Familial Hepatocellular Carcinoma- First Reported Case from India
Smita Chandra1, Anuradha Kusum2, Harish Chandra3, Kanika Yadav4, Sanjiv Kumar Verma5
1 Associate Professor, Department of Pathology, Himalayan Institute of Medical Sciences, SRHU, Swami Ram Nagar, Doiwala, Dehradun, Uttarakhand, India.
2 Professor, Department of Pathology, Himalayan Institute of Medical Sciences, SRHU, Swami Ram Nagar, Doiwala, Dehradun, Uttarakhand, India.
3 Professor, Department of Pathology, Himalayan Institute of Medical Sciences, SRHU, Swami Ram Nagar, Doiwala, Dehradun, Uttarakhand, India.
4 Resident, Department of Pathology, Himalayan Institute of Medical Sciences, SRHU, Swami Ram Nagar, Doiwala, Dehradun, Uttarakhand, India.
5 Professor, Department of Medicine, Himalayan Institute of Medical Sciences, SRHU, Swami Ram Nagar, Doiwala, Dehradun, Uttarakhand, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Smita Chandra, Associate Professor, Department of Pathology, Himalayan Institute of Medical Sciences, Swami Ram Nagar, Doiwala, Dehradun-248140, Uttarakhand, India. E-mail : smita_harish@yahoo.com
Familial clustering of Hepatocellular Carcinoma (HCC) is commonly observed in various parts of the world including China and Eastern Asia where HBV is endemic while in western world, genetic factors and metabolic disorders may play an important role. In India, HCC is considered to be a rare tumour and till date no case of familial HCC has been reported here. Therefore the present case demonstrates rare occurrence of familial HCC which is being reported for the first time from India on cytology. The case also highlights an unusual feature that it was not associated with any risk factor including HBV, HCV infection, alcoholism, obesity, diabetes or smoking suggesting its independent association with genetic factors. Cytology is uncomplicated diagnostic tool for HCC and may be useful for its early diagnosis. This case also highlights the importance of early surveillance and follow up of blood relatives for every case of HCC so that early diagnosis and management of familial HCC is possible.
Cytology, Risk factors, liver malignancy
Case Report
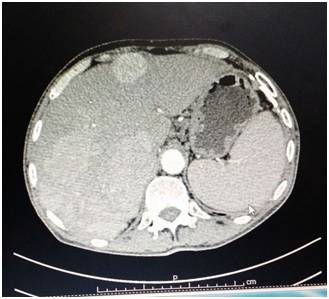
Two brothers aged 45 and 38 years, laborers by profession, thin built and natives of non-endemic north Himalayan state of India presented to the hospital with chief complaints of loss of appetite, history of loose stools and with weakness for last one year and along with mild pain in right upper quadrant of abdomen. Both the brothers were non vegetarian by diet and were strict non alcoholic and non smokers. There was no family history of diabetes and hypertension. Clinical examination revealed mild pallor but icterus was absent in both the brothers. Per-abdomen examination revealed mild hepatomegaly in both the brothers. There was no past history of jaundice or blood transfusion. Family history revealed an important feature of death of mother about 20 years back with similar complaints when she was 48-year-old. However, no clinical, laboratory or diagnostic details were available regarding her illness. The relevant laboratory investigations of one brother showed mild anaemia (10.5 g/dl), normocytic normochromic type with serum total bilirubin of 1.8 mg/dl (Indirect- 0.8 g/dl, Direct-1.0mg/dl), AST of 60 IU/l, ALT of 58 IU/l, total protein of 5.2 g/dl and serum albumin of 3.8 g/dl and random blood sugar level of 100 mg/dl. The laboratory investigations of another brother revealed haemoglobin of 10 gm/dl, normocytic normochromic anaemia, with total bilirubin of 2.1 mg/dl (Indirect- 1.1, Direct- 1.0 mg/dl), AST of 74 IU/l, ALT of 51 IU/l, total protein 6.1 g/dl and serum albumin of 4.1g/dl and globulin of 2.0 g/dl random blood sugar level of 98 mg/dl. Both the patients were non reactive for hepatitis B or C virus. Ultrasonography (USG) of whole abdomen in both brothers revealed hepatomegaly with multiple echogenic masses of varying sizes in both the lobes of the liver and possibility of secondary in liver was suggested. CECT abdomen revealed multiple heterogeneously enhancing space occupying lesion in liver [Table/Fig-1]. USG guided Fine Needle Aspiration Cytology (FNAC) from liver lesion was advised and cytological examination in both the brothers revealed Tumour sheets and fragments with sinusoidal pattern and transgressing capillaries with Tumour cells showing prominent macro nucleoli and intranuclear inclusions [Table/Fig-2,3]. Occasional Tumour cells showed presence of bile in them and mitosis was frequent. There was evidence of mild to moderate steatosis in the smears examined in both the cases [Table/Fig-2,3]. Cytological diagnosis of HCC was given in both the patients and serum alpha-fetoprotein levels were advised. However, due to reluctance of both brothers and financial constraints any further investigations, surgery, therapy and genetic studies were not carried out and both the brothers succumbed to their illness within period of 3 months.
