A Rare Case of Type IV Dual Left Anterior Descending Coronary Artery
Onur Baydar1, Veysel Oktay2, Ugur Coskun3, Ahmet Yildiz4, Tevfik Gurmen5
1 Cardiologist, Department of Cardiology, Istanbul University Institute of Cardiology, Turkey.
2 Cardiologist, Department of Cardiology, Istanbul University Institute of Cardiology, Turkey.
3 Cardiologist, Department of Cardiology, Istanbul University Institute of Cardiology, Turkey.
4 Cardiologist, Department of Cardiology, Istanbul University Institute of Cardiology, Turkey.
5 Professor, Department of Cardiology, Istanbul University Institute of Cardiology, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Onur Baydar, Cardiologist, Department of Cardiology, Istanbul University Institute of Cardiology, Haseki, Aksaray 34350, Istanbul, Turkey.
E-mail: dr.onurbaydar@hotmail.com
Coronary artery anomalies are usually asymptomatic and associated with other cardiac malformations. Dual left anterior descending coronary artery (LAD) is an uncommon congenital anomaly with four subtypes. This anomaly has been described in the angiographic literature and dual LAD types depending on the origin of major septal and diagonal branches and course within the anterior interventricular sulcus. Type IV expresses the anomaly of a rudimentary LAD artery ending in the mid-portion of the anterior interventricular sulcus, and the presence of other LAD originating from the right coronary artery and continuing to the anterior interventricular sulcus. We report the rare case of a patient with the type IV dual left anterior descending coronary artery.
Coronary angiography, Coronary vessel anomalies
Case Report
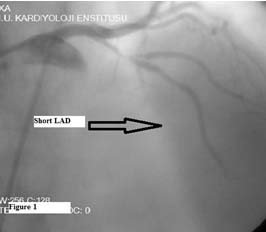
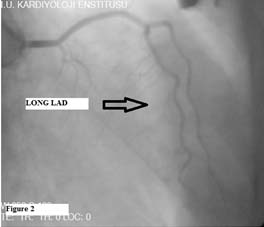
A 78-year-old man with a ten-year history of hypertension was admitted to our hospital because of 3 hours chest pain at rest. The physical examination was normal. His arterial blood pressure was 149/80 mm hg. On surface ECG the rhythm was in sinus rhythm and anterior ischemic ST changes were present. On transthoracic echocardiography; anteroseptal mid, anterior mid apical walls were hypokinetic and EF: 42%. Cardiac biomarkers were detected high and there was no abnormality in other standard biochemical tests. With these results patient was diagnosed Non ST elevation myocardial infarction. Low molecular weight heparin, acetylsalicylic acid and clopidogrel therapy was started immediately. Coronary angiography revealed a coronary artery anomaly of type IV dual LAD with a short LAD, which originated from the LMCA and terminated in the mid-portion of the AIVS. The long LAD originated from the right sinus valsalva, entered into the distal part of the AIVS and travelled towards the apex of the heart, also LAD mid % 90 and D1 proximal % 95 stenosis were detected [Table/Fig-1&2]. Percutaneus coronary intervention was performed to mid segment of the LAD the patient was discharged 5 days after coronary stenting in good health status without any cardiac adverse event. Currently, patient is on follow up, without any problems.
The short LAD originating from the LMCA terminated in the middle part of the AIVS. LMCA: left main coronary artery.
The long LAD originating from the right sinus valsalva and entered the distal part of the AIVS.
Discussion
Coronary artery anomalies are seen in angiographic series about 0.3-0.8% [1]. Most coronary artery anomalies are a result of coincidence during angiography [2,3]. Dual LAD anomaly is usually described by a short LAD that ends high in the anterior interventricula groove and a long LAD that has a proximal course outside the anterior interventricular groove and returns to the groove in its distal course. Four subtypes have been described. In types l and ll, along LAD originates as a branch from the LAD proper, takes a course parallel to the short LAD in its proximal course on either the left ventricle (type l) or the right ventricle (type ll), and re-enters the anterior interventricular groove. Rather than having a parallel diagonal branch, along LAD reenters the anterior interventricular groove in the distal aspect. Type llI dual LAD is extremely rare, occurring in only one of the 23 cases of dual LAD in the angiographic series described by Spindola-Franco et al., Type III dual LAD is characterized by a proximal intramyocardial course of the long LAD. Type IV dual LAD is a very rare type in which the long LAD arises from the right coronary artery, takes an anomalous course, and inserts the anterior interventricular groove [4,5].
