Urinary Protein Creatinine Ratio in Normal Zero to Three-Day-Old Indian Neonates
Indu Saxena1, Varun Shivankur2, Manoj Kumar3
1 Assistant Professor, Deparment of Biochemistry, AIIMSJodhpur, Rajasthan, India.
2 Under Graduate Student, AIIMSJodhpur, Rajasthan, India.
3 Professor, Department of Physiology, TMMC&RC, Moradabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Indu Saxena, Assistant Professor, Deparment of Biochemistry, AIIMS Jodhpur-342005, Rajasthan, India.
E-mail: indu.saxena@rediffmail.com
Introduction
Early neonates (1-7-day-old) may develop acute kidney injury or acute renal failure due to functional (pre-renal, may be caused by decreased renal perfusion), intrinsic (renal, may be caused by acute insult), or obstructive (due to anatomic urinary tract obstruction) causes. Urinary protein estimation is important for diagnosis, follow-up and prognosis of disease. The Protein Creatinine Ratio (PCR) has been successfully used to establish proteinuria in different types of patients.
Aim
This study was undertaken to establish normal PCR range in neonates, to rule out abnormal protein excretion in sick neonates.
Materials and Methods
A total of 37 normal early neonates of age 0-3 days were enrolled for this study. Random spot urine samples were collected in paediatric urine bags for protein and creatinine estimation.
Results
The urinary PCR varied between 0.1-0.8. The range of PCR values obtained was greater in 0-1 day old infants, compared to infants older than one day. Changes in PCR values were due to variations in the creatinine excretion.
Conclusion
Urinary PCR values ≤ 0.8 indicate normal protein excretion. However, reference intervals of PCR should be established for narrow age groups in case of early neonates, e.g. 0-6h, 6-12h, 12-24h, 24-72h old babies.
Newborn, Protein estimation, Proteinuria
Introduction
Renal disorders may develop in the newborns as a result of congenital or acquired conditions. 1-24% patients in the neonatal intensive care unit develop acute renal failure which can be pre-renal, renal, or post-renal in origin [1,2]. The Intensive Care Nursery House Staff Manual of the UCSF Children’s Hospital, University of California [3] reports the detection of renal and urinary tract anomalies in about 1% of fetuses by pre-natal ultrasound, in 1% of newborns by physical examination, and in 7-9% individuals by autopsy. Early diagnosis of abnormalities of renal structure or function can help prevent future complications including hypertension, obstructive uropathy, urinary tract infections and renal failure. Urine analysis is important in establishing renal disease [4]. Since it is difficult to obtain timed urine specimens from neonates, biochemical techniques that can be performed on untimed urine samples are useful in assessing renal function.
Proteinuria and haematuria are indications of renal damage. The amount of protein excreted in 24h urine can not be estimated without catheterization of the new-born. The semi-quantitative dipstick analysis, performed on random spot urine samples, is the most commonly performed investigation for proteinuria However, it is of debatable accuracy and different rates of false positives and false negatives have been reported by different researchers [5,6]. While the false positive results lead to over investigations and interventions, the false negative results compromise the treatment of the neonate. The use of automated dipstick readers in laboratories has reduced observational errors and improved the accuracy of dipstick results [7].
The Protein Creatinine Ratio (PCR) shows a good correlation with subsequent 24h protein estimation in patients suffering from different diseases [8–11]. In children older than one year and adults, the spot urinary Protein Creatinine Ratio (PCR) is often used for the quantitation of proteinuria [12]. The excretion of protein and creatinine in urine has been shown to vary in the different trimesters of pregnancy [13]. The amount of urinary creatinine varies with age, height, muscle mass, sex, and race [14]. Creatinine excretion in urine is reported to be less in Indo-Asians compared to the Caucasians [15].
Aim
This study was conducted on early (0-3 day old) normal Indian neonates. The excretion of protein and creatinine in urine was determined, and the protein creatinine ratio was calculated. The values of PCR were compared in babies of different ages.
Materials and Methods
This observational study was conducted in a three month period (from July- September, 2015), after obtaining Ethical Clearances from the Institutes’ Ethical Committees. Total of 37 early neonates (0-3-day-old) (16 female) were selected for this study after obtaining signed informed consent from their parent or guardian.
