Endometrial Cholesterol Granuloma Associated with Prolapsed Uterus- A Rare Case Report with Unusual Clinical Presentation
S. Sumathi1
1 Associate Professor, Department of Pathology, Melmaruvathur Adhiparasakthi Institute of Medical Science and Research Institute, Melmaruvathur, Kanchipuram, Tamilnadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. S. Sumathi, Associate Professor, Department of Pathology, Melmaruvathur Adhiparasakthi Institute of Medical Science and Research Institute, Melmaruvathur, Kanchipuram District, Tamilnadu-603319, India.
E-mail: mr.rathinamari@rediff mail.com
Cholesterol granuloma is a chronic inflammatory reaction to cholesterol deposition. It may develop in variety of sites including middle ear, mastoid process, para nasal sinuses, mediastinum, breast, testis and kidney. But endometrial cholesterol granuloma is a rarely reported case and is usually presented clinically as pyometra. This article reports a case of cholesterol granuloma in the endometrium associated with prolapsed uterus. In this case the patient clinically presented with urinary retention and overflow incontinence of urine. The reason of acute urinary retention in this case was pelvic fibrosis and adhesion secondary to this chronic inflammatory reaction. This was supported by the presence of pus like yellowish material over the uterine surface and pelvic adhesion, noted during surgery. Endometrial biopsy revealed cholesterol granuloma that confirmed the source of chronic inflammatory reaction and pelvic fibrosis.
Endometrium, Pyometra, Urinary retention
Case Report
A 65-year-old lady presented to the gynecology department with complaints of dribbling of urine and constipation for two days. General examination revealed mild pale conjunctiva. Abdominal examination revealed distended bladder upto the umbilicus. Vaginal examination indicated bulky uterus with second degree uterovaginal prolapse, minimal rectocele and cystocele. Clinical diagnosis of prolapsed uterus with acute urinary retention was made. Laboratory investigation indicated that her haemoglobin level was 10.7g%, WBC count 17,300cells/cmm with 85% neutrophils and blood sugar level was 103mg%. Pelvic scan revealed enlarged uterus and distended uterine cavity with large collections. PAP smear showed inflammatory changes and there was no evidence of cervical intra epithelial lesion. Endometrial curettage and cervical biopsy was taken with the clinical suspicion of associated pyometra. Histopathological examination showed only haemorrhagic necrotic material in the endometrial sample [Table/Fig-1] and chronic cervicitis features. Abdominal hysterectomy was planned to rule out occult malignancy. During surgery the surgeon noticed pus like discharge from the uterus while holding it with forceps. Posterior wall of uterus, left sided ovary, tube were adherent with the sigmoid colon also. Adhesion was released. Total hysterectomy was done and sent for histopathological examination. Grossly, the uterus was slightly enlarged with dilated endometrial cavity. Endometrial thickness was only 2mm and yellowish brown haemorrhagic material was attached to the endometrial cavity wall [Table/Fig-2]. Microscopic examination showed total destruction of endometrial glands and stroma. Endometrium was entirely replaced by many aggregates of longitudinal clefts of cholesterol crystals surrounded by lymphocytes, foamy histiocytes, neutrophils and many multinucleated giant cells [Table/Fig-3,4]. This granulamatous inflammation was extended into the adjacent myometrium also [Table/Fig-5]. Histological examination of cervix showed benign mucosal epithelium and inflamed stroma [Table/Fig-6]. The final diagnosis of endometrial cholesterol granuloma with chronic cervicitis was made.
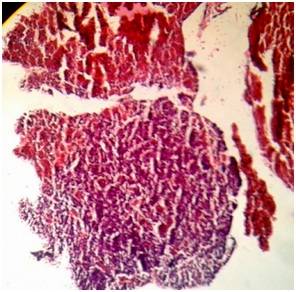
Photomicrograph of endometrial curetting showing haemorrhagic necrotic material. (H&E x 50).
Gross photograph of uterus cervix with dilated endometrial cavity containing yellowish haemorrhagic material.

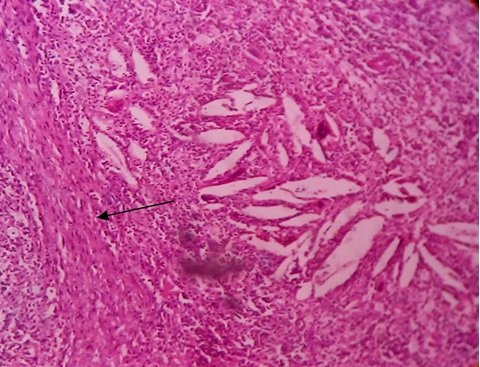
Photomicrograph of endometrium showing cholesterol granuloma (Long arrow) & Intact endometrial gland (Short arrow). (H&E x 100).

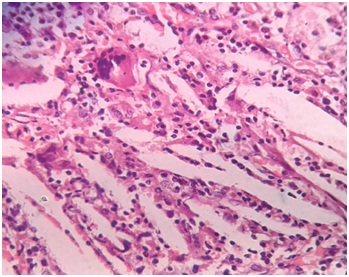
Photomicrograph shows cholesterol clefts, inflammatory cells & foreign body giant cells. (H&E x 400).
Photomicrograph shows myometrial extension of cholesterol granuloma (H&E x 100). Arrow points out smooth muscle tissue.
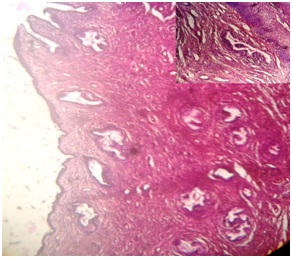
Photomicrograph showing benign endocervical mucosa & glands. (H&E x 50). Inset shows benign squamous lining of cervix. (H&E x 100).
