Fine Needle Aspiration (FNA) is a cost-effective, rapid and safe diagnostic procedure for the initial evaluation of the patient. Aspiration performed under image guidance can provide the desired material from the representative site. In addition to the routine smears, preparation of cell block (CB) can further aid in the cytopathological diagnosis [1]. Large amount of material remains in the needle hub after preparation of smears and this is generally discarded. The material that remains in the needle hub can be used in CB preparation, thus, increasing the sensitivity of diagnosis [2]. The CB provides high cellularity, better architectural patterns, morphological features and an additional yield of malignant cells, and thereby, increasing the sensitivity of the cytodiagnosis when compared with the FNA smears [3]. CB is also useful for categorization of tumour, that otherwise may not be possible from smears [4].
CB also ensures storage and optimal preservation of histochemical and immunocytochemical properties [4].
Thus, FNA and CB together can have a major impact on the patient management and in many cases, avoid diagnostic surgical procedure or expedite the planning for therapy.
Materials and Methods
Our study included all cases of abdominal masses subjected to image-guided FNA during the period from June 2007 to May 2009 in the Cytopathology Department. Cases in which FNA was not under guidance, non-abdominal masses or with inadequate material were not included in the study.
The patients were explained about the simple procedure of FNA and a written consent was taken.
After ruling out bleeding diathesis, FNA was performed and a minimum of 4 smears were prepared for routine stains like Haematoxylin and Eosin (H&E), Papanicolaou stain (PAP), and May-Grunwald Giemsa stain (MGG). The rest of the material present in the needle hub was submitted in CB solution. The CB solution was prepared in accordance with Nathan alcohol formalin substitute but with few modifications. Nathan et al., used 9 parts of 100% ethanol with 1 part of 40% formaldehyde [4]. The CB solutions were prepared by mixing equal quantity of 100% ethanol and 10% formaldehyde. A minimum of 2 hours were given for fixation. Later, the sample was centrifuged at 3,000 rpm for 2-3 min. The supernatant was discarded. 2-3 ml of 10% formalin was added to the pellet and submitted for histopathological processing. As we obtained satisfactory results with this method, the same was applied for the study. In difficult cases and where the patient was willing, IHC was performed on CB sections. These sections were de-paraffinized and subjected to IHC. The sections were treated appropriately with blocking reagents to prevent background staining. IHC markers were selected as per the test requirements and reports.
The cytological smears were categorized as neoplastic and non-neoplastic. The neoplastic lesions were further classified into benign/tumour-like and malignant lesions. The histopathological features of the corresponding CB sections were also studied simultaneously. Additionally, special stains and IHC were done on cell block sections. The FNA diagnoses were then compared with the histopathology of CB sections.
Statistical Analysis
The data was analysed by using Epi info 07 software and Diagnostic accuracy testing was done by sensitivity, specificity, positive predictive value and negative predictive value.
Results
All smears and corresponding CB were studied and a cytopathological diagnosis was made.
The present study included 66 patients with abdominal masses referred for guided FNA cytology. The distribution of abdominal mass is shown in the [Table/Fig-1]. Out of the total 66 patients, 41 were males and 25 were females with a male to female ratio of 1.6:1. The youngest patient was a 10-month-old female child and the oldest patient was 82-year-old. The maximum numbers of patients were in the age group of 5th and 6th decade accounting to 25% each.
Distribution of cases based on site of origin of abdominal mass.
| Site | No of cases | % of cases |
|---|
| Liver | 38 | 57.5% |
| Paraspinous | 06 | 9.09% |
| Retroperitoneum | 06 | 9.09% |
| Renal | 04 | 6.06% |
| Adrenal | 04 | 6.06% |
| Hypogastrium | 02 | 3.03% |
| Ovary | 02 | 3.03% |
| Pancreas | 02 | 3.03% |
| Right Iliac fossa | 01 | 1.51% |
| Left hypochondrium | 01 | 1.51% |
Majority of the patients presented with complaints of pain abdomen (38%) followed by abdomen distension (17%), fever (12%) in decreasing order of frequency.