Inclusion Criteria
Full term babies of 38-41 week gestational age (calculated from menstrual history and ultrasonography), birth weight 2500-4000 gram, and Apgar score ≥ 7 five minutes after birth were selected for this study.
Exclusion Criteria
Babies in the acute phase of physiologic jaundice and those currently taking any medications were excluded from the study.
Since only 37 babies were recruited in this study, they were not grouped on the basis of gender.
Spot urine samples were collected from the selected neonates by using paediatric urine collection bags. Urine collected in the bag was stored in non-sterile urine pot and taken to the laboratory for analysis. None of the samples contained blood (determined by using urine dipsticks) or faeces (observed visually).
Urinary microprotein was analysed using microprotein estimation kit (from Bio Lab Diagnostics) based on pyrogallol red dye binding method. Urinary creatinine was estimated using estimation kit (from Span Diagnostics) based on modified Jaffe’s method. The Protein Creatinine Ratio (PCR) of each sample was calculated from the equation:

The PCR values obtained from full term, normal early neonates were used to obtain the reference interval. Since the distribution was non-Gaussian, a non- parametric method was used. The 95% range (2.5th–97.5th percentile) was taken as the reference interval.
Results
The protein and creatinine concentrations (mg/dL) in the random spot urine samples obtained from 0-1, 1-2, and 2-3-day-old infants are summarized in [Table/Fig-1]. The mean values of protein concentration do not show much variation in the three age groups, 13.67, 17.68, and 15.25 mg/dL, respectively. The average creatinine concentration was lower in 0-1-day-old infants (25.5 mg/dL) compared to creatinine excretion in infants older than one day.
Protein and creatinine concentrations and PCR values obtained from random spot urine samples obtained from 0-3-day-old neonates.
| Parameter | Age of neonate at the time of sample collection |
|---|
| 0-1 Day | 1-2 Days | 2-3 Days |
|---|
| Urinary Protein (mg/dL) | 13.667 ± 7.89 | 17.684 ± 7.00 | 15.25 ± 7.16 |
| Urinary Creatinine (mg/dL) | 25.5 ± 8.29 | 42.05 ± 14.49 | 44.58 ± 16.47 |
| Protein Creatinine Ratio | 0.542 ± 0.255 | 0.423 ± 0.124 | 0.333 ± 0.086 |
