Right Sided Sigmoid Colon and Redundant Loop of Descending Colon with Its Embryological Correlation and Clinical Significance
Pooja Bhadoria1, Shahid Bahksh2, Shilpi Agarwal3, Babita Pangtey4, Smita Kakar5
1 Senior Resident, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
2 PG Resident, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
3 Senior Resident, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
4 Assistant Professor, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
5 Professor, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pooja Bhadoria, Senior Resident, Department of Anatomy, Maulana Azad Medical College, Bahadur Shah Zafar Marg, New Delhi-110002, India.
E-mail: dr.poojabhadoria@gmail.com
Anatomical variations of colon are mostly developmental and can lead to variety of acute and chronic pathological conditions. So it becomes important to recognize and understand the importance of clinical implications of such anomalies to benefit surgeons, clinical geneticists and research community. We describe two cases of right sided sigmoid colon and long descending colon which had two segments: vertical and horizontal. The mesentery of ascending and descending colon was retained. This mesentery along with the mesentery of transverse colon was continuous with the mesentery of small intestine. There were variations in blood vessels supplying these anomalous colons. The findings of this study may be helpful to make surgeons and radiologists aware about different varieties of presentations while undertaking an investigative or surgical procedure in this area like sigmoidoscopy, percutaneous cecostomy and anterior transperitoneal aproach of kidney to avoid colon puncture.
Case Report
As a part of routine dissection, we found right sided sigmoid colon with redundant loop of colon in two cadavers of age ranging from 40-65 years in the anatomy department. As per the instructions given in Cunningham’s manual of practical anatomy [1] the midline incision was given extending from xiphoid process to the pubic symphysis to explore the peritoneal cavity without any damage to the peritoneum and structures covered by it. After exposing the abdominal cavity and removing peritoneal fat, the viscera were carefully separated and cleared from the field of view. In situ placement of small and large intestines and their peritoneal relations were studied in detail. The small intestine and its mesentery was reflected to the right, to study extent and location of parts of colon along with their peritoneal relations. The blood vessels supplying the small and large intestine were carefully dissected and studied.
The right sided sigmoid colon and long loop of descending colon was observed in two cadavers. The mesentery of ascending and descending colon was retained. This mesentery along with the mesentery of transverse colon was continuous with the mesentery of small intestine [Table/Fig-1,2]. In case one, the vertical segment of descending colon extended upto L4-L5 vertebral level and the horizontal segment crossed in front of the left gonadal vessels, left genitofemoral nerve, left ureter, abdominal aorta, common iliac vessels and superior rectal artery, right ureter, right genitofemoral nerve and right gonadal vessels [Table/Fig-3] to reach to right lumbar region and at this point it ascended one vertebral level higher and then turned downwards to become sigmoid colon at the right pelvic brim. The sigmoid colon occupied right iliac fossa and caecum was in the right lumbar region. The right limb of mesentery of sigmoid colon was attached to the right pelvic wall and left limb extended from right pelvic brim to third sacral vertebra. The inferior mesenteric artery turned towards right side so as to supply the right sided sigmoid colon. The left colic branch of inferior mesenteric artery divided into, left colic1 and left colic2, to supply the long segment of descending colon. The left colic1 divided into ascending and descending branch. The descending branch ended by anastomosing with the left colic2. The ascending branch ended by anastomosing with the left branch of middle colic [Table/Fig-3,4].
