Valvular heart disease is a common and an important clinical diagnosis throughout the world; and the commonest cause is Rheumatic heart disease. Upto 0.3% of children with group A beta-hemolytic Streptococcal pharyngitis develop acute Rheumatic fever. Pancarditis with valvular insufficiency, pericarditis, heart failure and even death may be present in 39% of patients with acute Rheumatic fever. Patients with chronic Rheumatic heart disease develop valvular stenosis with varying degrees of regurgitation, arrhythmias, atrial dilatation and ventricular dysfunction [1].
Echocardiography is the gold standard investigation for the evaluation of valvular heart disease. Recent reports have suggested that dynamic cardiac Magnetic Resonance (MR) imaging may serve as an attractive alternative or complement to the echocardiography in the assessment of valvular pathologies [2]. This noninvasive technique provides three-dimensional (3D) anatomic and functional data and also aids in more accurate measurement of ventricular function than is possible with echocardiography [3]. Velocity-Encoded Cine (VEC) MRI allows accurate estimation of velocity profiles across a valve or any vascular structure and provides quantitative measurements comparable to those provided by echocardiography [4]. In addition, as compared to echocardiography, MRI does not have the limitations with respect to acoustic penetration of different portions of the heart and therefore better demonstrates flow velocity and morphology throughout the cardiovascular structures.
The advantages of a MRI study is it can provide much of the information required for evaluating the affected cardiac valves, defining the valvular anatomy, assessing the nature and effects of valvular dysfunction and is reproducible [5]. The disadvantages of MRI are limitations like lengthy imaging time, patient claustrophobia, high examination cost and requires skilled technique.
The study was undertaken to define the role of MRI in the evaluation of Rheumatic valvular heart disease and to compare the role of MRI with transthoracic echocardiography with regard to quantity of stenosis and volume regurgitation.
Materials and Methods
A prospective longitudinal study was conducted in a tertiary care hospital in Department of Radiology, Mumbai, over a period of four years from 06 January 2009 to 05 January 2013 in a selected population of 50 patients.
Inclusion criteria: The study population included patients of all ages and both sex (males & females), who were known cases of chronic Rheumatic valvular heart disease diagnosed on transthoracic 2D- Echo and were referred from Department of Cardiology.
Exclusion criteria: Patients who were critically ill, in severe cardiac failure and with prosthetic valves and other implants, were excluded from this study.
Technique
The individual information, clinical history and findings of every patient were recorded in a prescribed format. A chest radiograph was done in all patients. A repeat Echocardiography was performed by the Cardiologist in all patients two days before the MRI by using a PHILIPS SONOS 5500 Echocardiography machine. Informed consent was taken from all patients. A patient population of all ages was selected with females being the dominant group of the study (58%).
ECG gated cardiac MRI was performed in all patients with a 1.5-Tesla system (MAGNETOM SYMPHONY- Model 2005) using basic cardiac software (Argus viewer) by a phased-array multicoil. All the patients were given a mild sedation before cardiac MRI. Four patients were found to be having tachycardia and were given B-blockers (T. Metaprolol 12.5 mg b.d.) for three days.
Localizer images were obtained in the coronal, sagittal and transverse planes and followed by Turbo spin echo and Turbo fast low angle shot sequences (FLASH) - two dimensional with a 280–320-mm field of view and slice thickness 5 mm were done. A flip angle of 180 degrees for Turbo spin echo and 30 degrees for Turbo fast low angle shot sequences (FLASH) - two dimensional sequences were used. Both breath hold and breath hold cine mode (4 frames / s) sequences were done. In addition T1 weighted (T1W), T2 weighted (T2W), Half-Fourier Acquisition Single-Shot Turbo Spin-Echo (HASTE) and Prospective Acquisition Correction (PACE) sequences were studied. The average time spent by study group in the MRI Gantry was 40-45 min.
Ethics
All procedures done were in accordance with the standards of the Institutional Ethics Committee.
Statistical Analysis
The results were presented in number for the data in tables. All the data was analysed using SPSS software version. Statistical significance was accepted when p<0.05.
