Hernia is an abnormal protrusion of an organ or tissue through a defect in its surrounding walls. It can be divided into internal, external and diaphragmatic hernias. Most of them can be asymptomatic. If they become symptomatic they can present with features of intestinal obstruction, incarceration or strangulation. In this case series we compare the incidence of these rare presentations of hernias with world literature and to warn surgeons not to cut the obstructing band in cases of internal hernias. In this case series, we review the clinical details of 7 rare presentations of hernia, who presented with various types of hernias to a tertiary care centre in Kerala over a period of one year. Of these 7 cases 6 cases were internal hernias (3 left paraduodenal hernias, 2 transmesentric hernias, and 1 pericaecal hernia) and a case of spigelian hernia above the level of umbilicus. All of them presented as acute abdomen in the emergency department. Among these 7 cases, only one case was diagnosed preoperatively. Three patients had bowel gangrene and had to undergo resection- anastomosis of the bowel. The survival rate among these cases was 100% as compared to 50% in the world literature if they had been left untreated. Even though internal hernias are a rare entity, we need to have it as a differential diagnosis in case of intestinal obstruction, in a previously non-operated abdomen.
Abdominal wall abscess, Internal hernia, Intestinal obstruction, Spigelian hernia
Case Series
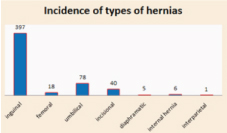
Over a period of one year from March 2014 to March 2015, a total of 695 patients with hernia and intestinal obstruction were considered retrospectively. Of these, 545 patients were hernia cases (both elective and emergency), and the rest were intestinal obstruction cases, from other causes. Among the hernias most were inguinal hernias (397 patients) and internal hernias were constituted by 6 cases. All of them presented as acute intestinal obstruction, constituting 1.8% of acute intestinal obstruction cases [Table/Fig-1].
