaned and sectioned in mesio-distal direction using diamond disc. Both sections were evaluated at the gingival margin and to stay on the conservative side only section with worst score (greater amount of microleakage) was recorded. The evaluation was done using stereomicroscope (Motic, Causeway Bay, Hong kong) at 40X magnification [Table/Fig-2].
Stereomicroscopic images of representative specimen from each group at 40X magnification. A: Group A; B: Group B; C: Group C; D: Group D.
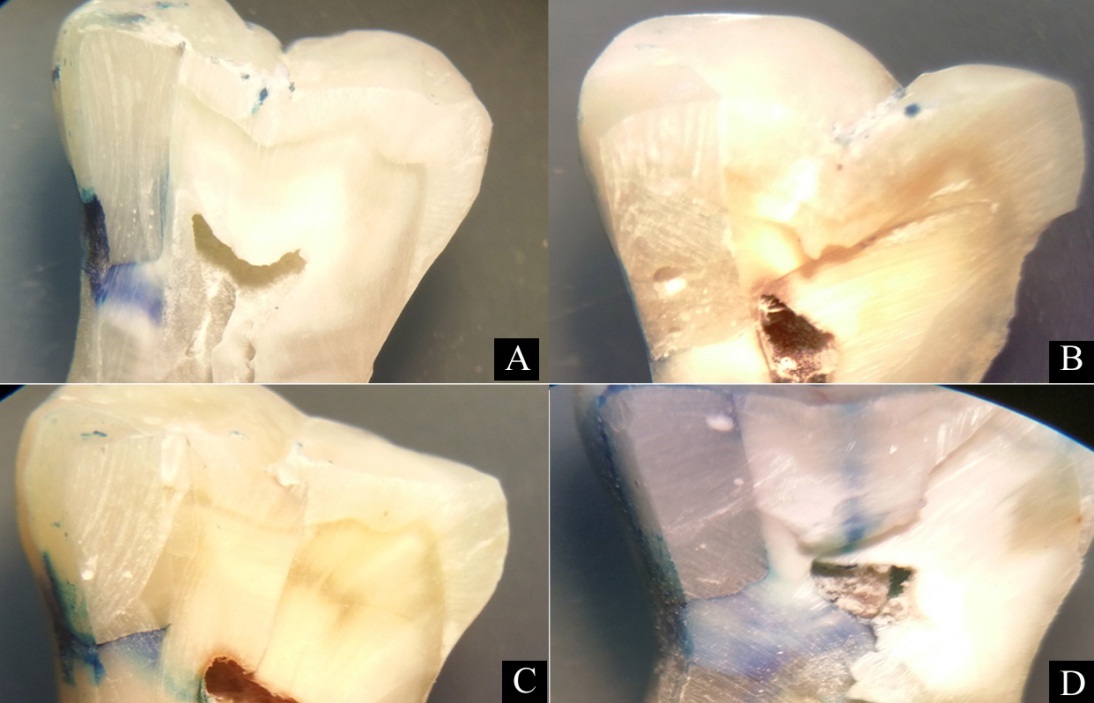
The severity of dye penetration was evaluated using the scoring criteria suggested by Loguercio et al., [14] as follow: Score 0- No dye penetration; Score 1- Dye penetration up to one half of the gingival floor; Score 2-Dye penetration up to more than one half of the gingival floor; and Score 3- Dye penetration up to the axial wall [Table/Fig-3]. Obtained scores were statistically analysed using one way ANOVA test and Post Hoc test.
Master chart showing microleakage scores.
| GROUPS | A(RMGIC) | B(RMGIC withUltrasonic Activation) | C(Beautifil FlowPlus F 03) | D(Beautifil FlowPlus F 03 withUltrasonic Activation) |
|---|
| Tooth Specimen | Score | Score | Score | Score |
| I. | 1 | 1 | 2 | 2 |
| II. | 0 | 0 | 0 | 2 |
| III. | 2 | 0 | 2 | 0 |
| IV. | 0 | 1 | 2 | 1 |
| V. | 2 | 1 | 3 | 2 |
| VI. | 1 | 0 | 2 | 3 |
| VII. | 0 | 1 | 1 | 0 |
| VIII. | 3 | 2 | 0 | 1 |
| IX. | 1 | 0 | 0 | 0 |
| X. | 3 | 2 | 0 | 0 |
Results
One way ANOVA test was used to compare the means of the group (p=0.817, df - 9). [Table/Fig-4].
One way analysis of variance.
Post–Hoc Tukey test was used to find interrelationship between different groups. [Table/Fig-5].
