Chemotherapy, Neoplasm, Surgery
Wilms’ tumour is a rare neoplasm of kidney in adults. They are advanced and have poorer prognosis than those in children. Though controversial, aggressive multimodality therapy is recommended. We report a case of Wilms’ tumour in an adult female who was treated with radical nephrectomy and is under three-drug chemotherapy at present.
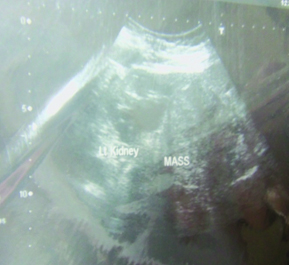
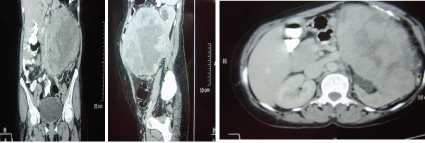
A 48-year-old female was admitted with history of left-sided flank mass since 1 year which was gradually increasing in size. There was history of left flank pain since 7 days. There was no history of haematuria or co-morbid illness. Complete haemogram, coagulation profile, renal and liver function tests were normal. An abdominal ultrasound revealed a large well-defined mass of size 17x14.3cm arising from lower pole of left kidney with mild vascularity [Table/Fig-1]. Computed Tomography (CT scan) suggested a 15.3x15.8 cm heterogeneously enhancing solid lesion arising from lower pole of the left kidney with multiple non enhancing areas and displacing major vessels [Table/Fig-2a-c]. The left renal vein was free. The right kidney was normal in both the imaging investigations. Radical nephrectomy was done [Table/Fig-3,4]. Histopathology revealed adult onset Wilms’ tumour. She was started on three-drug chemotherapy regimen and is currently undergoing chemotherapy.
USG Image showing Left Kidney and a large well-defined mass of size 17x14.3cm arising from lower pole of left kidney with mild vascularity.
Computed Tomography (CT scan) showing a 15.3x15.8 cm heterogeneously enhancing solid lesion arising from lower pole of the left kidney with multiple non-enhancing areas and displacing major vessels. The left renal vein was free. The right kidney was normal.
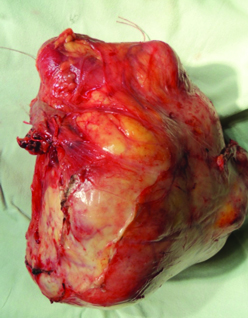
Excised specimen of Left Kidney showing a large lobulated mass arising from lower pole. The Hilum and Upper Pole are free.
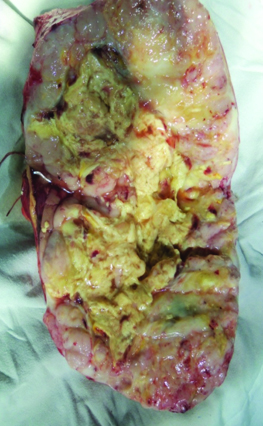
Cut-section of the excised specimen of left kidney showing the tumour invading and distorting the pelvicalyceal system.
Wilms’ tumour is the most common primary malignant renal tumour in the paediatric age group [1]. Most cases of paediatric Wilms’ tumour present between the ages of 12 months to 48 months [1]. It is a malignant embryonic renal neoplasm arising from metanephric blastema which is rare in adults [2]. Although rare, the exact number of adult cases of Wilms’ tumour cannot be commented because of under-reporting. The incidence in Europe and USA has been estimated to be 0.2 per million per year [3]. Only around 300 cases of adult Wilms’ tumour have been reported in the literature [3].
Adults usually present with pain and haematuria, whereas children present with an incidentally detected abdominal lump. Distant metastases occur in lungs, liver, bones, skin, bladder, bowel, central nervous system and opposite kidney [3]. Staging criteria are based on the anatomic extent of the tumour. Management is based on National Wilms’ Tumour Study Group (NWTS)/ Children’s Oncology group (COG) and Society of Paediatric Oncology (SIOP) protocols. NWTS/COG protocol recommends upfront surgery followed by chemotherapy whereas SIOP recommends chemotherapy before surgery. Histology is the same in tumours occurring both in the child and adult. The prognosis is poorer in Wilms’ tumour in adults, probably because of advanced stage at diagnosis [2].
In 1980, Kilton et al., has laid down the following criteria for diagnosis of adult Wilms’ tumour [4]:
It should be a primary neoplasm
There should be presence of primitive blastematous spindle or round cell component
Formation of abortive or embryonal tubular or glomeruloid structures is necessary
No area of the tumour should show features of renal cell carcinoma
Pictoral confirmation of histology is required
Age should be more than 15 years.
Pre-operative diagnosis is difficult [2]. Abdominal CT scan shows a large, well-defined, exophytic, inhomogeneous mass which is cortical in origin [5]. There may be large areas of low density present along with areas of focal necrosis and haemorrhage on non-contrast images [5].
There is controversy regarding management plans, though multimodality therapy is accepted [2]. Radical nephrectomy is the preferred mode of management in most of the cases. Those tumours which are initially inoperable are given chemotherapy followed by surgery after which the chemotherapy is continued. Prognosis is poorer in adults.
[1]. Ehrlich Peter F, Shamberger Robert C, Wilms’ Tumour in: O’Neil JA Jr, Rowe MI, Grosfeld JL, Fonkalsrud EW, Coran AG, editorsPediatric Surgery 1998 5th edNew York, USAMosby:423-440. [Google Scholar]
[2]. Sharma MS, Ahmed MZ, Adult Wilms’ tumourSaudi J Kidney Dis Transpl 2009 20(5):835-37. [Google Scholar]
[3]. Guo A, Wei L, Song X, Liu A, Adult Wilms’ tumour with intracaval and intracardiac extension: Report of a case and review of literatureJ of Cancer 2011 2:132-35. [Google Scholar]
[4]. Kilton L, Mathews MJ, Cohen MH, Adult Wilms’ tumour: a report of prolonged survival and review of literatureJ Urol 1980 124:1-5. [Google Scholar]
[5]. Krishnan J, Pietras J, Nachmann M, Brown G, Adult Wilms’ tumour with a unique presentation of high-grade fever, photophobia and headacheRev Urol 2012 14(1/2):31-4.doi: 10.3909/riu0541 [Google Scholar]