Constitutional Mosaic Trisomy 13 in Two Germ Cell Layers is Different from Patau Syndrome? A Case Report
Fulesh Kunwar1, Vidhi Pandya2, Sonal R. Bakshi3
1 Ph.D. Pursuing, Institute of Science, Nirma University, Sarkhej-Gandhinagar Highway, Ahmedabad, Gujarat, India.
2 Student, Institute of Science, Nirma University, Sarkhej-Gandhinagar Highway, Ahmedabad, Gujarat, India.
3 Assistant Professor, Institute of Science, Nirma University, Sarkhej-Gandhinagar Highway, Ahmedabad, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sonal R. Bakshi, Institute of Science, Nirma University, Sarkhej-Gandhinagar Highway, Ahmedabad - 382 481 Gujarat, India.
E-mail: sonal.bakshi@nirmauni.ac.in
The heterogeneous phenotype of known syndromes is a clinical challenge, and harmonized description using globally accepted ontology is desirable. This report attempts phenotypic analysis in a patient of constitutional mosaic trisomy 13 in mesoderm and ectoderm to make globally comparable clinical description. Phenotypic features (minor/major abnormalities) were recorded and matched with the Human Phenotype Ontology terms that were used to query web-based tool Phenomizer. We report here a case of 24-year-old girl born to non consanguineous parents with history of one abortion. Her phenotypic evaluation included short columella, low-set ears, seizures, enlarged naris, bifid tongue, infra-orbital fold, smooth philtrum, microtia, microcephaly, carious teeth, downslanted palpebral fissures, proportionate short stature, high palate, thin upper lip vermilion, small for gestational age, broad fingertip, broad hallux, mandibular prognathia and dental malocclusion. Karyotype and interphase FISH (Fluorescence in situ hybridization) was done in blood cells. Interphase FISH was also performed on buccal epithelial cells. Cytogenetic analysis demonstrated trisomy 13 mosaicism in 25% cells i.e. 47, XX,+13(9)/46,XX(27). The interphase FISH in blood cells showed trisomy 13 in 15%, whereas in buccal mucosa cells showed nearly 6%. Mosaic aneuploidy in constitutional karyotype can be responsible for variation in clinical and morphological presentation of patient with genetic disorder.
Constitutional karyotyping, FISH, Mosaicism, Patau syndrome, Phenomizer, Phenotyping
Case Report
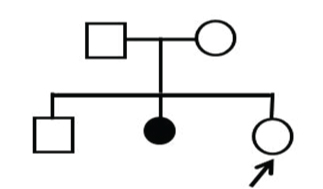
We describe here a 24-year-old female with intellectual disability and various minor and major dysmorphisms. There was no remarkable history during pregnancy and perinatal period. She was the third child born to non-consanguineous, healthy parents when the mother was 24 and the father was 30 years old with a normal male child of 4 years, and a missed abortion at 1.5 months [Table/Fig-1]. The birth history includes cyanosis while crying till the age of 3 years. Her birth weight was 2.2 kg, and global developmental delay was noticed from early infancy. She started sitting at 10 months, walking at 2 years, and unclear speech at 3 years. Current medical history includes moderate mental retardation with IQ (Intelligence Quotient) 35% based on BKT (Binet Kamat Intelligence Test) and DQ (Disability Quotient) 75%. The proband has history of generalised epilepsy, and has a regular menstrual cycle.
Karyotyping: Peripheral blood was collected in heparinised vial aseptically for short term culture from proband and parents after obtaining written informed consent. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Helsinki declaration. Standard protocol was followed for metaphase chromosome preparation and GTG banding for karyotype as per the ISCN (International System for Human Cytogenetic Nomenclature)-2013 [1] using IKAROS software (Metasystems, Germany).
Sample collection from buccal mucosa: Patient was asked to rinse the mouth and using sterile scrapper the upper most layers of inner cheeks were scrapped once and discarded. The same procedure was repeated and the cells of buccal mucosa were collected in 0.9% N-Saline, centrifuged at 3000 rpm for 10 minutes and washed twice. Around 6 ml hypotonic solution was added, mixed well and incubated for 20 minutes before adding 6 ml fresh chilled Carnoy’s fixative and centrifuged to get a clear pellet. Cells were dropped onto clean microscope glass slide and allowed to air-dry.