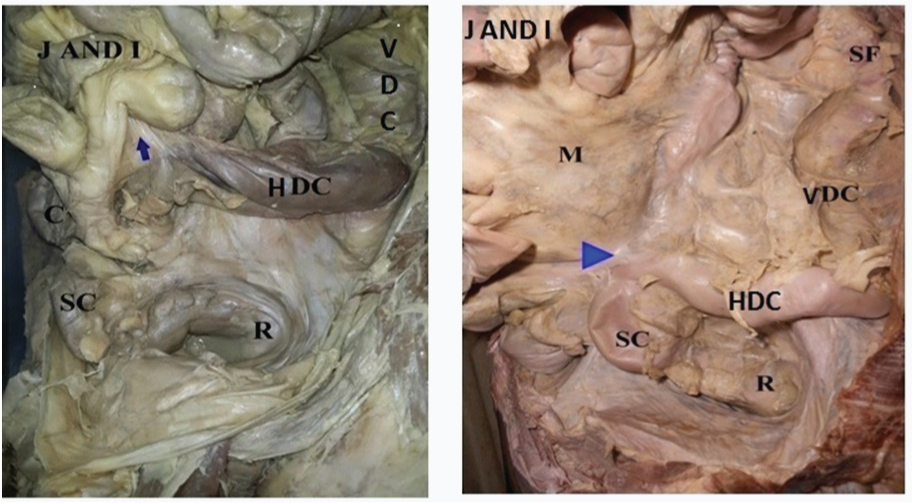
In both the photographs (case 1&2), the jejunal and ileal loops (J AND I) are reflected upwards and towards right to show the two segments of long descending colon: vertical(VDC) and horizontal(HDC) segment. The mesentery of long descending colon is retained and is continuous with the mesentery of small intestine(M). C: caecum, S.F: splenic flexure, S.C:sigmoid colon and R: rectum.
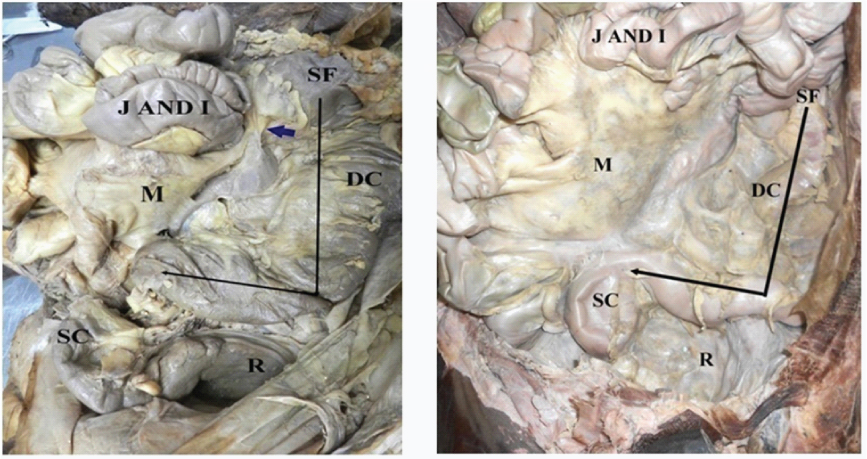
Photograph showing the long loop of descending colon(DC) and the position of sigmoid colon(SC). In first case sigmoid colon occupied right iliac fossa while in second case it reached 3.5 cm from right of midline to lie opposite L5 to S3 vertebrae. J AND I: jejunal and ileal loops, M: mesentery of small intestine, S.F: splenic flexure, and R:rectum.
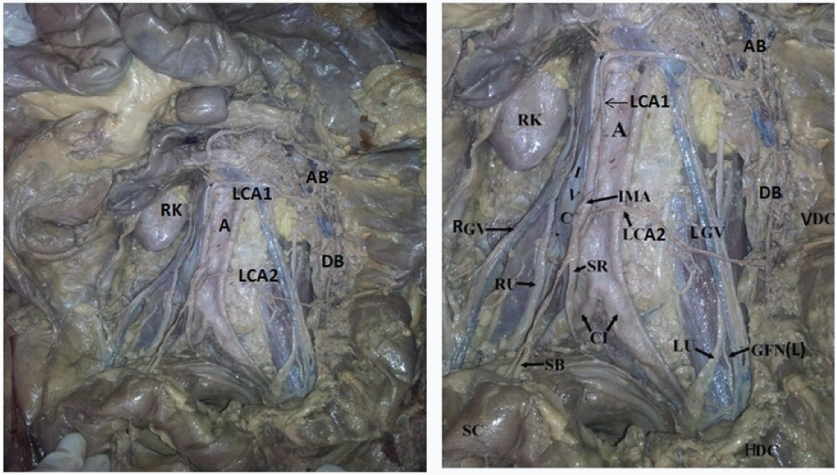
Photograph taken after retraction of the horizontal segment of descending colon (HDC) showing the structures crossed by this segment while traversing towards right i.e. LGV: left gonadal vessels, GFN :left genitofemoral nerve, LU: left ureter, A: aorta, IVC: inferior vena cava, CI :common iliac vessels, SR: superior rectal artery and SB: sigmoidal branches. RGV: gonadal vessels, RU: right ureter, RK: right kidney, IMA: inferior mesenteric artery and VDC: vertical segment of descending colon.
