Intestinal Volvulus: A Life-Threatening Disease
Mohammed Y Hasosah1, Wael I Meer2, Khalid Alsaleem3
1 Assistant Professor, Department of Pediatric Gastroenterology, King Saud Bin Abdulaziz University for Health Sciences, National Guard Hospital, Jeddah, Saudi Arabia.
2 Pediatric Resident, Department of Pediatric, Dr Suliman Faqeeh Hospital, Jeddah, Saudi Arabia.
3 Pediatric Consultant, Department of Pediatric Gastroenterology, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mohammed Y Hasosah, Department of Pediatric Gastroenterology, Assistant Professor of Pediatric, King Saud Bin Abdulaziz University for Health Sciences/Pediatric Consultant Gastroenterologist, King Abdul-Aziz Medical City, National Guard Hospital, Jeddah, PO Box: 8202, Jeddah 21482.
E-mail: hasosah2007@yahoo.com
Ladd’s procedure, Malrotation, Midgut
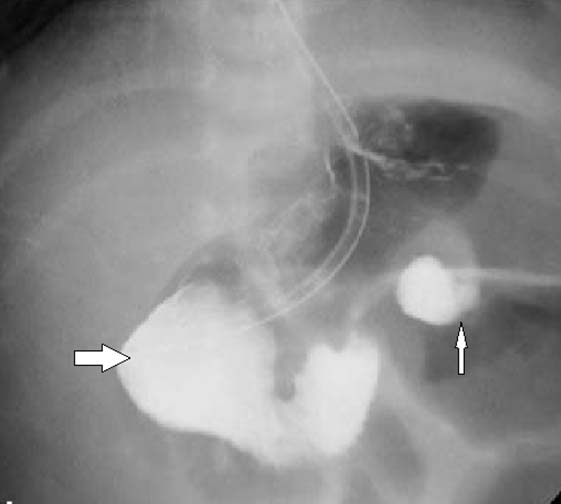
A male infant was delivered at 40th week gestational age with a birth weight of 3.2 kilogram via cesarean section to a 29-year-old primiparous woman. The mother had normal antenatal care. The infant was admitted into neonatal intensive care unit with bilious vomiting and rectal bleeding at the age of 4 days. Physical examination revealed sick baby. He is tachycardiac (Heart rate: 170) and hypotensive (Blood pressure 45/20). There is abdominal distension, otherwise systemic examinations were normal. The baby was rapidly resuscitated with normal saline and intravenous antibiotics were started. Blood transfusion was given because hemoglobin dropped to 6.1 (normal value: 12. 2-15.3 gm/dL). An Upper Gastrointestinal Barium Swallow showed dilated duodenum (bold arrow) and “Corkscrew” of contrast projecting away from the posterior abdominal wall suspecting malrotation with midgut volvulus (narrow arrow) [Table/Fig-1].
An Upper Gastrointestinal Barium Swallow showing dilated duodenum (bold arrow) and “Corkscrew” of contrast projecting away from the posterior abdominal wall suspecting malrotation with midgut volvulus (narrow arrow).
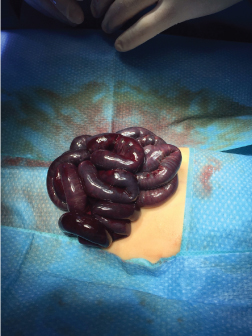
An emergency laparotomy was performed, which confirmed twisting of superior mesenteric artery. Volvulus occurred at the duodenojejunal junction. There was 360 degree rotation of volvulus. The diagnosis of small-bowel volvulus was confirmed and Ladd’ procedure was performed [Table/Fig-2]. The bowel was not resected because of intestinal viability and no necrotic tissues in the second-look operation at 24 hours.
Twisting of superior mesenteric artery on laparotomy.
During fetal development the intestinal volvulus is twisted because of malrotation of the intestine [1]. When the normal embryologic sequence of bowel development and fixation is interrupted, malrotation of the intestine occurs [1]. The pathogenesis of volvulus occurs because the narrow mesenteric base, which develops as a result of malrotation, allows the small bowel to twist around the superior mesenteric artery. This leads to vascular compromise of large portions of the midgut [1]. In neonates, malrotation with midgut volvulus classically presents with bilious vomiting and intestinal obstruction. Abdominal tenderness and hemodynamic deterioration (hematemesis, hematochezia and shock) are associated symptoms [2]. If the volvulus is missed, it can lead to vascular compromise, which can cause intraluminal bleeding evidenced by melena and/or hematemesis and worsening intestinal ischemia can lead to signs of shock [2].
The best diagnostic choice to diagnose malrotation, with or without midgut volvulus, is an upper GI series. The Ladd procedure remains the cornerstone of surgical treatment for malrotation [3]. Ladd procedure is described as reduction of volvulus (if present), division of mesenteric bands, placement of small bowel on the right and large bowel on the left of the abdomen. When intestinal malrotation is complicated by volvulus especially if the child has signs of systemic decompensation (hematochezia, abdominal distension, peritonitis and shock), it is a potentially life-threatening condition and requires emergent evaluation and treatment. The child should be rapidly resuscitated and immediately taken to surgery for exploration because quick surgical intervention, not prolonged medical management, is associated with the best results if midgut volvulus is suspected [3].
[1]. Fonkalsrud E, Rotational anomalies and volvulusIn: Principles of Pediatric Surgery, O’Neill JA et al. (Ed) 2003 St. LouisMosby:477 [Google Scholar]
[2]. Shalaby MS, Kuti K, Walker G, Intestinal malrotation and volvulus in infants and childrenBMJ 2013 347:f6949 [Google Scholar]
[3]. Millar AJ, Rode H, Cywes S, Malrotation and volvulus in infancy and childhoodSemin Pediatr Surg 2003 12:229 [Google Scholar]