In our study, maximum number of cases were of liver origin. We had 38 cases of which all the FNA’s showed material while only 27 cases had adequate material on CB. With both FNA and CB, cytopathological diagnosis was given out of which 31 were neoplastic, 3 were tumour-like and 4 were non-neoplastic as shown in the [Table/Fig-2]. Among the 31 neoplastic lesions, 20 were diagnosed as Hepatocellular carcinoma (HCC) and 11 cases were diagnosed as metastatic deposits to the liver.
Distribution of cases of liver lesions.
| Lesions | Type | Total |
|---|
| Malignant Lesions | Hepatocellular Carcinoma | 20 |
| Metastatic Lesions | 11 |
| Tumour like conditions | Diffuse parenchymal liver disease | 1 |
| Large cell dysplasia | 1 |
| Regenerative nodule | 1 |
| Non neoplastic lesions | Hydatid cyst | 2 |
| Non specific abscess | 2 |
| Total | 38 |
In non-neoplastic lesions of the liver, two cases were of hydatid cyst. A 5 ml of straw colour fluid (5 ml) was aspirated with the CB exhibiting hyaline laminated membrane. Three cases were reported as tumour-like lesions which included diffuse parenchymal disease, large cell dysplasia and regenerative nodule. Two cases of liver abscess were reported.
Rest of the cases were from other sites which included paraspinous region, retroperitoneum, kidney, adrenal gland, ovary, pancreas, hypogastrium, left hypochondrium and right iliac fossa.
The details of these cases with cytopathological diagnosis have been mentioned in the [Table/Fig-3].
Distribution of cases of non-liver origin.
| Cytopathological diagnosis | No of cases |
|---|
| Paraspinous mass lesions | Small round cell tumour | 1 |
| Metastatic adenocarcinoma | 1 |
| Chondroma | 1 |
| Embryonal CA | 1 |
| Granulomatous lesion | 1 |
| Non specific infection | 1 |
| Retroperitoneal masses | Small round cell tumour | 3 |
| Lymphoma | 1 |
| Metastatic Adenocarcinoma | 1 |
| Spindle cell neoplasm | 1 |
| Kidney cytological diagnosis | Renal cell carcinoma | 1 |
| Renal cell carcinoma | 1 |
| Renal cell carcinoma | 1 |
| Wilm’s tumour | 1 |
| Hypogastrium cytological diagnosis | Lymphoproliferative disorder | 1 |
| Metastatic adenocarcinoma | 1 |
| Ovary cytological diagnosis | Mucinous cystadenoma ovary | 1 |
| Malignant ovarian tumour | 1 |
| Pancreas cytological analysis | Granulomatous lesion | 1 |
| Pseudocyst | 1 |
| Adrenal gland cytological analysis | Pheochromocytoma | 2 |
| neuroblastoma | 1 |
| Small round cell tumour | 1 |
| Right iliac fossa | Inflammatory lesion | 1 |
| Left hypochondrium | GIST | 1 |
The relation of FNA diagnosis to the histopathology of CB was also analysed as shown in [Table/Fig-4,5].
Analysis of FNA and cell block diagnosis.
| FNA | Cell block |
|---|
| Neoplastic | Non neoplastic | Total |
|---|
| Neoplastic | 33 (True positive) | 1 (False positive) | 34 |
| Non neoplastic | 3 (False negative) | 8 (True negative) | 11 |
| Total | 36 | 8 | 45 |
Comparative analysis of FNA and cell block diagnosis.
| Site | No of cases | Cytological diagnosis |
|---|
| Liver | 20 | Hepatocellular carcinoma |
| 11 | Metastatic carcinoma liver |
| Paraspinous | 1 | Round cell tumour [Table/Fig-6] |
| 1 | Metastatic adenocarcinoma |
| 1 | Chordoma |
| 1 | Embryonal carcinoma |
| Retroperitoneum | 1 | Lymphoma (Paraaortic LN) |
| 3 | Round cell tumour |
| 1 | Metastatic adenocarcinoma (paraaortic LN) |
| 1 | Spindle cell lesion [Table/Fig-7] |
| Hypogastrc mass | 1 | Lymphoma |
| 1 | Metastatic adenocarcinoma |
| Ovary | 1 | Malignant ovarian tumour |
| 1 | Mucinous cyst adenoma ovary |
| Renal | 3 | RCC |
| 1 | Wilm’s tumour |
| Adrenal | 1 | Small round cell tumour |
| 2 | Pheochromacytoma |
| 1 | Neuroblastoma |
| Left hypochondrium | 1 | GIST |
| Total | 54 | |
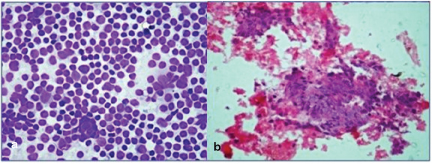
Malignant small round cell tumour.