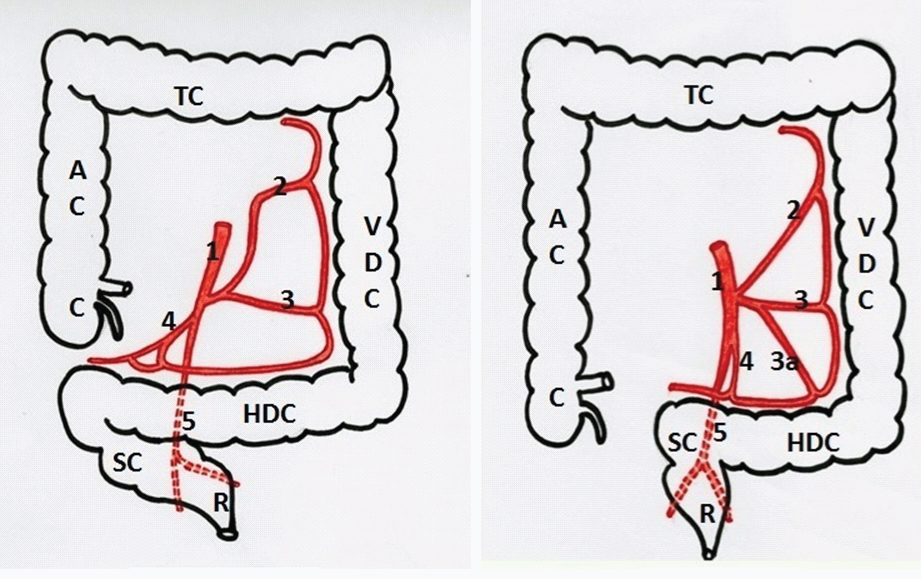
Schematic diagram to show the orientation of long descending colon and right sided sigmoid colon along with the anomalous branching pattern of inferior mesenteric artery supplying this long colon (case 1&2). 1: Inferior mesenteric artery divided into 2: left colic1 (LCA1) and 3: left colic2 (LCA2), 3a: left colic3 (LCA3), 4: sigmoidal branches, 5: superior rectal artery.
In case two, the vertical segment of descending colon extended upto L4-L5 vertebral level and the horizontal segment of descending colon reached 3.5 cm to the right and then continued as sigmoid colon at the level of right pelvic brim [Table/Fig-2,5]. Both limbs of sigmoid mesocolon were attached to posterior abdominal wall, 3.5 cm from right of midline, opposite L5 to S3 vertebrae. The sigmoid colon was 3.5cm right of midline and caecum occupied right iliac fossa. The inferior mesenteric artery (L3) supplied right sided sigmoid colon from left side [Table/Fig-5]. The left colic branch of inferior mesenteric artery divided into three branches: left colic1, left colic2 and left colic3. The left colic1 divided into ascending and descending branch. The descending branch ended by anastomosing with the ascending branch of left colic2. The ascending branch ended by anastomosing with the left branch of middle colic. The descending branch of left colic2 anastomosed with left colic3 [Table/Fig-3,4].