Total incidence of various types of hernias in our tertiary care centre over a period of one year. Internal hernias forms 1.1% of all types of these hernias.
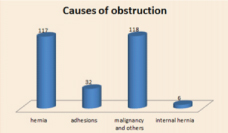
Shows the total intestinal obstruction cases over a period of one year. 1.8% of these obstruction cases were constituted by obstruction due to internal hernias.
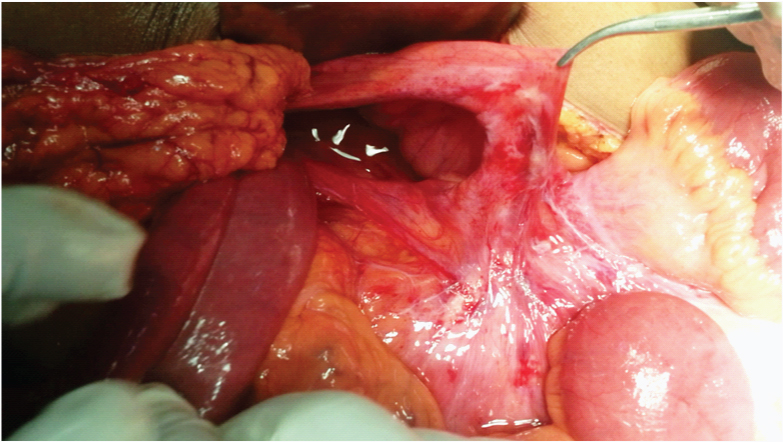
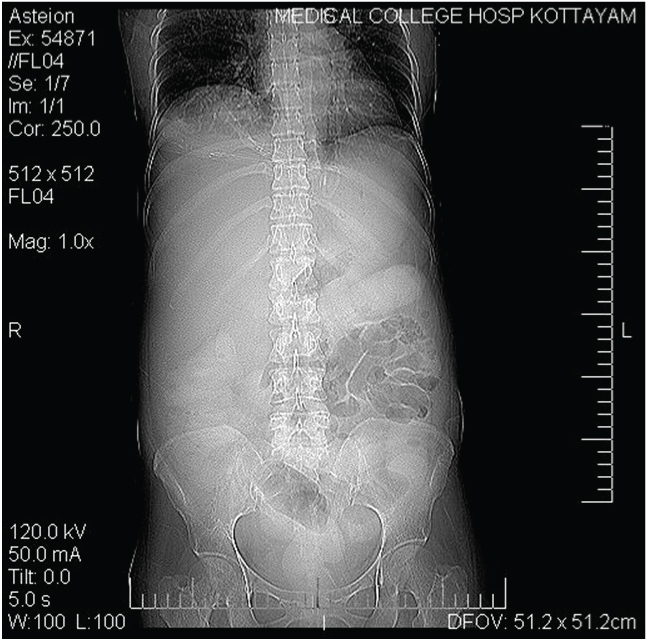
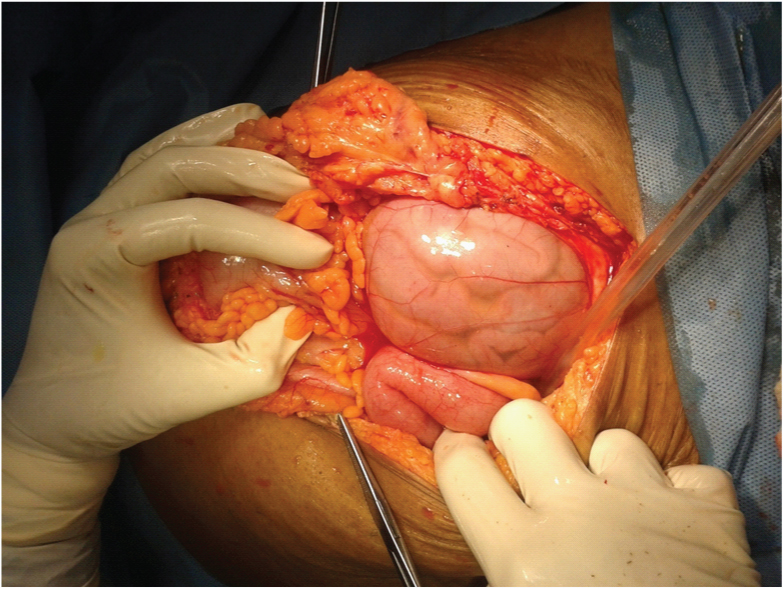
Case 1: Patient presented to our emergency department with features of intestinal obstruction. History of similar complaints were present previously which had subsided on its own. He was dehydrated and tachycardia was present. Abdomen was distended with diffuse tenderness and guarding. X ray abdomen showed multiple air fluid levels and dilated bowel loops. He was posted for emergency exploratory laparotomy. Intraoperatively ileum was found herniating through the left paraduodenal fossa with constricting band formed by inferior mesenteric vein and the proximal small bowel was found dilated [Table/Fig-2]. The contents of the hernia were reduced and the inferior mesentric vein was preserved. Defect was closed with the free peritoneum to the lateral border of duodeno-jejunal flexure, retroperitonialising the inferior mesenteric vein. Postoperative period was uneventful and he was discharged on day 7.
Shows the left paraduodenal fossa (Landzert’s fossa) with the inferior mesenteric vein forming the free edge of the defect through which the bowel was found herniating.