Post Hoc tests – multiple comparisons.
| (I) GROUP | (J) GROUP | Mean Difference (I-J) | Std. Error | p Value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| A | B | 0.500 | 0.473 | 0.717 | -0.77 | 1.77 |
| A | C | 0.100 | 0.473 | 0.997 | -1.17 | 1.37 |
| A | D | 0.200 | 0.473 | 0.974 | -1.07 | 1.47 |
| B | C | -0.400 | 0.473 | 0.832 | -1.67 | 0.87 |
| B | D | -0.300 | 0.473 | 0.920 | -1.57 | 0.97 |
| C | D | 0.100 | 0.473 | 0.997 | -1.17 | 1.37 |
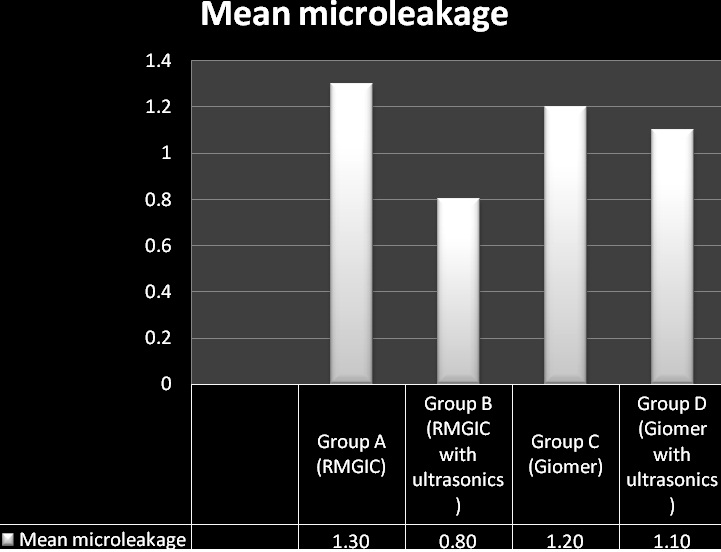
Amongst all, the group B (Resin Modified Glass Ionomer Cement) exhibited least microleakage and group A (Resin Modified Glass Ionomer Cement with ultrasonic activation) demonstrated maximum microleakage with statistically insignificant difference between all the groups. Group C (Giomer) and group D (Giomer with ultrasonic activation) performed better than group A, but were statistically insignificant. Group B performed better than group C and group D which was again statistically insignificant. Group D showed better results as compared to group C but was statistically insignificant.
Discussion
In the present research, group B (RMGIC with ultrasonic activation) depicted the best results, RMGIC owing to its adhesive properties like GIC and good wear resistance like composite along with ultrasonic activation may be the reason for the better performance and hence was selected as control group for the study. In Group B (RMGIC with ultrasonic) and Group D (Giomer with ultrasonic) ultrasonic activation, accelerated curing process increased powder surface area due to breaking down of glass particles by ultrasonic energy causes increased reactivity and improves physical properties. Previous experiments by Gorseta K, et al., reveals that ultrasonic energy has been successfully used for accelerating the curing process with GIC which was in accordance to the results of this study which reveals that the ultrasonic groups revealed less microleakage [13]. Group C (Giomer) performed better than group A (RMGIC) – low modulus of elasticity and increased flexibility of flowable resin may be helpful in distribution of stresses of polymerisation shrinkage and preserve integrity of bond to tooth structure. Results of this study correlate to the previous research by Payne et al., which demonstrated better marginal sealing ability with flowable composite resin [14]. In giomer glass particles are already pre-reacted and incorporated in the restorative, whereas in RMGIC glass particles are not pre-reacted and hence when ultrasonically activated glass particles are broken down increasing the surface area, providing significant improvement as compared to inactivated group. 0.5% Chloramine T was used because it has no adverse effect on organic phase (collagen) of dentin [15].
Class II cavities were selected for the study because branching of tubules is numerous in the root dentin area and acid etching of this heterogeneous dentin surface is quite difficult. In cases of deep cavities with cervical margin in cementum, bonding itself to cementum is poor; also the formation of hybrid layer is difficult in this critical zone [16]. Beautifil Flow Plus (Giomer) was used as a base because it combines delivery of flowable and strength of hybrid composites, Beautifil II (Giomer) was used for coronal restoration owing to its unique properties like flouride recharge/release, wear resistance, chameleon effect making it an ideal material for coronal restoration.
Thermo cycling (5°c and 55 °c, dwell time – 15 seconds) was done to mimic the temperature extremes found in oral cavity. Methylene blue dye was used as it exhibits better penetration results [17]. Molecular weight of methylene blue dye is lower than bacterial toxins (1.2 mm2) thus exhibiting better results as compared to eosin or other radioisotope tracers [18]. Dye penetration method was used to check microleakage because it demonstrate sections showing leakage in contrasting colours without the need for further chemical reaction or exposure to potentially hazardous chemicals. It has good sensitivity, convenience and ease of use [19].
Stereomicroscope was used for evaluation of prepared samples as it provides well magnified two dimensional view showing areas of microleakage.
Clinical implications: Ultrasonic activation of various recently introduced hybrid ionomers like giomers may provide better adaptation of lining material while restoring subgingival class II defects, thus resulting in long term restorative treatment success.