Coronary artery anomalies are usually not detectable symptoms. But, when atherosclerotic CAD is present, it is difficult to differentiate major stenosis or occlusion of this anomaly can precipitate CAD has not been established. In patients with suspected acute coronary syndrome superimposed by coronary artery anomalies, a mismatch may occur between the results of noninvasive studies of the involved vessel and those of coronary angiography [6,7].
The course and origin of coronary arteries are very important in these anomalies. Extrinsic compression between the aorta ascendens and pulmonary artery, especially exercise, produce angina, myocardial infarction, syncope or sudden cardiac death in these patients [6–13]. When this happen, surgical treatment is necessary. Coronary artery anomalies are best detected by coronary angiography. MSCT has a role to show relationship between great arteries [14].
Conclusion
The LAD is an important coronary artery and being aware of the congenital anomalies of the LAD helps the physicians make the correct diagnosis and treatment in patients undergoing percutaneous coronary intervention. We treated a patient with type IV dual LAD. Being alert to this coronary artery anomaly will facilitate clinicians to diagnose and manage patients properly.
[1]. Felmeden D, Singh SP, Lip GY, Anomalous coronary arteries of aortic originInt J Clin Pract 2000 54:390-94. [Google Scholar]
[2]. Click RL, Holmes DR, Vlietstra RE, Kosinski AS, Kronmal RA, Anomalous Coronaryarteries: location, degree of atherosclerosis and effect on survival—a Report from the Coronary Artery Surgery StudyJ Am Coll Cardiol 1989 13:531-37. [Google Scholar]
[3]. Patti G, D’Ambrosio A, DiSciascio G, Coronary stenting in patients with situs VisceruminversusG Ital Cardiol 1999 29:304-07. [Google Scholar]
[4]. Spindola-Franco H, Grose R, Solomon N, Dual left anterior descending coronary artery: angiographic description of important variants and surgical implicationsAm Heart J 1983 105:445-55. [Google Scholar]
[5]. Yamanaka O, Hobbs RE, Coronary artery anomalies in 126,595 patients undergoing coronary arteriographyCathet Cardiovasc Diagn 1990 21:28-40. [Google Scholar]
[6]. Trost B, Fernandez-Friera L, Sanz J, Anomalous origin of the three major Coronary arteries from a single common ostiumJ Invasive Cardiol 2010 22:499-501. [Google Scholar]
[7]. Furbatto F, Esposito G, Piccolo R, Franzone A, Capretti G, Piscione F, Chiariello M, Coronary angioplasty with stenting for acute coronary syndrome in Patients with isolated single coronary artery: a report of two casesJ Cardiovasc Med 2009 10:550-53. [Google Scholar]
[8]. Kastanis P, Marti V, Gotsanayidou M, Anomalous left coronary artery arising From the right sinus of Valsalva causing angına pectorisJ Cardiovasc Med 2009 10:574-75. [Google Scholar]
[9]. Taylor AJ, Byers JP, Cheitlin MD, Virmani R, Anomalous right or left coronary Artery from the contralateral coronary sinus: "high-risk" abnormalities in the Initial coronary artery course and heterogeneous clinical outcomesAm Heart J 1997 133:428-35. [Google Scholar]
[10]. Celik M, Iyisoy A, Celik T, A coronary artery anomaly: type IV dual left anterior descending arteryCardiovasc J Afr 2010 21:223-24. [Google Scholar]
[11]. Kunimoto S, Sato Y, Kunimasa T, Double left anterior descending artery arising from the left and right coronary arteries: depiction at multidetector-row computed tomographyInt J Cardiol 2009 132:e54-56. [Google Scholar]
[12]. Voudris V, Salachas A, Saounotsou M, Double left anterior descending artery originating from the left and right coronary artery: a rare coronary artery anomalyCathet Cardiovasc Diagn 1993 30:45-47. [Google Scholar]
[13]. Kosar F, An unusual case of double anterior descending artery originating from the left and right coronary arteriesHeart Vessels 2006 21:385-87. [Google Scholar]
[14]. Girzadas M, Varga P, Dajani K, A single-center experience of detecting Coronary anomalies on 64-slice computed tomographyJ Cardiovasc Med 2009 10:842-47. [Google Scholar]