Results
[Table/Fig-1] shows predominance of mitral stenosis in our study both as an isolated abnormality and in combination with other valvular lesions. All cases of significant valvular stenosis and regurgitations on Echo are confirmed by MRI.
Comparision of diagnosis by clinical, ECHO and MRI.
| S. No. | Clinical diagnosis | No of pts | ECHO diagnosis | No of pts | MRI diagnosis | No of pts |
|---|
| 1. | AR | 9 | AR | 9 | AR | 9 |
| 2. | AS | 9 | AS | 8 | AS | 8 |
| | | AS&AR | 1 | AS&AR&EAA | 1 |
| 3. | AS&AR | 1 | AS&AR | 1 | AS&AR | 1 |
| 4. | LVOT-O | 2 | AS | 1 | AS | 1 |
| | | AS(M)&EAA | 1 | EAA | 1 |
| 5. | MR | 7 | MR | 7 | MR | 7 |
| 6. | MS | 11 | MS | 9 | MS | 9 |
| | | MS&AR(M) | 1 | MS | 1 |
| | | MS&LAT | 1 | MS&LAT | 1 |
| 7. | MS&AR | 3 | MS&AR | 3 | MS&AR | 3 |
| 8. | MS&AS | 1 | MS&AS | 1 | MS&AS | 1 |
| 9. | MS&MR | 3 | MS&MR | 3 | MS&MR | 3 |
| 10. | RHD+D | 1 | PE&AR(M) | 1 | PE | 1 |
| 11. | RHD+F | 1 | MS&MR&AR(M) | 1 | MS&MR | 1 |
| 12 | RVOT-O | 1 | PS(M) | 1 | N | 1 |
| 13. | TR | 1 | TR | 1 | TR | 1 |
| Total | 50 | | 50 | | 50 |
AR (Aortic regurgitation), AS (Aortic stenosis), EAA (Ecstasia of ascending aorta), LVOT-O (Left ventricular outflow tract obstruction), RVOT-O (Right ventricular outflow tract obstruction), MR (Mitral regurgitation), MS (Mitral stenosis), LAT (Left atrial thrombus), RHD+D (Rheumatic heart disease with dyspnoea), RHD+F (Rheumatic heart disease with fever), PE (Percardial effusion), PS (Pulmonary stenosis), TR (Tricuspid regurgitation), M (Mild).
[Table/Fig-2] shows significant correlation between the findings of Echo and MRI for ejection fraction. The coefficient of correlation (r) was 0.82 for average Ejection Fraction (EF) which means a strong positive association between the results by ECHO and MRI and the p-value is <0.00001, that is the test is highly significant.
Comparison of Ejection Fraction (EF) between ECHO and MRI
| S.No | EF(Echo) | EF(MRI) | r | F.Statistic | p |
|---|
| 1. | 64.94±7.11(48-78) | 67.52±7.84(50-80) | 0.82 | 225.28 | <0.00001 |
EF (Echo)-Ejection fraction by Echo, EF (MRI)- Ejection fraction by MRI, r- Coefficient of Correlation.
[Table/Fig-3] shows significant correlation between the findings of Echo and MRI for valve areas. The coefficient of correlation is 0.98 for average mitral valve area (V.A) and 0.92 for average aortic valve area (V.A) indicating a strong positive association between the results by ECHO and MRI. The p-value is <0.00001 suggesting that the test is highly significant
Comparision of Valve area (V.A) (cm2) between ECHO and MRI.
| S.No | Valve | V.A (ECHO) Cm2 | V.A.(MRI) Cm2 | r | F. Statistic | p |
|---|
| 1. | Mitral | 1.79±0.43(0.99-2.53) | 1.82±0.47(0.96-2.58) | 0.98 | 2623.47 | <0.00001 |
| 2. | Aortic | 1.10±0.21(0.65-1.90) | 1.12±0.25(0.70-1.98) | 0.92 | 2582.56 | <0.00001 |
V.A (ECHO) - Valve area by Echo, V.A. (MRI) - Valve area by MRI, r - Coefficient of Correlation.
Echocardiography had a sensitivity of 98% and specificity of 100% and cardiac MRI was having a sensitivity of 90% and specificity of 50% in the diagnosis of valvular lesions in our study.