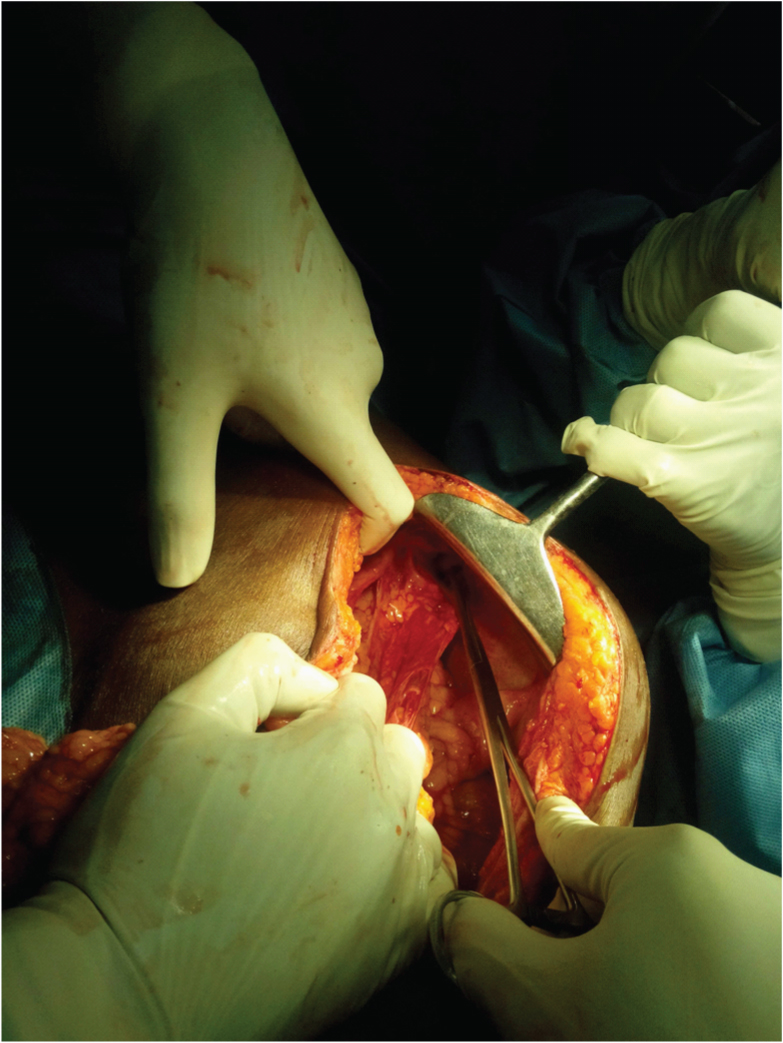
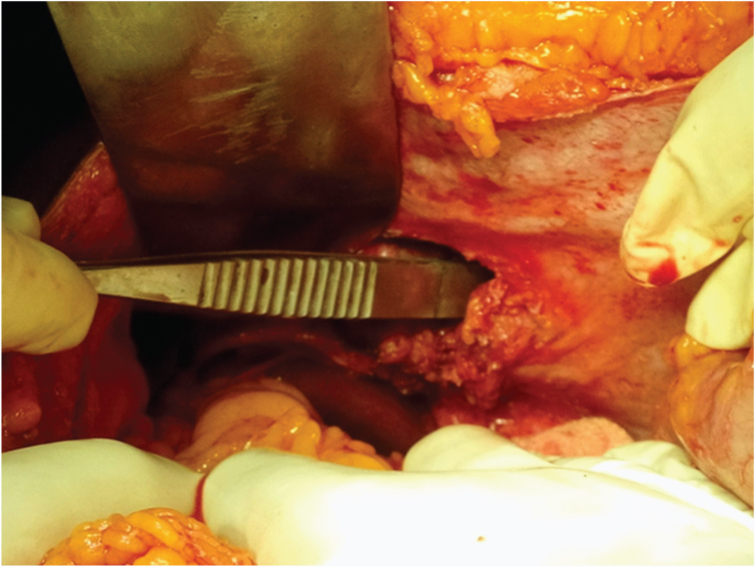
Case 2: Patient presented to our casualty with features of intestinal obstruction. He was febrile and dehydrated, tachycardia was present. Abdomen was distended, with diffuse tenderness, guarding and rebound tenderness. X ray abdomen showed multiple air fluid levels and dilated small bowel loops. He was posted for emergency exploratory laparotomy. During laparotomy ileum was found herniated in the left paraduodenal fossa with 50 cm of ileum found gangrenous within it and proximal segment dilated [Table/Fig-3,4]. The constriction band was formed by inferior mesenteric vein. The contents were reduced, gangrenous bowel was resected and an end to end ileo-ileal anastomosis was done in two layers. The defect was closed with peritoneum to the DJ flexure after preserving the inferior mesenteric vein. Postoperative period was uneventful and he was discharged on postoperative day 9.
Shows the dilated small bowel in the left paraduodenal fossa.