Fluorescence in situ hybridization (FISH) for chromosome 13 copy number determination in peripheral blood lymphocytes as well as buccal mucosa epithelial cells: The copy number detection was done by FISH using probe mix for chromosome 13 (13q14) & 21 (21q22) each from Kreatech (KBI-40001) as per the manufacturer’s protocol.
Phenomizer query: Phenotypic features in terms of minor/major abnormalities were recorded in consultation with a clinical geneticist and matched with the HPO term and entered in web-based tool Phenomizer. Her phenotypic evaluation included short columella, low-set ears, seizures, enlarged naris, bifid tongue, infra-orbital fold, smooth philtrum, microtia, microcephaly, carious teeth, downslanted palpebral fissures, proportionate short stature, high palate, thin upper lip vermilion, small for gestational age, broad fingertip, broad hallux, mandibular prognathia and dental malocclusion [Table/Fig-2]. Software generated possible differential diagnoses along with p-value in terms of semantic similarity search and also associated genes for pathogenesis.
The phenotypic features of patient with mosaic trisomy 13.

Discussion
A clinical syndrome with trisomy 13 was first described by Patau in 1960 [2]. The global prevalence of trisomy 13 is 1 in 29,000 live births [3]. The Patau syndrome cases have multiple congenital anomalies, mental retardation, and shorter life span [4]. The trisomy 13 can be present as free trisomy or unbalanced or Robertsonian translocation [5]. The Patau syndrome is well-characterized whereas the phenotype of those with mosaic trisomy 13 is heterogeneous [6]. The mosaic cases include combination of euploid and trisomy 13 cells in various percentages [7]. The mosaicism is reported in 6% of individuals with trisomy 13 who have wide phenotypic variability sometimes including unusual skin pigmentation, and longer survival compared to Patau syndrome [8]. The possibility of mosaicism in all the germ cell layers is not ruled out in majority of cases, which may be contributing to variations in morphology.
The considerable variations in phenotype of even a well characterized syndrome like Down syndrome suggests heterogeneity at genetic sequence level, which if identified, can help delineate a disease sub-entity and thus enable more specific genetic counselling, prognosis, and clinical management. Thus it is important to put on record a case of genetic abnormality along with phenotyping by globally uniform methods. In addition to trained clinical geneticist, the genetic researchers can get valuable help from the Phenomizer which is a web-based software tool for matching the phenotypic data with existing known genetic conditions [9].
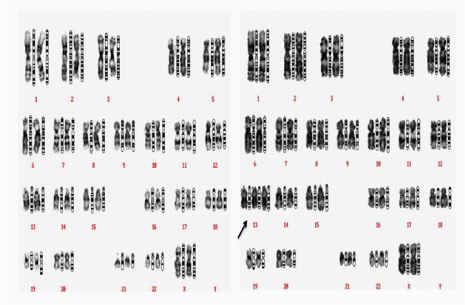
The karyotype [Table/Fig-3] in blood lymphocyte was mos 47,XX,+13(9)/46,XX(27) i.e. the presence of trisomy 13 in 25% of cells. The karyotype of parents was normal which suggests that origin of abnormality was de-novo. The interphase FISH for the cultured cell suspension from blood showed presence of trisomy 13 in 15% of the cells and in case of buccal mucosal cells nearly 6% of the cells showed trisomy 13 [Table/Fig-4]. The result of FISH assay for copy number of chromosome 13 using DNA probe specific for the region 13q14 and internal control 21q22.1 is depicted in [Table/Fig-5]. The FISH signals for centromere of chromosome 13 indicated trisomy in 30 out of 202 cells lymphocytes, and 3 out of 50 cells in buccal mucosa cells. The Phenomizer results based on selected phenotypic features of the proband in terms of various differential diagnoses ranked by their p-value of semantic similarity is shown in [Table/Fig-6].
Karyotyping of patients showing mos 47,XX,+13(9)/46,XX (27).
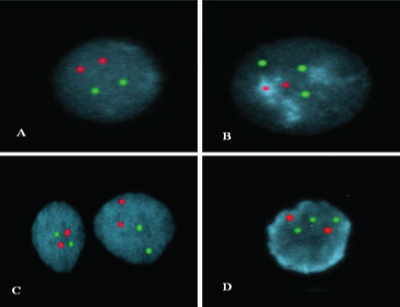
Interphase FISH using Repeat-Free™ Poseidon™ Chromosome 13 (13q14) &21(21q22) specific Probes in a mosaic trisomy 13 case in blood lymphocytes as well as buccal cells. Interphase cells from blood lymphocytes showing normal signals (A) and trisomy 13 (B); Interphase cells from buccal showing normal signals (C) and trisomy 13 (D).