Discussion
HCC is one of the most commonly diagnosed cancer in the world with the incidence of 5.6% of total cancer cases [1]. The prognosis for liver cancer is very poor with mortality to incidence ratio of 0.9:1 [1]. However, the prevalence of liver cancer in India is rare and estimated five year prevalence is 0.7% with mortality of 3.9% and maximum number of cases presenting in age group of above 75 years (21.9 per 1, 00,000 of cases) [1]. Persistent infections by Hepatitis B (HBV) or Hepatitis C (HCV) along with aflatoxin exposure are important risk factors for hepatocellular carcinoma (HCC) and recently heavy alcohol drinking, tobacco smoking, overweight, diabetes, familial/genetic factors and dietary factors are also considered to play an important role in its pathogenesis [2]. Familial clustering of HCC has been reported from some parts of the world including east Asia where HBV infection has proved to be an important associated risk factor while in western world, family history independently plays an important role [3–5]. However, literature search and to the best of our knowledge no case of familial HCC has still been reported from India. The present case of familial HCC which is being reported is unusual as both the siblings did not show any evidence of HBV or HCV infection or any other risk factor including alcoholism, smoking, obesity or diabetes. However, death of their mother around the same age and under similar circumstances suggests an inheritable genetic cause for the development of familial HCC. Apart from China and other East Asian countries where HCC is common and HBV infection is considered to be important risk factor for familial HCC, studies from western world have concluded that family history of HCC increases the risk of familial HCC independently of hepatitis [5,6]. They also concluded that combination of family history of liver cancer and hepatitis B/C serum markers is associated with an over 70-fold elevated HCC risk [5].
CECT abdomen revealed multiple heterogeneously enhancing space occupying lesion in liver.
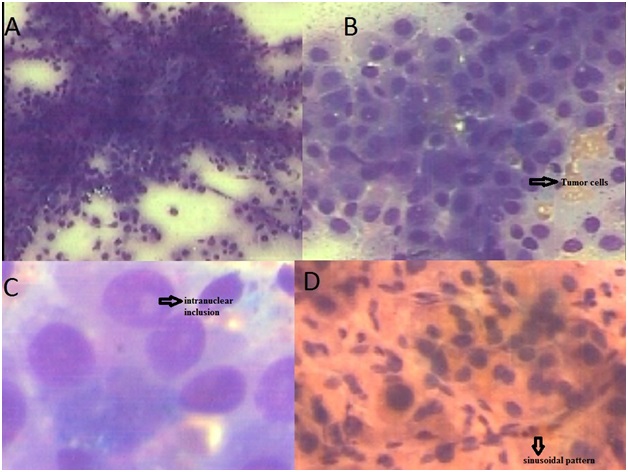
FNAC of liver in one brother showed: a) Tumour fragments and singly lying malignant cells in hepatocellular carcinoma (Giemsa; x40); b) Malignant round to polygonal liver cells showing overcrowding with well defined cytoplasm and nuclei with coarse chromatin, prominent nucleoli (Giemsa; x100); c) Malignant cells showing intranuclear inclusions (Giemsa; x400); d) Characteristic sinusoidal pattern observed in HCC (Haematoxyline- eosin; x40).
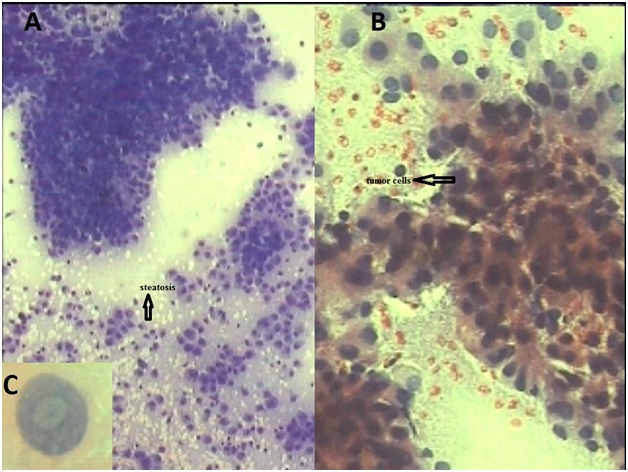
FNAC of liver in another brother showed: a) Sheets and singly lying Tumour cells with evidence of steatosis (Giemsa; x40); b) Tumour cells at higher magnification (Papanicolaou stain; x100); c) Nuclei showing intranuclear inclusion in HCC (Papanicolaou stain; x400).