(a) FNA smears show sheets of monotonous cells with open chromatin. (MGG,40X)
(b) Cell Block section show similar tumour cells. (H&E, 40X).
Out of the 66 cases, adequate material was obtained on FNAC in 64 cases and on CB in 45 cases.
In cases with both FNA and cell block findings (45 cases), 33 were diagnosed as neoplastic (true positive) and 8 cases were diagnosed as non-neoplastic (true negative). Two cases which had haemorrhagic aspirate with few cellular components were diagnosed as neoplastic on cell block sections (False negative). One case diagnosed as benign spindle cell neoplasm [Table/Fig-7] on FNA was diagnosed as Gastro Intestinal Stromal Tumour (GIST) on cell block section along with IHC (False negative). One case of liver nodule, reported as suspicious of malignancy on FNA was diagnosed as regenerative nodule on cell block section (False positive).
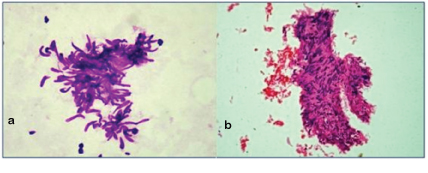
Spindle cell lesion.
(a) FNA smears show clusters of spindle cells. (H&E, 40X).
(b) Cell Block section show spindle cells arranged in whirling pattern. (H&E, 40X).
Additionally, in 21 cases where CB showed no material were, diagnosis was based on aspiration smears alone.
As we did not obtain biopsy or resected sample for histopathological confirmation in all cases, we limited our scope to FNAC and CB study only.
Our study showed a sensitivity of 91.6%, specificity of 88.8%, positive predictive value of 97% and negative predictive value of 72.2%. The diagnostic accuracy was 62% and discordance was 6%.
[Table/Fig-8,9] shows the overall distribution of cases of abdominal lump along with their cytological diagnosis. [Table/Fig-10] gives the details of special stains and IHC done on Cell Block sections.
Neoplastic lesions of abdomen – cytological analysis
| Site | No of cases | Cytological diagnosis |
|---|
| Liver | 20 | Hepatocellular carcinoma |
| 11 | Metastatic carcinoma Liver |
| Paraspinous | 1 | Round cell tumor |
| 1 | Metastatic adenocarcinoma |
| 1 | Chordoma |
| 1 | Embryonal carcinoma |
| Retroperitoneum | 1 | Lymphoma (Paraaortic LN) |
| 3 | Round cell tumor |
| 1 | Metastatic adenocarcinoma (paraaortic LN) |
| 1 | Spindle cell lesion |
| Hypogastrc mass | 1 | Lymphoma |
| 1 | Metastatic adenocarcinoma |
| Ovary | 1 | Malignant ovarian tumor |
| 1 | Mucinous cyst adenoma ovary |
| Renal | 3 | RCC |
| 1 | Wilm’s tumor |
| Adrenal | 1 | Small round cell tumor |
| 2 | Pheochromacytoma |
| 1 | Neuroblastoma |
| Left hypochondrium | 1 | GIST |
| Total | 54 | |
Non neoplastic lesions of abdomen – cytological analysis.
| Site | No of cases | Cytological Diagnosis |
|---|
| Liver | 1 | Diffuse parenchymal disease |
| 1 | Large cell dysplasia |
| 1 | Regenerative nodule |
| 2 | Hydatid cyst |
| 2 | Abscess |
| Paraspinous | 1 | Granulomatous |
| 1 | Inflammatory |
| Pancreas | 1 | Granulomatous |
| 1 | Multicystic lesion |
| Right Iliac fossa | 1 | Inflammatory lesion |
| Total | 12 | |
Special stains and IHC done on CB section.