Results of fluorescence in situ hybridisation performed on interphase nuclei using the Kreatech PN 13(13q14) and PN 21(21q22.1) on blood lymphocytes and buccal mucosa epithelial cells.
| Green(13q14) | Orange(21q22.1) | No. of cells | Interpretation |
|---|
| Blood | Buccal mucosa |
|---|
| Chromosome | 13 | 21 | | | |
| Signals per cell | 2 | 2 | 172 | 47 | Normal 13 chromosome pair |
| 3 | 2 | 30 | 3 | Trisomy 13 |
Result generated by web based software Phenomizer showing ranked list of possibilities and associated gene based on score and p-value.
| Known genes | Disease entry | Score | p- Value |
|---|
| KDM5C | #300534 MENTAL RETARDATION,X-LINKED SYNDROMIC,CLAES-JENSEN TYPE;MRXSCJ;;MENTAL RETARDATION,X-LINKED, SYNDROMIC,JARIDIC-RELATED;MRXSJ(OMIM:300534) | 2.5242 | 0.0006 |
| %227330 FACIODIGITOGENITAL SYNDROME, AUTOSOMALRECESSIVE;;AARSKOG-LIKESYNDROME;;KUWAIT TYPEFACIODIGITO-GENITALSYNDROME (OMIM:227330) | 2.4787 | 0.0006 |
| KDM6A | #300867 KABUKI SYNDROME 2;KABUK2 (OMIM:300867) | 2.4657 | 0.0006 |
| 606155 FRYNS-AFTIMOS SYNDROME;PACHYGYRIA, MENTAL RETARDATION,EPILEPSY, AND CHARACTERSTICFACIES; CEREBROOCULOFACIALLYMPHATIC SYNDROME;COFL SYNDROME;;MENTALRETARDATION WITH EPILEPSYAND CHARACTERSTIC FACIES(OMIM:606155) | 2.4259 | 0.0006 |
| 612948 STARGARDT MACULARDEGENERATION, ABSENT ORHYPOPLASTIC CORPUS CALLOSUM,MENTAL RETARDATION, ANDDYSMORPHIC FEATURES (OMIM:612948) | 2.3148 | 0.0006 |
| 157980 MOMO SYNDROME;MACROSOMIA, OBESITY,MACROCEPHALY, AND OULARABNORMALITIES (OMIM:157980) | 2.2899 | 0.0006 |
| ATKIN-FLAITZSYNDROME (OMIM:300431) | 2.2454 | 0.0006 |
| 600991 HYDROCEPHALUS,SPRENGEL ANOMALY, ANDCOSTOVERTEBRAL DYSPLASIA(OMIM:600991) | 2.2084 | 0.0006 |
| MCDONOUGH SYNDROME(OMIM: 248950) | 2.1908 | 0.0006 |
| CHROMOSOME 5P13DUPLICATION SYNDROME(OMIM:613174) | 2.1363 | 0.0006 |
The mosaic aneuploid chromosome complement in constitutional karyotype of a patient with genetic disorder would have different clinical and morphological picture as compared to complete aneuploidy as discussed above. With the advent of Interphase FISH, it has become possible to detect tissue specific mosaicism because the extent of mosaicism is known to vary significantly among different tissues [10].
The Phenomizer query using entry of phenotypic feature indicated possibility of Mental Retardation (X-linked), Faciodigitogenital Syndrome and Kabuki Syndrome with 2.5242, 2.4787 and 2.4657 scores respectively having 0.0006 p-values. The Phenomizer query results did not indicate Patau syndrome or mosaic trisomy 13 conditions which seem to be due to non-classical or variant phenotypic features of the proband. This kind of observation is not unlikely as the variation in genetic abnormalities is enormous, making each case a unique disease entity in itself; which translates into increasing need for customized clinical, diagnostic, and management approaches. The identification of such subtle genetic alterations indicate that by systematic and combined approaches of genetic analysis and phenotypic analysis the proportion of cases categorized as ideopathic mental retardation can be reduced as on identification of underlying genetic anomaly these do not remain idiopathic.