Since there were only 6 infants aged 0-1 day, while there were nineteen 1-2-day-old babies and twelve 2-3-day-old babies, the results were not compared by ANOVA. Maximum variation in PCR was observed in 0-1 day old infants (0.11-0.82), compared to 1-2-day-old (0.29-0.78) and 2-3-day-old (0.17-0.33) infants.
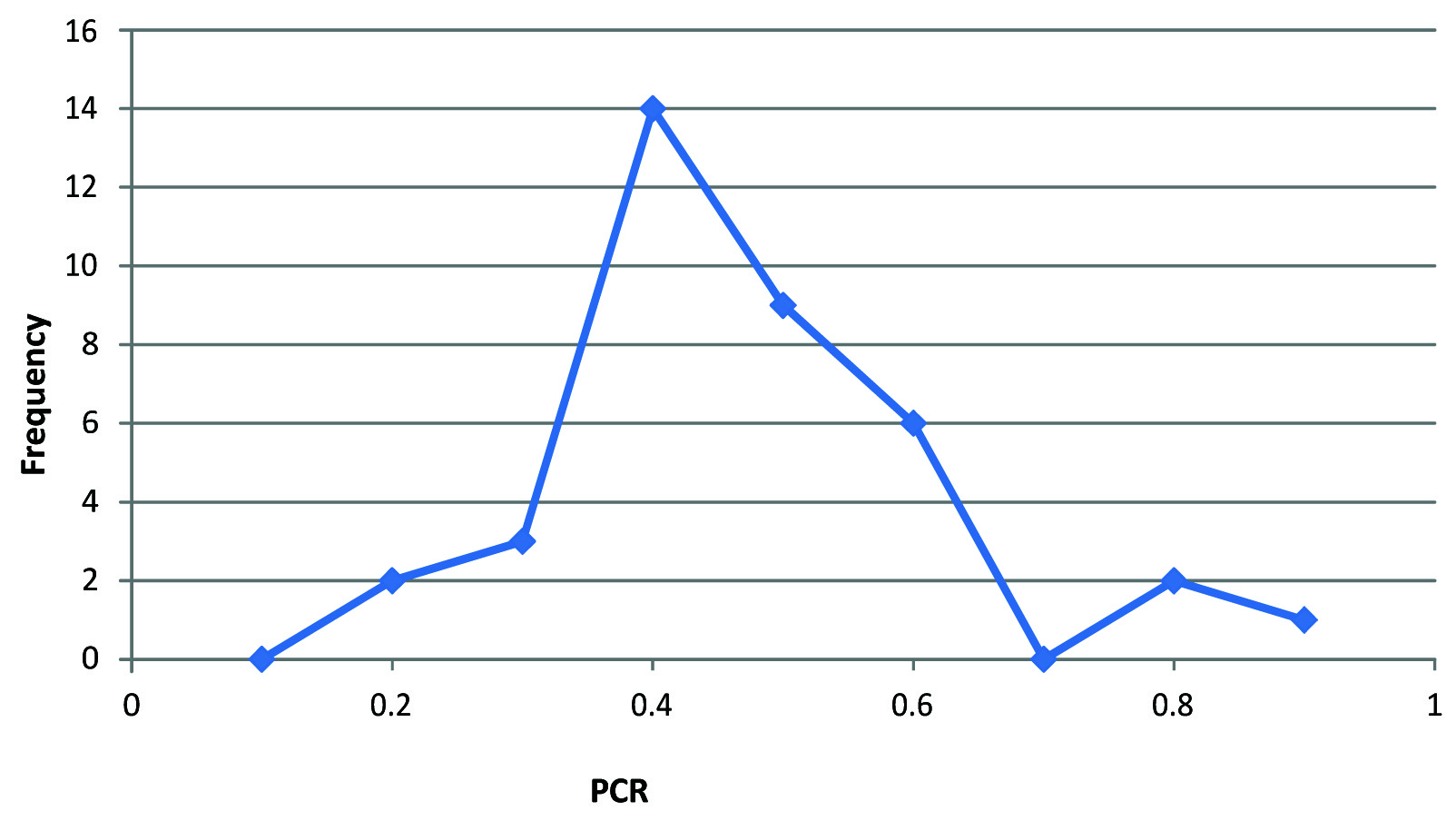
The frequency curve [Table/Fig-2] for urinary protein creatinine ratio showed a median range of 0.4-0.6. The modal range (with maximum number of observations) was 0.3-0.4. Since the distribution of PCR values was non- Gaussian, the normal range of urinary PCR was determined by the non- parametric method (2.5th - 97.5th percentile) and was found to be 0.1-0.8.
Frequency distribution curve for urinary protein creatinine ratio in 0-3-day-old neonates
Discussion
The protein concentration varied from 6-32 mg/dL in 0-3-day-old neonates. When the protein excretion was compared in infants of different ages (0-1 day, 1-2 day, and 2-3 day), the mean values did not show much variation: 13.667mg/dL (Day 0-1), 17.684 mg/dL (Day 1-2), 15.250 mg/dL (Day 2-3). Variation in protein excretion was less compared to that noted for creatinine [Table/Fig-1]. Creatinine is produced from creatine, which is almost exclusively located in the skeletal muscle. About 2% of the muscle creatine is converted into creatinine everyday, and is subsequently excreted in the urine [16]. Creatinine excretion varied from 14 to 65 mg/dL in 0-3-day-old neonates. Matos et al., have reported a high and variable creatinine excretion in the first few days of life in human neonates [17]. Although nephrogenesis begins at 5 weeks of gestation and is complete by 36 weeks of gestation, the GFR is very low as the nephrons are small and functionally immature [18]. The GFR increases after 36 weeks of gestation till birth, and shows a dramatic increase after birth due to increase in cardiac output and systemic blood pressure and decrease in renal vascular resistance leading to increased renal blood flow and effective glomerular filtration pressure. There is also an alteration in the pattern of renal blood flow distribution, an increase in the permeability of the glomerular membrane, and an increase in the surface area available for filtration [19]. Still the GFR in the full term neonate is very low (about 20 mL/min/1.73 m2 increases to about 40 mL/min/1.73 m2 at one month) [18], still less than the normal adult values (55-140 mL/min/1.73m2) [20]. The rapidly increasing values of GFR explain the high variation in creatinine excretion in early neonates.
