Urinary Incontinence (UI) has considerable social and economic impact on the individuals and society. The International Continence Society (ICS) has defined the symptoms of UI as “Involuntary loss of urine that is a social or hygienic problem’ [1]. Women have a higher risk of developing incontinence in their lifetime compared with males. Ageing is associated with many physiologic changes that may lead to UI. Pregnancy, childbirth and physical straining during labour together with lacerations and episiotomies during delivery have been found to increase the incidence of incontinence. Menopause also worsens this condition [2].
UI is a socially distressing problem with a high degree of discomfort and though it severely impacts the quality of life in women. Women do not usually discuss the problems with others or during visit to a doctor for treatment and are the typical ‘silent sufferers’ of the problem. The percentages of people who suffer from UI and seek treatment are few, demonstrating the ‘tip of ice berg phenomenon’. The actual severity of leakage ranges from loss of drops of urine to complete bladder emptying. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) have funded the UI Treatment Network (UITN) to undertake epidemiological and clinical trial studies on various aspects of UI [3]. Few studies in India evaluated the risk factors and the significance of their association with UI, which reflected a lack of awareness of the condition among the study population [4–6].
Increasing age, multiparty, forceps delivery, chronic cough, constipation and history of UTI were found to have significant association with UI, and thus these conditions were termed as ‘risk factors’ [1]. A study by Gerwen et al., identified the comorbidities that are more common in patients with UI compared with patients without this diagnosis [8]. In women, diabetes mellitus, genitourinary prolapse and chronic obstructive pulmonary disease (COPD)/asthma, constipation, obesity, were all recognised as co-morbidities [8]. Of all the co-morbidities the prevalence rate for UTI was the highest.
This study aimed at determining the association of a single risk factor - UTI among UI patients, to analyse the causative organism and their susceptibility patterns.
Materials and Methods
This was cross-sectional, non-randomized study conducted in a hospital based population after obtaining necessary Ethical Committee clearance from the institutional scientific review board. The study was conducted for a period of one year, from June 2012 to May 2013. The Departments of Microbiology, Obstetrics & Gynaecology, Urology, Medicine and Surgery were involved in the study. Patients included were parous or nulliparous married women attending the hospital OPD. Unmarried women and patients with anatomical genital tract pathology like prolapse uterus were excluded.
This study was based on history and clinical examination of patients. The purpose of the study was explained and informed consent was obtained from all respondents. Patients who were not willing to participate in the study were excluded. Privacy and confidentiality were ensured and maintained during the whole process; patients were motivated to come for follow ups for further management. The sample size of 107 was calculated by taking into consideration the previous 10% prevalence [4] of UTI in women presenting with UI.
A semi-structured questionnaire was designed by the subject experts who include gross-sections like demographic details, history of incontinence, obstetric history, past medical and surgical history. It was provided to the patients who came under the study group and we explained the questionnaire in their own language and recorded the responses.
The patient’s urinary complain and its duration, parity, mode and place of delivery were noted. History of constipation, previous pelvic surgeries and history of previous episodes of UTI and treatment for the same was also recorded. Midstream urine sample was collected in a sterile container after giving proper instructions to those married women with positive history of incontinence. All the samples were transported to the microbiology laboratory and processed.
Screening of urine for significant bacteriuria was done by Gram staining the samples. Urine culture was done by a semi-quantitative technique. Urine (0.001ml) was cultured by using a calibrated bacteriological loop on Blood agar and MacConkey’s agar. After an overnight incubation at 37°C, number of colonies which were counted and they were multiplied by 1000, to obtain the colony forming units (cfu)/ml. Presence of 105 bacteria/ml of urine indicated significant bacteriuria.
Isolates were identified by Gram staining, motility tests and standard biochemical reactions [10]. Antibiotic sensitivity was performed by using Kirby Bauer disc diffusion method following the Clinical Laboratory Standards Institute (CLSI) guidelines [11].
Results
All patients attending the hospital OPD were approached with a questionnaire and the 107 patients with positive history of incontinence were selected. Incontinence was noted in patients with minimum age of 27 to a maximum age of 80. Majority of the patients (62.6%) fell into the 41-60 category of age group. Almost 64.5% of the patients came under lower class of socioeconomic status, calculated using educational status, occupation and annual income (Kuppuswamy scale) [12]. The distribution of various types of UI according to the age groups is shown in [Table/Fig-1].
