A Case of Reverse Palmaris Longus Muscle- An Additional Muscle in the Anterior Compartment of the Forearm
Sapna Marpalli1, Ashwini Lagadamane Sathynarayana Bhat2, Mohandas Rao Kappettu Gadahad3
1 Senior Grade Lecturer Department of Anatomy, Melaka Manipal Medical College, Manipal University, Manipal, Karnataka, India.
2 Lecturer, Department of Anatomy, Melaka Manipal Medical College, Manipal University, Manipal, Manipal, Karnataka, India.
3 Professor, Department of Anatomy, Melaka Manipal Medical College, Manipal University, Manipal, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sapna Marpalli, Senior Grade Lecturer, Department of Anatomy, Melaka Manipal Medical College, (Manipal Campus) Manipal University, Manipal, Udupi District-576 104, Karnataka, India.
E-mail: sapnamarpalli@gmail.com
It is uncommon to have additional muscles in the upper limb. Some of them may restrict the movements or compress the nerves and vessels, while others may go unnoticed. During the routine dissection for undergraduate medical students, we observed an additional muscle in the anterior compartment of the forearm in about 60-year-old male cadaver. The muscle had a prominent belly and a long tendon. Distally, it was attached to the flexor retinaculum by a short and thick tendon. Proximally, long tendon of the muscle passed between the flexor carpi ulnaris and palmaris longus and was attached to the common aponeurosis shared by the extensor carpi ulnaris and flexor digitorum profundus muscles. The additional muscle belly was supplied by a branch from the anterior interosseous nerve. The ulnar nerve and artery was passing deep to the fleshy belly of the muscle. The muscle reported here might compress the ulnar nerve and artery and may produce neurovascular symptoms. On the other hand, the tendon and fleshy belly of the muscle could be useful in muscle/tendon grafts. The observations made by us in the present case will supplement our knowledge of variations of the muscles in this region which could be useful for surgeons during the forearm and hand surgeries.
Common aponeurosis, Flexor retinaculum, Tendon grafts, Ulnar nerve
Case Report
During the routine dissection for undergraduate medical students, an additional muscle in the anterior compartment of the right forearm in about 60-year-old male cadaver was observed. The additional muscle was in the superficial aspect of the anterior compartment of the forearm. When compared to other superficial muscles of this region, the additional muscle was found to be reversed palmaris longus with its belly in the distal part of the forearm extending towards wrist and the tendon running towards the proximal aspect. The thin long tendon of the additional muscle passed between the fleshy bellies of palmaris longus and flexor carpi ulnaris muscles and when traced proximally, it was blending with the common aponeurosis shared by extensor carpi ulnaris and flexor digitorum profundus muscles. The fleshy belly of the muscle in the lower one third of the forearm was passing superficial to the flexor retinaculum. Anterior to the wrist joint, the fleshy belly ended in a thick tendon which was attached to the anterior aspect of the flexor retinaculum and to the carpal ligaments just deep to the palmar aponeurosis [Table/Fig-1,2]. The ulnar nerve and artery were passing deep to the fleshy belly of the additional muscle. The additional muscle was supplied by a branch of anterior interosseous nerve. There was no such variation observed on the other hand.
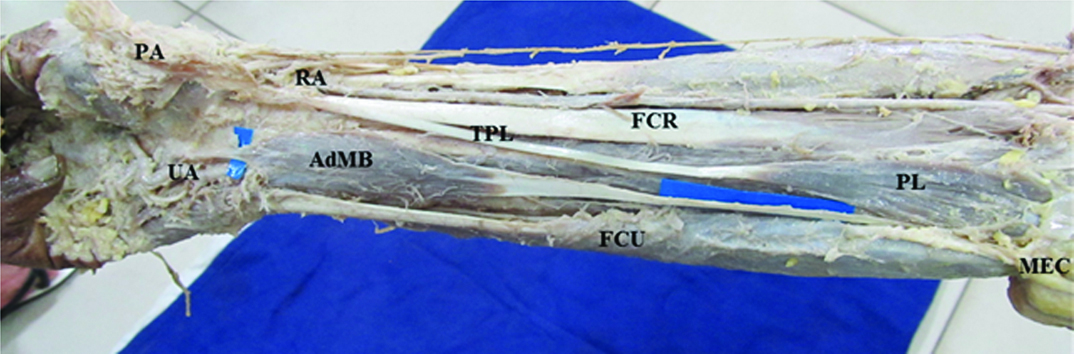
Photograph showing the dissection of the anterior compartment of the right forearm and palm. The picture shows the exposed anterior compartment of the forearm and proximal part of the palm to show the additional muscle belly (AdMB) with long tendon, proximal attachment of the tendon lies between the palmaris longus and flexor carpi ulnaris, and the distal part of it with fleshy muscle belly above the flexor retinaculum.