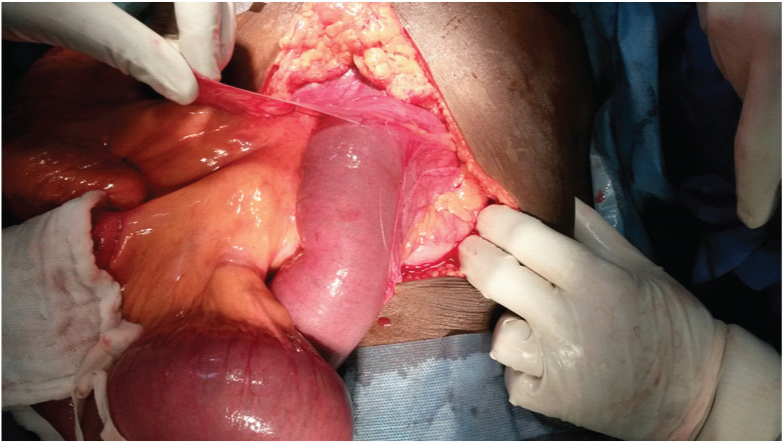
Shows the segment of the small bowel which was found gangrenous in the left paraduodenal hernia sac, which was later resected and an end to end ileo-ileal anastomosis was done.

Case 3: A chronic liver disease patient admitted in medicine ward presented to emergency department with features of intestinal obstruction. X ray abdomen showed multiple air fluid levels and Contrast Enhanced Computerized Tomography (CECT) abdomen showed encapsulation of distended bowel loops in an abnormal location in the left hypochondrium, with hepatomegaly and ascites [Table/Fig-5]. She was transferred to the surgery department for emergency exploratory laparotomy. Intraoperatively ascites was present. Liver was massively enlarged and ileum was found herniating through the left paraduodenal fossa and covered by peritoneal sac and the constricting band was formed by the inferior mesenteric vein causing obstruction [Table/Fig-6]. Sac was opened, contents were reduced and the defect was closed with the peritoneum to the lateral aspect of duodeno-jejunal flexure after preserving the inferior mesenteric vein. Postoperatively she was transferred to surgery ICU because of hypotension. She could not be revived and expired on postoperative day 3 due to cardiac cause.
CECT abdomen of the patient showing encapsulated small bowel in an abnormal location in the left side of the abdomen.
Showing the small bowel within the sac in the landzert’s fossa.
Case 4: Patient presented to our casualty with features of intestinal obstruction. He was febrile, dehydrated and tachycardia was present. Abdomen was distended with rebound tenderness. Total leukocyte count was 27,000\mm3. X ray abdomen showed multiple air fluid levels and dilated small bowel loops. He was posted for emergency exploratory laparotomy. Intraoperatively small bowel was found herniated in the pericaecal region, between peritoneal bands, with 75 cm of ileum gangrenous and proximal small bowel found dilated [Table/Fig-7]. The contents were reduced. Gangrenous segment was resected and an end to end ileo-ileal anastomosis was done in two layers. The hernial defect was closed by approximating the peritoneal bands. He was discharged on postoperative day 10.
Showing a segment of small bowel, seen gangrenous in the pericaecal hernia, which was later resected and an end to end ileo- ileal anastomosis was done.

Case 5: A chronic calcific pancreatitis patient who had undergone Frey’s procedure from a hospital in Tamil Nadu 2 years back, now presented with complaints of intestinal obstruction. CECT abdomen showed features of mechanical obstruction of bowel. He was posted for emergency exploratory laparotomy. During laparotomy the small bowel was found herniating through a defect in the transverse mesocolon near the previous anastomotic site with 50 cm of ileum found gangrenous within. Contents were reduced, the gangrenous segment was resected, and an end to end ileo-ileal anastomosis was done in two layers. The defect in the transverse mesocolon was closed. He was discharged on postoperative day 9.
Case 6: A 57-year-old female who had undergone subtotal gastrectomy with a Roux- en- Y reconstruction for a stomach GIST 2 years back. Now she presented to our casualty with complaints of intestinal obstruction. She was dehydrated, tachycardia was present. Abdomen was distended with diffuse tenderness. X ray abdomen showed dilated small bowel loops with multiple air fluid levels. Initially she was managed conservatively by nasogastric aspiration and IV fluids. But symptoms were persisting and hence she was posted for exploratory laparotomy. Intraoperatively ileum was found herniating though a rent in the Roux loop of jejunum causing obstruction. The ileum was reduced. The defect was closed by approximating mesocolon to the roux loop. She was discharged on postoperative day 7.