Type of urinary incontinence and its prevalence in the age group.
| Age group | Stress/Urge/Mixed | Total |
|---|
| Stress Incontinence | UrgeIncontinence | Mixed Incontinence |
|---|
| <40 yearsCount % of total | 1110.3% | 54.7% | 109.3% | 2624.3% |
| 41-60 yearsCount % of total | 1615.0% | 1816.8% | 3330.8% | 6762.6% |
| >60 yearsCount % of total | 00% | 1211.2% | 21.9% | 1413.1% |
| TotalCount % of total | 2725.2% | 3532.7% | 4542.1% | 107100.0 |
It was noticed that mixed incontinence was the most common type (42.1%) followed by urge incontinence (32.7%) and stress incontinence (25.2%). Younger age group (<40) had predominantly stress incontinence, 40-60 had mixed incontinence and older age group (>60) had predominantly urge incontinence. This association was calculated using chi-square analysis with p<0.000. Around 57% had a problem of daily urinary leak and a leak of 5-10 times/month was also seen to be common among 30.8%.
Among the study group, 92% did not seek medical advice for their condition and 81.3% complained that the UI affected their daily activities. None of the patients with positive history of UI were aware or taught of any perineal exercises during their antenatal or postnatal period. Almost 90% of patients with incontinence had normal vaginal delivery. The percentage for the presence and absence of co-morbid conditions associated with UI is shown in [Table/Fig-2].
Percentage of Co-Morbid conditions associated with Urinary Incontinence.
| S.No | Question. | Percentage |
|---|
| 1. | Chronic constipation | 42.1% |
| 2. | History of pelvic surgeries | 32.7% |
| 3. | Chronic cough | 17.8% |
Overall 25.2% (27 out of 107) of patients with incontinence had a positive urine culture, 74.8% (80 out of 107) of patients had negative urine culture. Association of positive culture in patients with history of UTI is shown in [Table/Fig-3]. The association was calculated using chi-square analysis with p <0.010. The distribution of the organisms causing UTI in UI patients is shown in [Table/Fig-4].
Association of Positive urine culture in patients with History of Urinary Tract Infection.
| History of Urinary Tract Infection | Urine Culture | Total |
|---|
| Yes | NO |
|---|
| Yes | Count | 16 | 25 | 41 |
| % of total | 15.0% | 23.3% | 38.3% |
| No | Count | 11 | 55 | 66 |
| % of total | 10.3% | 51.4% | 61.7% |
| Total | Count | 27 | 80 | 107 |
| % of total | 25.2% | 74.8% | 100.0% |
Distribution of organisms causing Urinary Tract Infections.
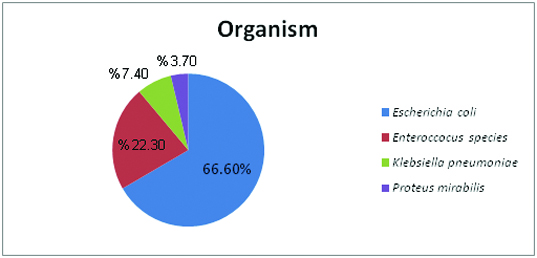
Antimicrobial susceptibility patterns for Escherichia coli showed a high sensitivity to Nitrofurantoin (94.4%) and 66.6% to Amikacin. The susceptibility patterns to other antibiotic were as follows: Imipenem (38.8%), Piperacillin-tazobactum (55.5%), Cefaperazone-Sulbactum (38.8%), Gentamicin (38.8%), Cefexime (16.6%), Norfloxacin (16.6%) and Cotrimaxzole (11.1%).
The next predominant organism was Enterococcus species which showed 100% sensitivity to Vancomycin and 93% to Ampicillin and maximum resistance to Erythromycin (97%). Other isolates such as Proteus mirabilis and Klebsiella pneumoniae were sensitive to all the commonly used drugs.
Discussion
UI, a socially distressing condition, is a significant health problem in the community. It typically leads to embarrassment, curtailment of daily, social and sexual activities and is a considerable economic burden on the individual as well as the healthcare system.
In the present study the prevalence of incontinence was seen increasing with age, 24.3% in women less than 40, and 62.6% in women between 41 and 60. This was in accordance with the study conducted by Bodhare TN et al., The increasing UI with advancing age can be explained by loss of muscle tone, decreased contractility, changes in the hormonal stimulation and repeated injuries during parturition [4].