| Site | Lesion | Special stains on CB | Results | Final Diagnosis |
| Hypogastric mass | Metastatic adenocarcinoma | PASMucicarmineChromogranin | NegativeNegativeFocal Positive | Metastatic adenocarcinoma probably from pancreas |
| Liver | Well differentiated HCC | Reticulin | + | Well differentiated HCC |
| Liver | Regenerative nodule | Reticulin | ++ | Regenerative nodule |
| Pelvic mass | Malignant tumour | CK-7 | Positive | Malignant ovarian tumour |
| Left hypogastrium | Spindle cell lesion | CD 117 | Positive | GIST |
Discussion
FNA cytology has been established as the first line of investigation of mass lesions in different organs and sites. Image guided FNAC plays an immensely beneficial role in diagnosis of deep seated lesions [5]. In addition to smears, CB preparations can be a useful complimentary method for cytological diagnosis. In the present study, the role of CB in guided FNA of abdominal masses was assessed in 66 patients.
Satisfactory aspirate for cytological diagnosis on FNA was obtained in 64 (96.96%) cases in the present study. This is comparable to 92.8% adequacy obtained by Khanna et al., [6]. Satisfactory material on CB was obtained in 45 cases (68.18%) comparable to the study by Nathan et al., who obtained adequate material on CB in 300 cases (73.3%) [4].
In our study the diagnostic sensitivity of smears alone was 96.96%. We agree with the importance of FNAC as an important diagnostic tool but CB was introduced in order to improve the accuracy and the interpretation [7]. In cases of liver lesions, with FNA smears we were able to make a diagnosis of hepatocellular carcinoma but the CB sections showed clearly recognizable patterns like trabecular, solid and acinar pattern as seen in the [Table/Fig-11]. In addition, the thickness of trabeculae was assessed as shown in the [Table/Fig-10], which cannot be done on aspiration. Thus, HCC were further sub-classified depending on the architecture, cytological and nuclear characters into well differentiated HCC (10 cases), moderately differentiated HCC (4 cases), poorly differentiated HCC (5 cases) and fibrolamellar variant of HCC (1 case). 11 cases were reported as metastatic carcinoma deposits to the liver, out of which 7 cases were reported as metastatic adenocarcinoma. 2 were reported as metastatic deposits probably of squamous origin, 1 as poorly differentiated malignancy and 1 reported as malignant melanoma metastasis to liver. In these cases, CB played a very important role in recognizing the architectural pattern and thus aided in arriving at a diagnosis.
In non-neoplastic lesions of the liver, 2 cases where only straw coloured fluid was aspirated, the CB showed hyaline laminated membrane and a diagnosis of Hydatid cyst was given. 1 case of regenerative nodule of liver was studied, where the FNA smears showed sheets of hepatocytes with mild atypical features. The CB showed benign hepatocytes arranged in plates with more than one cell thickness along with clusters of bile duct epithelium and the diagnosis of regenerative nodule was given.
We encountered 2 cases where aspiration was inadequate. However, cell block had enough material and a cytopathological diagnosis was given. 1 was a case from the kidney. CB sections showed clusters of tumour cells with moderate amount of eosinophilic cytoplasm, hyperchromatic nuclei and a prominent nucleoli. With clinical, radiological and CB findings, a diagnosis of Renal cell carcinoma was made. Another case where the diagnosis was made on the basis of CB alone was of ovary. The patient presented with abdomen distension. Computerized Tomography showed a large solid mass in the abdomen with ascites. The exact site of origin was not detected. FNA smears showed only haemorrhage. CB section showed sheets and papillary pattern of pleomorphic tumour cells with abundant mitotic activity. Taking into consideration the fact that the patient was female and with radiological findings, a diagnosis of malignant tumour, probably of an ovarian origin was given. Cytokeratin-7 immuno staining was performed on the CB section which showed positivity as shown in the [Table/Fig-12] and hence, a definitive diagnosis of malignant ovarian tumour was given.