Newborn babies have elevated plasma creatinine levels that are close to the maternal plasma creatinine values and do not reflect the size and muscle mass of the new born [21,22]. Since creatinine is a small molecule (molecular weight 113 dalton, radius 0.3 nm), it is able to pass through the placenta. Equilibration of maternal and fetal plasma creatinine levels occurs during the second half of gestation [23]. After birth, plasma levels of creatinine continue to remain high for about a week. This is due to the tubular reabsorption of creatinine, a result of back flow of creatinine across the leaky tubular and vascular structures. Once renal maturity is attained, creatinine excretion in urine increases and plasma creatinine levels fall to values normal for the age. Since the normal urine output in an early neonate is about ≥1mL/kg/h [3], creatinine excretion is slow and occurs over a period of about 7 days.
On comparing the creatinine excretion in infants of different age groups, the concentration of creatinine was less in 0-1-day-old infants (14-38 mg/dL, mean mg/dL). Concentration increased after the first day and was similar in 1-2 and 2-3-day-old infants [Table/Fig-1].
A comparison of the PCR values on days 0-1, 1-2, and 2-3 shows that PCR values showed a decreasing trend with the age of the infant [Table/Fig-1]. Also, maximum variation in the PCR values was observed on Day 0-1.
While the PCR values less than 0.2 are considered normal in children above 2 years of age and in adults, values up to 0.5 may be considered normal in 6-24 month old children [24]. This study suggests that random spot urinary PCR values of up to 0.8 may be considered normal in 0-3-day-old infants.
Limitations
The size of study sample was small. Values of protein creatinine ratio obtained in one, two, and three-day-old infants could not be compared by ANOVA since there were only 6 infants in the 0-1-day-old category.
A larger study with more subjects needs to be conducted to study the variation in protein creatinine ratio in 1-7 day old full term and pre-term neonates. Reference intervals of PCR should be determined for narrow range of age groups in case of early neonates, e.g. 0-6h, 6-12h, 12-24h, 24-72h old babies.
Conclusion
Protein concentration in random spot urine sample from 0-3-day-old neonates varied from 3-32 mg/dL, while creatinine concentration varied from 14-65 mg/dL. Creatinine concentration was lower in 0-1-day-old infants. Protein creatinine ratio of the random spot urinary samples varied from 0.11 to 0.82. The ratio showed a greater variation in the 0-1-day-old infants. A PCR value of ≤ 0.8 may be considered normal for 0-3-day-old infants. Reference interval of PCR needs to be calculated for infants of different ages, e.g. 0-6 hour, 6-12 hour, 12-24 hour, 24-72 hour olds, since the values show a large variation due to rapidly changing glomerular filtration rate.