Almost 64.5% of the patients came under lower class of socioeconomic status. A study conducted by Shilpi et al., in central India quoted Lower Urinary Tract Symptoms (LUTS) is commonly found in females of low socio-economic status [6]. LUTS refers to all Lower Urinary Tract Symptoms which includes, stress, urge, mixed incontinence, nocturnal enuresis, irritation, urgency, etc [1].
Our study showed that almost 92% of the patient did not consult a doctor even though they had symptoms. This is because most of the women of our country accept UI to be a ‘part of ageing’ and they believe that nothing can be done about it. The high prevalence rates for the condition can be accounted due to the lack of awareness among the patients that UI is globally recognised condition with sufficient treatment facilities [5].
Identification of risk factors and altering them with appropriate measures can reduce the burden of UI. Childbirth is identified as one of the risk factors of UI; the labor, delivery process, spontaneous lacerations and episiotomies may cause nerve damage and muscular damage resulting in pelvic floor dysfunction [4,7]. More than 60% of the incontinent women had borne more than two children in their obstetrical career in the current study.
There was a high prevalence of chronic constipation (42%) among the incontinent females in our study; similar results were noted by another study [4] with significant association between constipation and incontinence in regression analysis (Nagelkerke R2 = 0.7). Increased abdominal pressure during constipation could be the possible explanation given for UI [13].
The prevalence of stress incontinence was 25.2% and it was present mostly in younger age groups (<40), urge incontinence was 32.7% which was more prevalent in the older groups (>60) and mixed incontinence showed the highest prevalence of 42.1%. Almost similar observation was determined by a study [2] done in South India where the urge incontinence was found to be more when compared to stress incontinence [4]. But according to other studies; stress incontinence was more common than urge incontinence [14,15], and the overall prevalence of urinary incontinence (stress, urge and mixed) among women in rural and urban India varies between 10% and 58.8% [2,4,6,16].
One of the risk factor for incontinence is UTI. Studies in India, Dutch and Washington also proved UTI was one of the important co-morbid conditions causing UI [4,8,17]. The association of UTI in incontinent patients was 25.2% in our study, whereas higher percentage (45%) of patients was noted by a study done by Bergman A et al., [9]. They emphasized the need for correction of UTI by appropriate therapy as it regained bladder stability in about 60% of patients with UI.
In our study, Escherichia coli was found to be the most common organism causing the UTI in incontinent patients. Even though there was insufficient data on the common causative organism causing UTI in patients with UI; it was well known that Escherichia coli is the predominant organism isolated in all urinary tract infections. The antibiotic susceptibility for Escherichia coli revealed it to be highly sensitive for Nitrofurantoin (94.4%) and highly resistant to Ampicillin (94.4%). The next common organism is Enterococcus species which showed maximum sensitivity to Ampicillin and Vancomycin and resistance to Erythromycin.
UTI causes irritation of the bladder which initially presents as urgency; repetitive episodes of UTI can lead to weakening of the bladder wall and loss of contractility of the sphincters. This cumulatively leads to UI. UI causes stasis of urine in the bladder and can in turn lead to UTI. So, a vicious cycle sets in and can lead to worsening of both the conditions [8]. Hence, definite treatment of UI should not be undertaken before successful treatment of UTI after proper urine culture and sensitivity [9]. Our study statistically showed a significant proportion of incontinent patients (25.2%) had UTI. The literature shows that an appropriate correction of the existing UTI can help in the treatment of UI [1,9,18]. Hence, we suggest that the appropriate diagnosis and treatment of UTI could be a non-surgical approach for the treatment of Urinary Incontinence.
Limitation
However, the limitation is that we have studied the association of single risk factor with UI, while the association of other co-morbidities needs to be established in the given population.
Conclusion
Our study revealed that one in every four patients with incontinence had Urinary Tract Infection (UTI) and almost half of them suffered from previous episodes of UTI. Most of the patients were not aware of UI as a recognised disease. Moreover only 8% of the population had sought medical opinion for their condition, which shows that the awareness among the patient about the treatment facilities is low. We suggest periodic surveillance of the condition and epidemiological studies could lead to spread of awareness about the condition.