Limitation
The present laboratory research needs to be further validated by clinical researches before deriving the final conclusion. The present experiment incorporated 500 cycles of thermocycling to mimic the clinical scenario. However, 10,000 cycles of thermo cycling corresponds to one year of clinical performance whereas 500 cycles used in the present research approximately will correspond to 15 days of clinical performance, which again is a very small period to simulate the clinical situation [20]. From research perspective, it would be desirable to develop an accelerated aging model to challenge the durability of resin dentin bonds in a relatively short period of time. Some approaches that should be taken into consideration include masticatory stresses, pH cycling, temperature cycling, wet environment and various aging conditions [21]. This study partially incorporated the above mentioned parameters, however; strict adherence to aforesaid would have better mimicked the clinical environment.
Conclusion
Ultrasonic activation of the lining material seems to be good alternative to reduce microleakage. Also, recently introduced hybrid ionomers with good anti-cariogenic effect alike giomer may prove to be an effective alternative for the long term success of the highly technique sensitive class II composite restorations.
[1]. Klaff D J, Blending incremental and stratified layering techniques to produce an esthetic posterior composite resin restoration with a predictable prognosisJ Esthet Restor Dent 2001 13:101-13. [Google Scholar]
[2]. Dennison JB, Yaman P, Seir R, Hamilton JC, Effect of variable light intensity on composite shrinkageJ Prosthet Dent 2000 84:499-505. [Google Scholar]
[3]. Ausiello P, Davidson CL, Cascone P, DeGee AJ, Rengo S, Debonding of adhesively restored deep class II MOD restorations after functional loadingAm J Dent 1999 12:84-88. [Google Scholar]
[4]. Suzuki M, Jordan RE, Glass ionomer-composite sandwich techniqueJ Am Dent Assoc 1990 120:55-57. [Google Scholar]
[5]. Fabianelli A, Microleakage in class II restorations: open vs closed centripetal build-up techniqueOper Dent 2010 35:308-13. [Google Scholar]
[6]. Arora V, Nikhil V, Sawani S, Arora P, The open sandwich technique with glass ionomer cement – a critical evaluationInternational Journal of Innovative Research in Science, Engineering and Technology 2013 2:3874-82. [Google Scholar]
[7]. Uno S, Finger WJ, Fritz U, Long-term mechanical characteristics of resin-modified glass ionomer restorative materialsDent Mater 1996 12:64-69. [Google Scholar]
[8]. Irie M, Suzuki K, Marginal gap formation of light-activated base/liner materials: effect of setting shrinkage and bond strengthDent Mater 1999 15:403-07. [Google Scholar]
[9]. Ikemura K, Tay FR, Endo T, Pashley DH, A review of chemical-approach and ultramorphological studies on the development of fluoride-releasing dental adhesives comprising new pre-reacted glass ionomer (PRG) fillersDent Mater J 2008 27:315-39. [Google Scholar]
[10]. Gordan VV, Mondragon E, Watson RE, Garvan C, Mjör IA, A clinical evaluation of a self-etching primer and a giomer restorative material: results at eight yearsJ Am Dent Assoc 2007 138:621-27. [Google Scholar]
[11]. Tech profiles: Beautifil Flow PlusInside Dentistry201(7):108 [Google Scholar]
[12]. Griffin JD, Unique characteristics of the giomer restorative systemInside Dentistry 2014 10:84-87. [Google Scholar]
[13]. Gorseta K, Glavina D, Skrinjaric I, Influence of ultrasonic excitation and heat application on the microleakage of glass ionomer cementsAust Dent J 2012 57:53-57. [Google Scholar]
[14]. Payne JH, The marginal seal of class II restorations: flowable composite resin compared to injectable glass ionomerJ. Clin Pediatr Dent 1999 23:123-30. [Google Scholar]
[15]. DeWald JP, The use of extracted teeth for in vitro bonding studies: a review of infection control considerationsDent Mater 1997 13:74-81. [Google Scholar]
[16]. Bala O, Octasli MB, Onlu I, The leakage of class II cavities restored with packable resin based compositesJ Contemp Dent Pract 2003 4:01-11. [Google Scholar]
[17]. Rossomando KJ, Wendt SL Jr, Thermocycling and dwell times in microleakage evaluation for bonded restorationsDent Mater 1995 11:47-51. [Google Scholar]
[18]. Taylor MJ, Lynch E, Microleakage, reviewJ Dent 1992 20:03-10. [Google Scholar]
[19]. Camps J, Pashley D, Reliability of the dye penetration studiesJ Endod 2003 29:592-94. [Google Scholar]
[20]. ISO-Standards (1994) ISO TR 11405. Dental materials – guidance on testing of adhesion to tooth structure. In: Anonymous Geneve: International Organization for Standardization. 1st edition:15-25 [Google Scholar]
[21]. Reis A, Martins G, Paula E, Sanchez A, Loguercio A, Alternative aging solutions to accelerate resin-dentin bond degradationAdhes. Dent 2015 17:321-28. [Google Scholar]