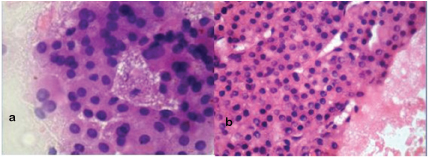
Hepatocellular carcinoma – well differentiated.
FNA smears show tumour cells with abundant cytoplasm, pleomorphic nuclei with prominent intranuclear pseudoinclusions and nucleoli.(H&E,40X) Cell block section showing tumour cells in trabecullar pattern with increase in cell plate thickness.(H&E,40X)
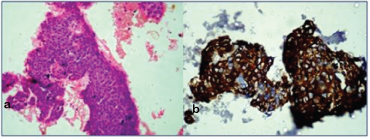
Papillary carcinoma ovary.
Cell Block section show tumour cells arranged in papillary pattern. (H&E, 40X).
IHC- CK 7 on cell block section showing diffused positivity.
Our study showed a sensitivity of 91.6% and specificity of 88.88%. This is comparable to the study done by Abobakar A et al., where the sensitivity and specificity of combined FNA and CB were 97% and 97.5% respectively [8].
Thus, an overall improvement in the final cytopathological diagnosis was noted where smears were complemented by CB. With FNA and CB together, we were able to provide a definitive cytopathological diagnosis in all the 66 cases, increasing the sensitivity to 100%. This study also corresponds to the study done by Khan N et al., in malignant effusion cases, in which 54 (72%) cases were reported positive for malignant cells by CB technique alone while, 42 cases (56%) by cytological smear only. When both the techniques were combined together, the diagnostic yield reached up to 64 cases (85.3%) [9]. Keyhani Rofaga et al., found 55% of original smear diagnosis was improved after the CB was examined [2]. Kern and Heber studied 393 cases of CB preparation. In 273 cases (60.3%) the findings were confirmatory and in 103 (60.3%) cases CB provided additional information for diagnosis [10]. Wojcik and Selvaggi showed that 84% of the cases had identical results on both smears and CB [11].
In our study, out of 66 cases, 52 cases were reported as malignant (78.78%), 2 cases as benign (3.03), 3 cases (5.7%) as tumour-like conditions and 9 cases (17.3%) as non-neoplastic. This is comparable to the study by Pachori RM et al., who had 71.7% malignant lesions [12]. In the present study, CB had adequate material in malignant lesions and thus, was more sensitive for malignant lesions (69.23%) followed by non-neoplastic lesions (66.6%) and benign lesions (60%).
Immunohistochemistry (IHC) on Cell Block
IHC was performed in difficult cases on CB sections which helped us to arrive at definitive diagnosis. The CB sections showed clearly recognizable architecture with minimal shrinkage and aberration.
It was also found in Kung et al., study that the staining results on the CB sections were superior compared to the surgical specimen probably due to very short fixation times [13]. Further, many sections can be cut which permits evaluation of large number of antigens. They can be stored easily.
Thus, CB has much to offer in the utilization of immunocytochemistry.
Furthermore, our data supports the conclusion that though smears may contain adequate diagnostic material, addition of CB would further enhance the specificity of the diagnosis by providing cellular architecture and additional sections for special stains and IHC. CB sections can also be utilized for other ancillary studies like immunophenotypic analysis, ultra structural studies, cytogenetics and polymerase chain reaction [14,15]. [Table/Fig-13] shows the comparative analysis of few similar studies.
Analysis of CB sensitivity in various studies.
| Studies | FNA diagnosis | Cell Block diagnosis | FNA + CB diagnosis |
|---|
| Khan N et al., [9] | 56% | 72% | 85.3% |
| Keyhani Rofaga et al., [2] | 55% | 60% | 86% |
| Richardson et al., [16] | 28% | 68% | 82% |
| Present study | 96.96% | 68.18% | 100% |
Conclusion
A cost effective, simple and reliable technique of Cell Block prepared from residual tissue is a useful adjunct to FNA smears. The Cell Block technique helps to perform special stains and IHC in difficult cases and thus, assists in arriving at a definitive diagnosis. The contribution of Cell Block to the final cytological diagnosis supports the view that CB should be considered in all FNA specimens.