The patient was so far followed up twice after surgery and she was free of symptoms.
Discussion
Cholesterol granuloma was first described in 1917 by Manase. It results from a foreign body reaction to cholesterol crystals deposition. The source of cholesterol is the anaerobic breakdown of blood products. So trauma with haemorrhage has been put forward as the initiating event in cholesterol granuloma formation [1].
One study showed that Perlecan (a basement membrane heparin sulfate proteoglycan) which is present abundantly in the wall of immature granulation tissue might be related to the development of cholesterol granuloma [2,3]. It may also be formed in mucous, pus or necrotic tissue [4]. Hyperlipidaemia, cholesterol emboli and impaired drainage may also play a role in these lesions [5].
The exact etiopathogenesis of cholesterol granuloma is not clear. However, in our case the presence of neutrophilic leukocytosis, dilated endometrial cavity with yellowish brown haemorrhagic collections, peroperative pus like yellowish discharge from the uterus, presence of haemorrhagic necrotic material in the endometrial curetting sample favours the possibility of breakdown of blood products and necrosis as the initiative factor for cholesterol granuloma formation. Red cells membrane damage leads to accumulation of lipids that triggers immune inflammatory reaction. Granulamatous inflammation of endometrium was also reported in endometrial tuberculosis, immune mediated ceroid histiocytic granuloma and also as idiopathic origin [6–8].
Studies showed that it commonly occurs in middle aged patients (mean age= 38-year-old; age range from 27 to 56 years) with male gender predilection [9]. In our case it is found in elderly post menopausal women. It is found commonly in head and neck region and few cases are reported in organs like breast, kidney, anterior mediastinum, ovary [1,5,10,11]. Endometrial cholesterol granuloma is a rare entity and represents a rare morphologic variant of benign senile pyometra [12].
To the best of our knowledge the case reported by Pounder DJ is the only case of endometrial cholesterol granuloma clinically presented as pyometra which later turned out to be an endometrial adenosquamous carcinoma [12]. It remains silent clinically for long time or presented with mass lesion, compressive symptoms depending upon the size and location. One study showed incidental lipogranuloma of cervix in post menopausal woman with prolapsed uterus [13]. In our case it was associated with prolapsed uterus but clinically presented with symptoms of obstruction like constipation and urinary retention. These obstructive symptoms are not due to endometrial cholesterol granuloma as such as in other places like middle ear. The extension of chronic granulamatous inflammation into the entire uterine wall, presence of pelvic adhesion, fibrosis explains the reason for the obstructive symptoms of urinary retention and constipation.
Conclusion
This case is reported because of its rarity of site and its association with prolapsed uterus. It can be presented as acute urological symptoms of urinary retention secondary to pelvic adhesion and clinically mimicks pyometra with occult malignancy. Histopathological evaluation is essential to rule out this benign entity.
[1]. Fatima Twisted ovarian tumor with cholesterol granuloma. An unusual morphological entity with review of literatureSch J Med case rep 2014 2(3):179-82. [Google Scholar]
[2]. Yamazaki M, Cheng J, Hao N, Takagi R, Jimi S, Itabe H, Basement membrane type heparin sulfate proteoglycan (perlecan) and low density lipoprotein (LDL) are co-localized in granulation tissues: a possible pathogenesis of cholesterol granuloma in jaw cystsJ Oral Pathol Med 2004 33:177-84. [Google Scholar]
[3]. Lee JH, Alrashden MS, Ahn KM, Kang MH, Hong SP, KIM SM, Cholesterol granuloma in the wall of a mandibular dentigerous cyst: a rare case reportJ Clin Exp Dent 2010 2(2):e88-90. [Google Scholar]
[4]. Surala U, Otitis media adhesiveArchives of otolaryngology 1964 80:287 [Google Scholar]
[5]. Ezzat TF, Alowami S, Cholesterol granuloma of the anterior mediastinum with osseous metaplasiaRare tumour 2012 4:e47 [Google Scholar]
[6]. Shintaku M, Sasaki M, Baba Y, Ceroid containing histiocytic granuloma of the endometriumHistopathology 1991 18(2):169-72. [Google Scholar]
[7]. Patacchiola F, Genital tuberculosis in menopausal women. A case reportMinerva Gynecol 2002 54(3):287-91. [Google Scholar]
[8]. Paul kelly-W, Gienn Mc Cluggage, Idiopathic uterine granuloma; Report of a series of morphological similiarities to idiopathic ovarian cortical granulomasInternational journal of gynecological pathology. 08 2006 25(3):243-46. [Google Scholar]
[9]. Chao TK, Cholesterol granuloma of the maxillary sinusEur Arch Otorhinolaryngol 2006 263:592-97. [Google Scholar]
[10]. Osada T, Kitayama J, Nagawa H, Cholesterol granuloma of the breast mimicking carcinoma: report of a caseSurg Today 2002 32(11):981-84. [Google Scholar]
[11]. Krishnan TR, Sinha SK, Kajriwal NK, A rare case of cholesterol granuloma in the anterior mediastinumHeart Lung circ 2013 22(4):303-04. [Google Scholar]
[12]. Pounder DJ, Iyer PV, Benign senile pyometra, endometrial cholesterol granulomas and adenosquamous carcinomaThe Australian & New Zealand journal of obstetrics & gynecology 1985 25(2):139-41. [Google Scholar]
[13]. Akbulut M, Utku Y, Soysal S, Lipogranuloma of the cervix in a postmenopausal patient with a uterine prolapseArch Gynecol obstet 2008 277(3):277-79. [Google Scholar]