The present case also showed evidence of familial HCC independent of hepatitis infection and suggests association with genetic factors. The overexpression of apolipoprotein family (ApoA1, ApoA2, ApoC3, ApoE) and serum amyloid A protein in comparative proteomic profiles of HCC cases family members indicate that genetic factors may account for familial aggregation of HCC [7]. However, as no genetic profiling was done in both the brothers so comments cannot be made on proteomic profiles in this case. Another interesting feature observed was that both the brothers were of much younger age group and succumbed to their illness within three months of diagnosis. Familial HCC is considered to be malignancy of elderly age group and maximum number of cases in India occur in age group of above 75 years with high mortality [1]. Liu Li et al., have concluded in their study that familial HCC has earlier age of onset with relatives having higher risk of HCC in early age group [3]. Other studies have also observed that a positive family history may be associated with earlier appearance of HCC even if associated with HBV infection recommending intense surveillance of family members of HCC patients [8].
Cytology is considered to be important tool for diagnosis of HCC with minimum complications and sensitivity ranging from 67 to 93% and specificity of 96 to 100% [9]. The observation of steatohepatitic morphology in HCC is commonly seen in non alcoholic fatty liver disease and suggests significant association with metabolic risk factors [10]. The vigilant examination of cytological smears in both the cases also showed evidence of mild to moderate steatosis which may indicate association with metabolic risk factors. However, as complete clinical follow up and investigations were not possible due to patients’ reluctance so definite opinion is not possible regarding it.
Conclusion
The present case of familial HCC is being reported for the first time from India and with an unusual feature that it was not associatedwith any risk factor including HBV, HCV infection, alcoholism, obesity, diabetes or smoking suggesting an independent association with genetic factors. Cytology is uncomplicated diagnostic tool for HCC and may be useful for its early diagnosis. In addition, this case highlights the importance of early surveillance and follow up of blood relatives forevery case of HCC so that early diagnosis and management of familial HCC is possible.
[1]. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, GLOBOCAN 2012 V1.0 Cancer Incidence and mortality worldwide : IARC CancerBase no. 11 (Internet) 2013 Lyon, FranceInternational Agency for Research on CancerAvailable from: http://globocan.iarc.fr, accessed on 13/2/2015 [Google Scholar]
[2]. Bosetti C, Turati F, La Vecchia C, Hepatocellular carcinoma epidemiologyBest Pract Res Clin Gastroenterol 2014 28:753-70. [Google Scholar]
[3]. Liu L, Li L, Zhou S, Jiang Q, Chen S, Gao Y, Familial correlations of onset age of Hepatocellular Carcinoma: a population-based case-control family studyPLosOne 2014 9:e108391 [Google Scholar]
[4]. Gao Y, Jiang Q, Zhou X, Ding B, Wang R, Zhao G, HBV infection and familial aggregation of liver cancer: an analysis of case- control family studyCancer Causes Control 2004 15:845-50. [Google Scholar]
[5]. Turati F, Edefonti V, Talamini R, Ferraroni M, Malvezzi M, Bravi F, Family history of liver cancer and hepatocellular carcinomaHepatology 2012 55:1416-25. [Google Scholar]
[6]. Hassan MM, Spitz MR, Thomas MB, Curley SA, Patt YZ, Vauthey JN, The association of family history of liver cancer with hepatocellular carcinoma: a case-control study in the United StatesJ Hepatol 2009 50:334-41. [Google Scholar]
[7]. Zhong DN, Ning QY, Wu JZ, Zang N, Wu JL, Hu DF, Comparative proteomic profiles indicating genetic factors may involve in hepatocellular carcinoma familial aggregationCancer Sci 2012 103:1833-38. [Google Scholar]
[8]. Park CH, Jeong SH, Yim HW, Kim JD, Bae SH, Choi JY, Family history influences the early onset of hepatocellular carcinomaWorld J Gastroenterol 2012 18:2661-67. [Google Scholar]
[9]. Mrzljak A, Kardum-Skelin I, Cvrlje VC, Filipec-Kanizaj T, Sustercić D, Skegro D, Role of fine needle aspiration cytology in management of hepatocellular carcinoma: a single centre experienceColl Antropol 2010 34:381-85. [Google Scholar]
[10]. Jain D, Nayak NC, Kumaran V, Saigal S, Steato hepatitic hepatocellular carcinoma, a morphologic indicator of associated metabolic risk factors: a study from IndiaArch Pathol Lab Med 2013 137:961-66. [Google Scholar]