Discussion
The most common pathological cause of valvular heart disease is Rheumatic heart disease in children and young adults and most common non pathological cause is degenerative valvular disease in older population [6]. Rheumatic heart disease is the most serious complication of Rheumatic fever. The most common valvular abnormality is mitral regurgitation followed by mitral stenosis, aortic regurgitation and aortic stenosis [7]. At present a variety of imaging techniques are available for the diagnosis and characterization of valvular pathologies and assess concomitant anatomy, with echocardiography still being the clinical "workhorse" [8].
In this study we selected 50 patients who were known cases of Rheumatic valvular heart diseases with females being the dominant group (58%). Mitral stenosis, either as an isolated valvular abnormality, or, in combination with other valvular abnormalities [Table/Fig-1] constituted the major bulk of study.
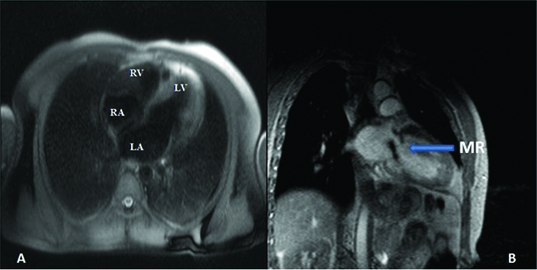
In our study, all the cases of significant valvular regurgitation that were diagnosed by ECHO were confirmed by MRI [Table/Fig-4&5] and the data is comparable to series of Schiebler M et al., and Gelfand EV et al., [9,10].
A) Spin echo image shows four chamber view, B) Cine imaging shows regurgitation through mitral valve into left atrium in a 22 year old female.
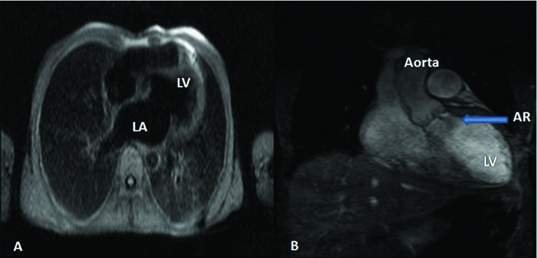
A) Spin echo image shows four chamber view, B) Cine imaging shows regurgitation through aortic valve into left ventricle in a 45 year old male.
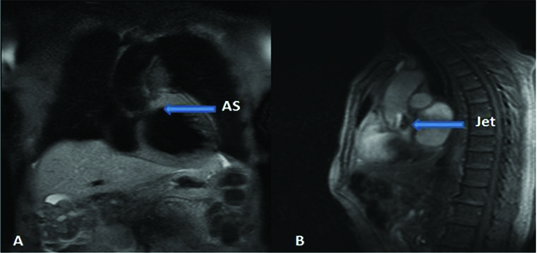
All the cases of significant Aortic Stenosis (AS) that were diagnosed by ECHO were confirmed by MRI [Table/Fig-6]. This data is comparable with studies done by Caruthers SD et al., [11].
A) Spin echo image shows aortic stenosis, B) Cine imaging in sagittal plane shows jet through stenosed aortic valve into Aorta in a 62 year old male.
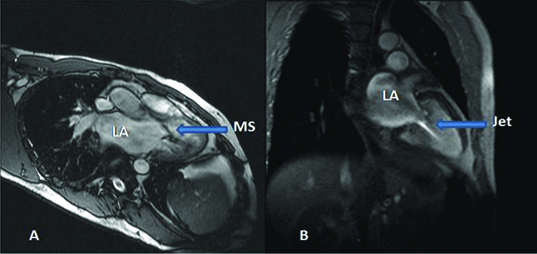
All the cases of significant Mitral Stenosis (MS) that were diagnosed by ECHO were confirmed by MRI [Table/Fig-7] and the data is comparable to series of Lin SJ et al., and Djavidani B et al., [12,13].
A) Spin echo image shows mitral stenosis, B) Cine imaging shows jet through stenosed mitral valve into left ventricle in a 41 year old male.