Case 7: A-45 year-old female came to emergency department with complaints of a swelling over left side of the abdomen, associated with fever and pain. No history of any trauma, or any similar illness in the past. She was febrile with a 10 x 8 cm tender parietal swelling in the left lumbar region extending to the left hypochondrium, the rest of the abdomen was normal. Ultrasound scan of the abdomen was suggestive of an abdominal wall abscess and it was drained with a catheter under ultrasound guidance. Despite this, after 4 days the swelling was persisting. Repeat ultrasound was taken, which showed persistence of pus in the region with some intra-abdominal structure communicating with the abscess cavity. She was posted for exploratory laparotomy. Intraopetratively the abscess cavity was laid open, and proceeded with laparotomy. It was found that the cavity was tracking to the left hypochondrium with a defect in the abdominal wall through which omentum was herniating which got strangulated [Table/Fig-8,9]. The contents were reduced. Strangulated omentum was resected, defect in the abdominal wall closed in layers with polypropylene. Postoperative period was uneventful and she was discharged 2 weeks after admission.
Shows the omentum herniating through the defect in the left hypochondrium, which was strangulated in the interparietal region presenting as an abscess.
Shows the defect in the left hypochondrium.
In this case series, we had 7 rare cases of hernias, of which, one was a spigelian hernia occurring above the level of umbilicus. Other 6 cases were internal herniation (3 left paraduodenal hernias, 2 transmesentric hernias and 1 pericaecal hernia) presenting with features of intestinal obstruction [Table/Fig-10]. Among them, only one had preoperative diagnosis of internal hernia. Considering the statistics of the incidence of various types of hernias in our institution over a period of one year, they correspond with that of world literature. The statistics are same for incidence of intestinal obstruction due to these types of hernias. Among these 7 cases 4 patients had strangulation of the contents. The survival in these cases was 100%. The statistics of these rare presentations of hernia are similar to those in the world. All the patients presented with acute abdomen, one had previous history of similar symptoms which subsided on its own.
Summary of the case series
| Patient | Age | Sex | Presenting complaints | Past history/co-morbidities | Type of hernia | Procedure done |
|---|
| Case 1 | 35 | M | Abdominal pain, vomiting, constipation | History of similar complaint present. | Left paraduodenal hernia | Reduction of hernia, closure of defect. |
| Case 2 | 58 | M | Bloody loose stools, vomiting, pain | Nil | Left paraduodenal hernia | Reduction of hernia, resection and anastomosis, closure of defect. |
| Case 3 | 48 | F | Abdominal distension, pain | Chronic liver disease | Left paraduodenal hernia | Reduction of hernia, closure of defect. |
| Case 4 | 73 | M | Abdominal pain, vomiting, constipation | Nil | Pericaecal hernia | Reduction of hernia, resection and anastomosis, closure of defect. |
| Case 5 | 30 | M | Abdominal pain, vomiting, constipation | Post frey’s procedure | Trans-mesenteric hernia | Reduction of hernia, resection and anastomosis, closure of defect. |
| Case 6 | 57 | F | Abdomen pain, vomiting, abdomen distension, constipation. | Post subtotal gastrectomy for stomach gist. | Trans-mesenteric hernia | Reduction of hernia, closure of defect. |
| Case 7 | 45 | F | Swelling left lumbar region, abdomen wall abscess | Nil | Spigelian hernia | Abscess drainage, laparotomy and closure of defect |
Discussion
A hernia is a bulging of part of the contents of the abdominal cavity through a weakness in the abdominal wall [1]. Hernia can occur in all areas, when there is congenital or acquired defects in the walls of body cavities in a case of external hernia or inside the abdominal cavity in a case of internal hernia through which the bowel prolapses [2]. Hernias are common diseases of the abdomen with a global incidence of approximately 4%- 5% [3] and are the most common reason for surgery in patients more than 50 years of age [4]. Of these, inguinal hernias are the most common with prevalence of 75%, followed by femoral (15%), and umbilical (8%) [3]. The male:female ratio is as high as 8:1. In the case of femoral hernia; females are the more commonly affected [4]. Hernias have a wide range of presentation. Mostly they are asymptomatic or may present with non-specific symptoms. But in some cases, the patients can have pain or nausea and, in some cases they can develop acute complications (incarceration, obstruction, volvulus & strangulation) that need prompt diagnosis and treatment [4]. Diagnosis is almost always clinical, but can be difficult in patients with obesity, pain or in rare presentations of hernias; where preoperative imaging may help in the diagnosis. Sometimes it can be an accidental finding intra operatively.