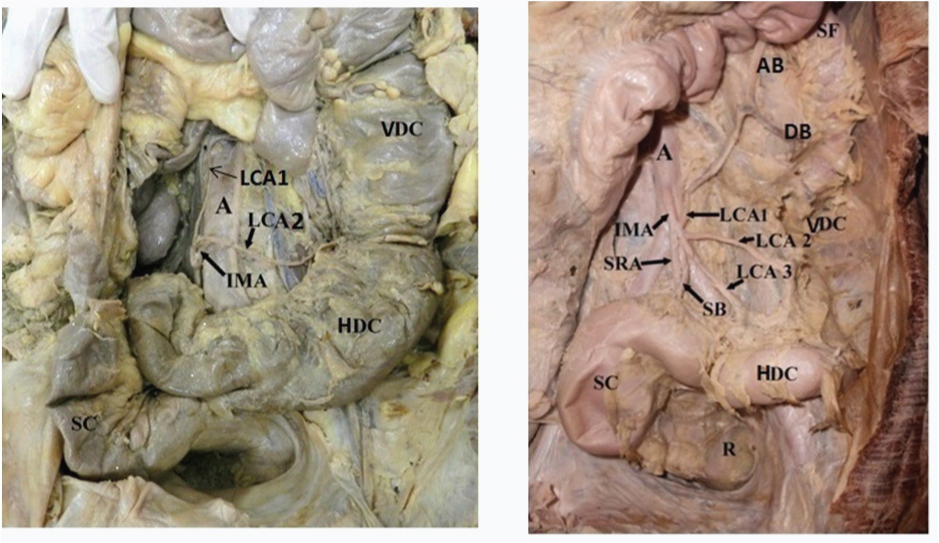
Photograph showing the anomalous branching pattern of inferior mesenteric artery supplying the long descending colon. In first case left colic branch of inferior mesenteric artery divided into, left colic1(LCA1) and left colic2(LCA2), to supply the long segment of descending colon. In second case left colic branch was seen to be dividing into three branches: left colic1(LCA1), left colic2(LCA2) and left colic3(LCA3). A: abdominal aorta, IMA: inferior mesenteric artery, SR: superior rectal artery, SB: sigmoidal branches, SF: splenic flexure, DC: descending colon, SC: sigmoid colon and R: rectum.
Discussion
Embryological development of the colon is complex and often unpredictable, leading to variations in the length and position. Jacob et al., reported caecum and appendix in the right lumbar region and the long loop of descending colon with right sided sigmoid colon [2]. Similar findings were observed in first case while in second case sigmoid colon was 3.5 cm to the right of midline with caecum in right iliac fossa and long loop of descending colon. Shrivastava et al., reported right sided descending and sigmoid colon and divided the anomalous colon into four parts [3]: First part: From splenic flexure to the right of midline at level of L5; Second: ascended upto L2; Third: descended on the right side of the ascending limb to the pelvic brim; Fourth: From right sacro-iliac joint to third sacral body. This descending colon and sigmoid colon loop had a common mesentery. In present cases the descending colon had a vertical segment in left lumbar region extending upto L4-L5 vertebral level and a horizontal segment that turned towards right across the abdominal cavity, in first case to reach right lumbar region and at this point it ascended one vertebral level higher and then turned downwards to become sigmoid colon at the right pelvic brim. While in second case reached 3.5 cm to the right and then continued as sigmoid colon. Indrajit et al., reported redundant loop (retroperitoneal) of descending colon with right sided sigmoid colon [4]. In our cases long loop of descending colon had a mesentery that fused with the mesentery of small intestine and the mesentery of sigmoid colon fused with right pelvic wall. Banerjee et al., conducted a study on 25 cadavers and found 96% of the caecum in Right iliac fossa and 4% in sub hepatic position [5]. Caecum was in right lumbar region in our first case and in second case it occupied right iliac fossa. Kanagasuntheram et al., classified redundant colon into four groups [6]: Group I: Presence of complete ascending and descending mesocolon; Group II: Presence of double hepatic flexure; Group III: Extension of sigmoid colon into the abdominal cavity; and Group IV: Displacement of sigmoid colon towards the right side. In the current cases complete ascending and descending mesocolon along with double flexure: (hepatic and splenic) and right sided sigmoid colon was observed. According to Kanagasuntheram et al., our variant cases would fall into Group I, II and IV category.