MEC- Medial Epicondyle, FCR- Flexor Carpi Radialis, RA - Radial Artery, TPL- Tendon of Palmaris Longus, FCU-Flexor Carpi Ulnaris, PL- Palmaris Longus, UA- Ulnar Artery, PA- Palmar Aponeurosis, AdMB- Additional Muscle Belly
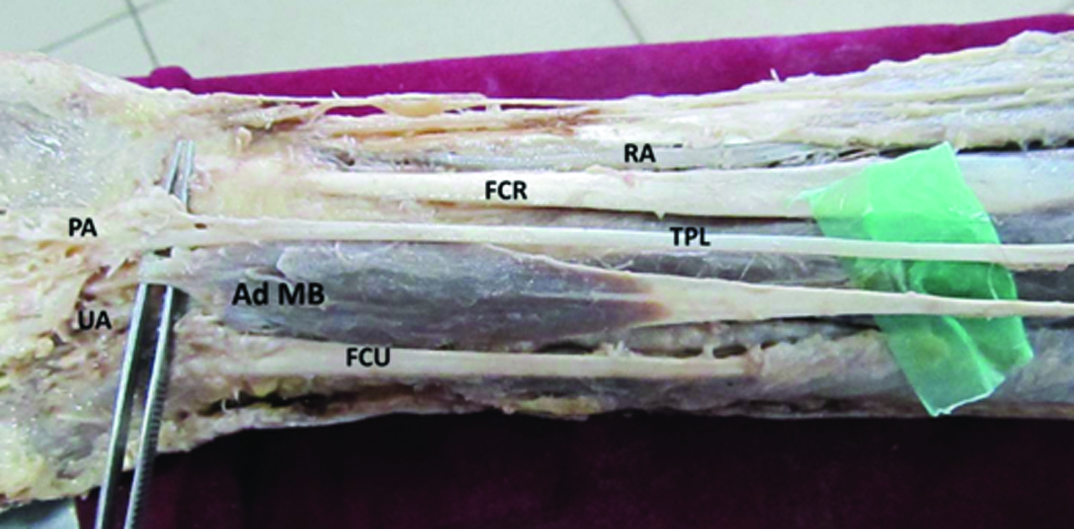
Photograph showing the dissection of distal part of the anterior compartment of the right forearm. The picture shows the distal attachment of the Additional musle belly (AdMB) distally ended in a thick tendon which was attached to the anterior aspect of the flexor retinaculum and to the carpal ligaments just deep to the palmar aponeurosis.
(FCR- Flexor Carpi Radialis, RA - Radial Artery, TPL- Tendon of Palmaris Longus, FCU-Flexor Carpi Ulnaris, Ad MB- Additional Muscle Belly, PL- Palmaris Longus, UA- Ulnar Artery, PA- Palmar Aponeurosis)
Discussion
Anterior compartment of the forearm consists of 5 superficial muscles and 3 deep muscles. The superficial muscles are pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis and flexor carpi ulnaris. These are attached proximally to the medial epicondyle of the humerus. Three deep muscles are flexor digitorum profundus, flexor pollicis longus and pronator quadratus. The muscles in this compartment are proximally attached to the different parts of the radius and ulna. As well as the overlying antibrachial fascia and the interosseous membrane and also to the septa which are passing between the individual muscles [1]. It is known that normally all these muscles have their fleshy part proximally and the tendinous part distally towards the hand. The distal attachment of these muscles attachments will vary, some of them attach to the carpal bones, and others attach to the digits.
Existence of an additional muscle in the forearm is not common. Usually any additional muscle in the flexor compartment of the forearm may not produce any major abnormal symptoms in individuals; instead it may cause compression of the neurovascular structures passing through this region. There are several cases of variations of additional tendon or belly of flexor digitorum superficialis muscle [2,3]. There may be two palmaris longus (PL) muscles [4]. The additional PL muscle may arise from the medial intermuscular septum, biceps or brachialis, the fascia of the forearm proximally or one of the neighbouring muscles. The distal attachment of this muscle is also variable it may be attached to the tendon of flexor carpi ulnaris, or any of the flexor tendons, flexor retinaculum, on the thenar or the hypothenar muscles. It may be directly attached to the deeper bones namely pisiform bone, scaphoid bone, or near to the metacarpophalangeal joint. These variable insertions of the additional muscle have a clinical importance because of its close relation with the median nerve and the ulnar nerve. Compression of the median and ulnar nerves in the region of the wrist which may result in ape hand, claw hand or even person cannot do the fine movements [5–7].