[1]. Suhas M, Nafday SM, Renal DiseaseIn Avery’s Neonatology Pathophysiology and Management of Newborn 2005 6th EditionLippincottWilliams and Wilkins:981-1065.Editor: MacDonald MG [Google Scholar]
[2]. Gouyon JB, Guignard JP, Management of acute renal failure in newbornsPaediatr Nephrol 2000 14:1037-44. [Google Scholar]
[3]. Intensive Care Nursery House Staff Manual, 2004; UCSF Children’s Hospital, UCSF Medical Center, University of California. Pp. 178-180 [Google Scholar]
[4]. Libório AB, Branco KMPC, deMelo Bezerra CT, Acute Kidney Injury in Neonates: From Urine Output to New BiomarkersBioMed Research International 2014 2014:601568 [Google Scholar]
[5]. Kuo VS, Koumanantakis G, Gallery EDM, Proteinuria and its assessment in normal and hypertensive pregnancyAm J Obstet Gynaecol 1992 167:723-28. [Google Scholar]
[6]. Meyer NL, Mercer BM, Friedman SA, Sibai BM, Urinary dipstick protein: a poor predictor of absent or severe proteinuriaAm J Obstet 1994 170:137-34. [Google Scholar]
[7]. Bell SC, Armstrong CA, Shennan AH, Boyce T, Halligan AWF, Reliable urine analysis in the management of hypertensive pregnanciesEur J Obstet Gynaecol Reprod Biol 2000 93:181-83. [Google Scholar]
[8]. Ginsberg JM, Chang BS, Matarese RA, Garella S, Use of single voided urine samples to estimate quantitative proteinuriaN Eng J Med 1983 309:1543-46. [Google Scholar]
[9]. Steinhauslin F, Wauters JP, Quantitation of proteinuria in kidney transplant patients: accuracy of the protein/ creatinine ratioClin Nephrol 1995 43:110-15. [Google Scholar]
[10]. Brodby RA, Rohde RD, Zeev S, Pohl MA, Bain RP, Lewis EJ, The urine protein to creatinine ratio as a predictor of 24 hour urine protein excretion in Type 1 diabetic patients with nephrologyAm J Kid Dis 1995 26:904-09. [Google Scholar]
[11]. Quadri KHM, Bernardini J, Greenberg A, Laifer S, Syed A, Holley JL, Assessment of renal function during pregnancy using a random protein to creatinine ratio and Cockcroft Gault formulaAm J Kid Dis 1994 24:416-20. [Google Scholar]
[12]. Price CP, Newall RG, Boyd JC, Use of protein: creatinine ratio measurements on random urine samples for prediction of significant proteinuria: A systematic reviewClinical Chemistry 2005 51(9):1577-86. [Google Scholar]
[13]. Saxena I, Kapoor S, Gupta RC, Detection of Proteinuria in Pregnancy: Comparison of Qualitative Tests for Proteins and Dipsticks with Urinary Protein Creatinine IndexJ Clin Diag Res 2013 7(9):1846-48. [Google Scholar]
[14]. Remer T, Neubert A, Maser-Gluth C, Anthropometry-based reference values for 24-h urinary creatinine excretion during growth and their use in endocrine and nutritional research 1Am J Clin Nutr 2002 75:561-69. [Google Scholar]
[15]. Jafar TH, Schmid CH, Levey AS, Serum creatinine as marker of kidney function in South-Asians: A study of reduced GFR in adults in PakistanJ Am Soc Nephrol 2005 16:1413-19. [Google Scholar]
[16]. Borsook H, Dubnoff JW, The hydrolysis of phosphocreatine and the origin of urinary creatinineJ Biol Chem 1947 168:493-510. [Google Scholar]
[17]. Matos V, Drukker A, Guignard JP, Spot urine samples for evaluating solute excretion in the first week of lifeArch Dis Child Fetal Neonatal Ed 1999 80:F240-42. [Google Scholar]
[18]. Bitsori M, The development of renal functionIn Essentials in Paediatric Urology 2012 Kerala, India:9-20.Editor: Sakellaris G. Research Signpost [Google Scholar]
[19]. Su SW, Stonestreet BS, Core Concepts: Neonatal Glomerular filtration rateNeo Reviews 2010 11(12):e714-21.DOI: 10.1542/neo.11-12- e714 [Google Scholar]
[20]. Wetzels JFM, Kiemeney LALM, Swinkels DW, Willems HL, den Heijer M, Age- and gender-specific reference values of estimated GFR in Caucasians: The Nijmegen Biomedical StudyKidney Int 2007 72:632-37. [Google Scholar]
[21]. Bueva A, Guignard JP, Renal function in pre-term neonatesPaediatr Res 1994 36:572-77. [Google Scholar]
[22]. Guignard JP, Renal function in the newborn infantPaediatr Clin North Am 1982 29:777-90. [Google Scholar]
[23]. Guignard JP, Drukker A, Why Do Newborn Infants Have a High Plasma Creatinine?Paediatrics 1999 103(4):e49 [Google Scholar]
[24]. Houser M, Assessment of proteinuria using random urine samplesJ Paediatr 1984 104:845-48. [Google Scholar]