In 1857, Treitz defined an internal hernia as a retroperitoneal protrusion of an abdominal organ through a peritoneal fold [5]. Internal hernia is a rare type of hernia in which the abdominal content herniates through the defect in the peritoneal cavity, which is found either congenitally or is acquired. Congenitally they may be pre-existing anatomical structures like recesses, foramina, or fossa [2]. Internal hernias account for < 1% of all abdominal hernias worldwide. Most of these patients may have nonspecific symptoms, until they present to the casualty with features of intestinal obstruction, abdominal pain, or distension. They mostly present with features of intestinal obstruction, which account for 5.8% of all small bowel obstruction cases [2]. It is classified by Ghahremaani into 6 groups [6]. They are: 1) Paraduodenal hernias (50-55%); 2) Hernias through foramen of Winslow (6-10%); 3) Transmesentric hernias (8-10%); 4) Pericaecal hernias (10-15%); 5) Intersigmoid hernias (4-8%); 6) Paravesical hernias (<4%). Paraduodenal hernias are mainly congenital, due to malrotation of the small bowel and entrapment of the small intestine beneath the mesocolon [7–9]. Two types are seen, left and right. Of these, left paraduodenal hernia is more common. This occurs through the Landzerts fossa [2,9]. Preoperative diagnosis by radiography, oral contrast study or CECT abdomen shows encapsulated bowel loops, at the duodeno-jejunal junction between the stomach and pancreas to the left of the ligament of Treitz in a case of left paraduodenal hernia with or without features of obstruction. The free edge of the defect in the right and left paraduodenal fossa are formed by colonic vessels and usually these structures form the obstructing band. So in these cases we need to be cautious in cutting the obstructing band. Internal herniation through the foramen of Winslow accounts for 6-10% of the internal hernias. The predisposing factors are larger than a normal opening at the foramen of Winslow and, also redundant small bowel with large mesentry [10]. Transmesentric variety of internal hernia accounts for 8-10%, and its incidence is seen to be increasing. It is mainly acquired, occurring due to herniation of bowel loops through defects in the mesentry, following previous surgeries. Other rare varieties are pericaecal, intersigmoid, and paravesical hernias [2]. Even though the treatment for obstructed hernia is release of the obstructing band and reducing the contents, it is not normally done in case of internal hernias as the obstructing band could be major vessels. Here the dilated loops are decompressed and reduced, and the defect is closed either by retroperitonealising the fossa or by approximating the peritoneal bands [10–12].
Spigelian hernia in itself is very rare and is difficult to diagnose clinically. It has been estimated that it constitutes 0.12% of abdominal wall hernias [13]. It was named after Adriaen Van den Spigehel, an anatomist from Belgium who described the fascial defects associated with this rare hernia [14]. It usually occurs along the semilunar line. This defect creates the plane for inter parietal hernias, between the rectus and the oblique muscles. Spigelian hernias usually occur below the level of the umbilicus [1]. Until now, only 3 other reported cases, were seen above the level of umbilicus [15] and one case reported to present like abdominal wall abscess, but below the level of umbilicus [16]. Our patient presented with a Spigelian hernia seen above the level of umbilicus presenting as an abdominal wall abscess. The treatment for spigelian hernias is surgery as there is more chance for strangulation due to narrow fibrous neck. It can be done by mesh repair either by open or laparoscopic technique.
Conclusion
Though internal hernias are rare, in a previously non operated abdomen presenting as intestinal obstruction, especially when there is a history of similar episode subsiding by itself, we should have a differential diagnosis of internal hernia and we should always be cautious of cutting the obstructing band in internal hernias as it may hamper important vascular supplies. In a case of internal hernia; early intervention prevails better survival.