In the present case the additional muscle has a long tendinous proximal attachment and small fusiform belly at the distal part (distal third) of the forearm which looks like RPL but PL is normal in this case and we can consider this muscle as additional reversed PL muscle (Ad RPL). The distal attachment of the fleshy belly ended in the form of thick tendon which was attached to the anterior aspect of the flexor retinaculum and to the carpal ligaments just deep to the palmar aponeurosis. The present case has evident clinical/surgical significance. Unexpected muscular belly in the distal part of the forearm and a thick tendon in the region of the wrist which may cause the complications in the interpretation of local radiological images [8] and even in the wrist endoscopic & electromyographic procedures for the treatment of the carpal tunnel syndrome [9].
Although PL is categorized as one of the most variable muscles in the body and is classified as a phylogenetically retrogressive metacarpophalangeal joint flexor [10]. Like many other vestigial structures, this tendon served a practical purpose at some point in our evolutionary history. The structure serves no specific purpose to human being. PL tendon is commonly used as a graft source by hand surgeons, pre-operative researches should be carefully performed in suspicious cases [11].
Conclusion
Knowledge of occurrence of Ad RPL muscle is very important for hand surgeons, the distal attachment of the muscle belly and the tendon may confuse with the nerve even by an experienced surgeon. The clinician must consider this possibility if there is any suspicion of an abnormal swelling in the distal forearm. In this regard, the knowledge of this variation becomes handy to the surgeons.
[1]. Standring S, Ellis H, Healy JC, Johnson D, Williams A, Collins P, From Gray’s Anatomy: The Anatomical Basis of Clinical Practice 2005 39th editionEdinburghElsevier Churchill Livingstone:879-81. [Google Scholar]
[2]. Vincent R, Satheesha BN, Mohandas KGR, Venkataramana V, Nagabhooshana S, Ashutosh SR, Abnormal muscle in the anterior compartment of the forearm case reportCases J 2009 2:9125 [Google Scholar]
[3]. Shoja MM, Tubbs RS, Loukas M, Shokouhi G, The split flexor digitorum superficialisItal J Anat Embryol 2008 113(2):103-07. [Google Scholar]
[4]. Iqbal S, Raiz Iqbal, Faiz Iqbal, A bitendinous palmaris longus. Aberrant insertions and its clinical impact - a case reportJ Clin Diagn Res 2015 9(5):AD03-05. [Google Scholar]
[5]. Colin G, Thomas JR. Clinical manifestations of an accessory palmaris muscleJ Bone Joint Surg Am 1958 40(4):929-30. [Google Scholar]
[6]. Regan PJ, Roberts JO, Bailey BN, Ulnar nerve compression caused by a reversed Palmaris longus muscleJ Hand Surg Br 1988 13(4):406-07. [Google Scholar]
[7]. Hayes JR, Mulholland RC, O’Connor BT, Compression of the deep palmar branch of the ulnar nerve. Case report and anatomical studyJ Bone Joint Surg Br 1969 51(3):469-72. [Google Scholar]
[8]. Seyhan T, Median nerve compression at the wrist caused by reversed 3-headed palmaris longus muscle:case report and review of the literatureAm J Orthop (Belle Mead NJ) 2005 34(11):544-46. [Google Scholar]
[9]. De Smet L, Median and ulnar nerve compression at the wrist caused by anomalous muscles: review articleActa Orthop Belg 2002 68(5):431-38. [Google Scholar]
[10]. Fazan VPS, Reversed palmaris longus muscle and median nerve Relationships:Case report and literature reviewBraz J Morphol Sci 2007 24(2):88-91. [Google Scholar]
[11]. Acikel C, Ulkur E, Karagoz H, Celikoz B, Effort-related compression of median and ulnar nerves as a result of reversed three headed and hypertrophied palmaris longus muscle with extension of Guyon’s canalScan J Plast Reconstr Surg Hand Surg 2007 41:45-47. [Google Scholar]