The coefficient of correlation (r) was 0.82 for average Ejection Fraction (EF) which means a strong positive association between the results by ECHO and MRI. The p-value is <0.00001, that is the test is highly significant [Table/Fig-2]. These data are comparable with studies done by Grothues F et al., and Demir H et al., [14,15].
The coefficient of correlation is 0.92 for average aortic valve area (V.A.) and 0.98 for average mitral valve area (V.A) which means a strong positive association between the results by ECHO and MRI. The p-value is <0.00001, that is the test is highly significant [Table/Fig-3]. This data is comparable to series of Lin SJ et al for the assessment of mitral valve area and Reant P et al., for the assessment of aortic valve area [12,16].
In our study, Echocardiography had more sensitivity & specificity (98% and 100% respectively) as compared to cardiac MRI (90% and 50% respectively) in the diagnosis of valvular lesions. MR imaging could not detect mild pulmonary stenosis in one patient, mild aortic stenosis in one patient and mild aortic regurgitation in three patients [Table/Fig-1]. Infact MRI proved to be less efficient in detecting mild valvular stenosis and mild regurgitation.
The Echocardiography has the advantages of being cheap, fast, easily available, portable modality with superior spatial and temporal resolution. It also has the maneuverability to achieve the optimal angulation for measurement of peak velocities. Echocardiography is still the procedure of choice for obtaining anatomic and pathological information regarding valve thickness, number of leaflets and presence of vegetations in endocarditis. Technical limitations due to poor acoustic window and operator dependency are the disadvantages of echocardiography [17].
On the other hand, MRI with its multiplanar capability, good spatial resolution, non ionizing radiation and better soft tissue demonstration, is more accurate at quantification of ancillary findings in valve disease viz mitral stenosis, mitral regurgitation, aortic stenosis and aortic regurgitation. Without any hazards of radiation, this non invasive technology has proved to be the standard of reference for measurement of ventricular mass, cardiac volumes, ejection fraction and is reproducible method of quantifying valvular stenosis and regurgitation. Dynamic MR imaging is useful in the assessment of ventricular function accurately, which is required for long-term follow-up and preoperative evaluation of patients and also helps in determining optimal timing for surgical intervention [18]. Unlike echocardiography, Velocity Encoded Cine (VEC) MR imaging allows more comprehensive evaluation of pathophysiologic changes in valvular disease by providing combined measurements of flow volume and velocity [5]. Due to low inter-study variability, cardiac MRI is an optimal technique for serial assessment of valvular pathologies in patients that are managed expectantly [19].
The disadvantages of MR examination is being high equipment and examination cost, increased acquisition time, requirement of skilled technique and patient claustrophobia. Although some studies have shown echo planar MR imaging to be useful in evaluating the motion of cardiac valves in real time, significant improvements are still required for this modality to be competitive with echocardiography in this setting [5].
Limitation
The limitations in our study are lengthy imaging time and availability of only basic cardiac software (Argus viewer) with the model of 2005 and MRI was unable to detect mild valvular stenosis and mild regurgitation.
Conclusion
In our study Echocardiography was found to be the gold standard for the diagnosis of Rheumatic valvular heart disease and the role of MRI remained only complimentary to Echocardiography due to limitations in its technology. However with advanced cardiac software, more advanced techniques, and faster imaging sequences, MRI will become a routine procedure for investigation and follow-up of patients with valvular heart disease.
AR (Aortic regurgitation), AS (Aortic stenosis), EAA (Ecstasia of ascending aorta), LVOT-O (Left ventricular outflow tract obstruction), RVOT-O (Right ventricular outflow tract obstruction), MR (Mitral regurgitation), MS (Mitral stenosis), LAT (Left atrial thrombus), RHD+D (Rheumatic heart disease with dyspnoea), RHD+F (Rheumatic heart disease with fever), PE (Percardial effusion), PS (Pulmonary stenosis), TR (Tricuspid regurgitation), M (Mild).
EF (Echo)-Ejection fraction by Echo, EF (MRI)- Ejection fraction by MRI, r- Coefficient of Correlation.
V.A (ECHO) - Valve area by Echo, V.A. (MRI) - Valve area by MRI, r - Coefficient of Correlation.