[1]. Norman S. Williams, Christopher J, Bulstrode K, O’Connell P. Ronan, Bailey and Love’s Short practice of Surgery 2013 26th EditionLondonTaylor & Francis Ltd:948-68. [Google Scholar]
[2]. Martin LC, Merkle EM, Thompson WM, Review of Internal Hernias: Radiographic and Clinical FindingsAJR 2006 186:703-17.10.2214/AJR.05.0644. Available from: http://www.ajronline.org/doi/abs/10.2214/AJR.05.0644 [Google Scholar]
[3]. Digestive diseases in the United States; epidemiology and impact. NIH publication no. 94-1447. BETHESDA: NIDDK, 1994. [Accessed on 30/09/2015] [Google Scholar]
[4]. Lassandro F, Iasiello F, Pizza NL, Valente T, Luisa M, di Santo Stefano M, Abdominal hernias: Radiological featuresWorld J Gastrointest Endosc 2011 3(6):110-17.PMCID: PMC3158902. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3158902 [Google Scholar]
[5]. Killedar MM, Maharaul HH, Left paraduodenal hernia: Case report and literature reviewInternational Journal of Biomedical Research. IJBR 2014 05(04):296-98.Available from: http://www.ssjournals.com/index.php/ijbr/article/view/1001 [Google Scholar]
[6]. Ghahremani GG, Abdominal and pelvic hernias. In: Gore RM, Levine MS, edsTextbook of gastrointestinal radiology 2000 2nd edPhiladelphia, PASaunders:1993-2009. [Google Scholar]
[7]. Martin LC, Merkle EM, Thompson WM, Review of internal hernias: radiographic and clinical findingsAJR Am J Roentgenol 2006 186(3):703-717.PMID:16498098 [Google Scholar]
[8]. Armstrong O, Internal hernias: anatomical basis and clinical relevanceSurg Radiol Anat 2007 29(4):333-37.PMID: 17487440 [Google Scholar]
[9]. Huang YM, Chou ASB, Wu YK, Wu CC, Lee MC, Chen HT, Left paraduodenal hernia presenting as recurrent small bowel ObstructionWorld J Gastroenterol 2005 11(41):6557-59.PMCID: PMC4355805 [Google Scholar]
[10]. Maya A, Cazeneuveb N, Bourbao-Tournoisc C, Acute small bowel obstruction due to internal herniation through the Foramen of Winslow: CT diagnosis and laparoscopic treatmentJournal of Visceral Surgery 2013 150:349-51.Available from: http://www.em-consulte.com/en/article/850784 [Google Scholar]
[11]. Bartlett MK, Wang C, Williams WH, The Surgical Management of Paraduodenal HerniaAnnals of Surgery 1968 168(2):249-54.Available from: http://journals.lww.com/annalsofsurgery/Citation/1968/08000/The_Surgical_Management_of_Paraduodenal_Hernia_.10.aspx [Google Scholar]
[12]. Katagiri H, Okumura K, Machi J, Internal hernia due to mesenteric defectJournal of Surgical Case Reports. JSCR 2013 5(3 pages)Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3813620/pdf/rjt037.pdf [Google Scholar]
[13]. Mittal T, Kumar V, Khullar R, Sharma A, Soni V, Baijal M, Diagnosis and management of Spigelian hernia: A review of literature and our experienceJ Minim Access Surg 2008 4:95-98.doi: 10.4103/0972-9941.45204. PMCID: PMC2699070 [Google Scholar]
[14]. Martell EG, Singh NN, Zagorski SM, Sawyer MAJ, Laparoscopic Repair of a Spigelian Hernia: A Case Report and Literature ReviewJSLS 2004 8(3):269-74.PMCID: PMC3016797 [Google Scholar]
[15]. Rehman JM, Seow CS, O’dwyer PJ, A case of a Spigelian hernia at an unusually high anatomical locationJR Coll Surg Edinb 2000 46:196-97.PMID: 10881490 [Google Scholar]
[16]. Malik SA, NazeerKawoosa NU, Zargar BR, Spigelian Hernia Presenting As Abdominal Wall AbscessIran Red Crescent Med J 2012 14(4):252-54.PMCID: PMC3385808 [Google Scholar]