Studies have also shown that some patients did not show typical Patau gestalt due to variability in the tissue distribution of the trisomic cells. It is also expressed by some that there is no clear association between the level of mosaicism, the severity of the phenotype and potential survival at birth [11,12]. A decrease in the percentage of abnormal cells with age has also been noted in the literature, and which may be due to a natural selection against the abnormal cells [11,12]. The present report of mosaic trisomy 13 in more than one germ cell layers and phenotyping with harmonized terms of Phenomizer combines the genotype and phenotype analysis for a more precise categorization of genetic conditions that are rare and hence pose a clinical challenge.
We have reported earlier rare cases of abnormal constitutional karyotypes characterized using molecular cytogenetic methods i.e. mosaic partial trisomy of chromosome 21 [13] and mosaic tetrasomy of chromosome 18p [14]. These cases presented with supernumerary marker chromosome on karyotype analysis initially and had various minor phenotypic anomalies. Such findings of rare constitutional cytogenetic abnormality with detailed phenotypic description can be put on record to help delineate rare subentities of genetic conditions.
Conclusion
The abnormal constitutional karyotype analysis in cases of suspected genetic conditions can be aided with targeted molecular cytogenetics in more than one germ cell layers which is not generally reported. This information reveals the origin of genetic aberration at the developmental stage. The correlation of genotypic aberration with phenotypic details in cases of genetic conditions can be very important for the Human Phenome Project and should be carried out using harmonized tools like Phenomizer.
[1]. Shaffer LG, McGowan-Jorda J, Schmid M, An International System for Human Cytogenetic NomenclatureS. Karger AG, Basel 2013 :140 [Google Scholar]
[2]. Edwards JH, Harnden DG, Cameron AH, Crosse VM, Wolff OH, A new trisomic syndromeLancet 1960 1(7128):787-90. [Google Scholar]
[3]. Locock L, Crawford J, Crawford J, The parents’ journey: continuing a pregnancy after a diagnosis of Patau’s syndromeBMJ (Clinical researched) 2005 331(7526):1186-89. [Google Scholar]
[4]. http://patient.info/doctor/pataus-syndrome-trisomy-13 [Google Scholar]
[5]. Eubanks SR, Kuller JA, Amjadi D, Powell CM, Prenatal diagnosis of mosaic trisomy 13: a case reportPrenat Diagn 1998 18(9):971-74. [Google Scholar]
[6]. Delatycki MB, Pertile MD, Gardner RJ, Trisomy 13 mosaicism at prenatal diagnosis: dilemmas in interpretationPrenat Diagn 1998 18(1):45-50. [Google Scholar]
[7]. Pachajoa H, Meza Escobar LE, Mosaic trisomy 13 and a sacral appendageBMJ Case Reports 2013 :bcr2012008150 [Google Scholar]
[8]. Gonzalez-del Angel A, Estandia-Ortega B, Gavino-Vergara A, Saez-de-Ocariz M, Velasco-Hernandez MD, Salas-Labadia C, A patient with trisomy 13 mosaicism with an unusual skin pigmentary pattern and prolonged survivalPediatr Dermatol 2014 31(5):580-83. [Google Scholar]
[9]. Kohler S, Schulz MH, Krawitz P, Bauer S, Dolken S, Ott CE, Clinical diagnostics in human genetics with semantic similarity searches in ontologiesAm J Hum Genet 2009 85(4):457-64. [Google Scholar]
[10]. Halder A, Fauzdar A, Potential use of blood, buccal and urine cells for rapid noninvasive diagnosis of suspected aneuploidy using fluorescence in situ hybridization (FISH)J Clin Diagn Res 2007 1:33-38. [Google Scholar]
[11]. Delatycki M, Gardner RJ, Three cases of trisomy 13 mosaicism and a review of the literatureClin Genet 1997 51(6):403-07. [Google Scholar]
[12]. Chen M, Yeh GP, Shih JC, Wang BT, Trisomy 13 mosaicism: study of serial cytogenetic changes in a case from early pregnancy to infancyPrenat Diagn 2004 24(2):137-43. [Google Scholar]
[13]. Bakshi SR, Dave BJ, Sanger W, Brahmbhatt MM, Trivedi PJ, Kakadia PM, Characterization of a familial small supernumerary marker chromosome in a patient with adult-onset tongue cancerCytogenetic and Genome Research 2008 121(1):14-17. [Google Scholar]
[14]. Bakshi SR, Brahmbhatt MM, Trivedi PJ, Chudoba I, Constitutional Tetrasomy 18pIndian Pediatrics 2006 43:357-60. [Google Scholar]