Embryological basis
The growth and rotation of midgut can be studied in four stages [7]:
Stage 1: No distinct boundary between the extra- and intra-embryonic coeloms;
Stage 2: Midgut loop in the extraembryonic coelom;
Stage 3: Return of the gut to the abdominal cavity;
Stage 4: Ultimate fixation of the gut derivatives.
In these two variations stage 1&2 of gut rotation can be presumed to be normal. The redundant loop of descending colon in both cases can be due to excess growth of the caudal segment of gut tube in stage 3. And due to faulty fixation of gut derivatives in stage 4, the mesentery of ascending and descending colon failed to fuse with the peritoneum of posterior abdominal wall and led to the retention of the mesentery. In case one early fixation of sigmoid colon on right side caused imperfect descent of caecum because of which it was observed in right lumbar region and lead to short length of ascending colon. While in second case the sigmoid colon occupied 3.5 cm right of midline so caecum occupied right iliac fossa.
The forkhead box transcription factor Foxf1 plays a key role in the formation of dorsal mesentery. The ultrastructural changes in the dorsal mesentery initiate intestinal rotation and generate the left-right asymmetry [8]. Intestinal malrotation can be due to abnormalities of either left-right patterning, dorsal mesentery, intestine itself or may be due to other abdominal contents. The identification of new genes with a role in intestinal development will benefit families via genetic counseling, information about recurrence risk and pre-natal diagnosis where the disorder is lethal.
Conclusion
The case of right sided sigmoid colon and long descending colon may present with symptoms that may suggest gastric ulcer, heart disease, appendicitis, chronic obstruction of bowel, so in diagnosing these conditions the possibility of redundant colon should be kept in mind. Gas shadow in right ilac fossa in plain radiographs can be mistaken for caecal gas and can cause difficulty during surgical intervention. The identification of new genes with a role in intestinal development will benefit families via genetic counseling, information about recurrence risk and pre-natal diagnosis where the disorder is lethal.
[1]. Romanes GJ, Cunningham’s manual of practical anatomy 2007 15th edNew YorkOxford medical publications:118-146. [Google Scholar]
[2]. Jacob M, Shivarama CH, Bindu S, Nallathamby R, Avadhani R, Undescended caecum and appendix with right sided sigmoid colon - a case reportNitte University Journal of Health Sciences 2013 3(4):2249-7110. [Google Scholar]
[3]. Shrivastava P, Tuli A, Kaur S, Raheja S, Right sided descending and sigmoid colon: its embryological basis and clinical implicationsAnat Cell Biol 2013 46(4):299-302. [Google Scholar]
[4]. Gupta I, Majumdar S, Mandal S, A redundant loop of descending colon and right sided sigmoid colonInternational Journal of Anatomical Variations 2012 5:11-13. [Google Scholar]
[5]. Banerjee A, Kumar IA, Tapadar A, Pranay M, Morphological Variations in the Anatomy of Caecum and Appendix - A Cadaveric StudyNational Journal of Clinical Anatomy 2012 1(1):30-35. [Google Scholar]
[6]. Kanagasuntheram R, Some observations of the development of the human duodenumJ Anat 1960 94:231-40. [Google Scholar]
[7]. Sadler TW, Langman’s Medical Embryology 2009 11th EdBaltimore, Philadelphia, New DelhiLippincott Williams and Wilkins:209-231. [Google Scholar]
[8]. Martin V, Shaw-Smith C, Review of genetic factors in intestinal malrotationPediatric surgery international 2010 26:769-81. [Google Scholar]