Maxillary Incisor with Internal Resorption: Endodontic and Restorative Management
Alberto Dagna1
1 Assistant Professor, Endodontic Unit, Department of Clinical Surgical, Diagnostic and Pediatric Sciences, University of Pavia, Italy.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Alberto Dagna, Via Buozzi 55, 15121 Alessandria, Italy.
E-mail: alberto.dagna@unipv.it
Dental trauma, Endodontic treatment, Internal root resorption
A 34-year-old female patient reported with a chief complaint of cervical erosion and discoloration of upper maxillary central incisor with the history of trauma a week before. The patient said the tooth showed a pink spot on the crown at the cervical area 36 hours after the trauma, with no symptoms. Few days before she observed the erosion of the enamel at the same area, since it become a cavity in the next days.
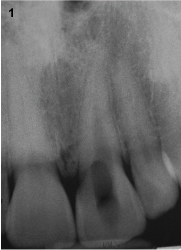
Radiographic examination showed the presence of an internal resorption at the crown,starting from the pulp chamber [Table/Fig-1]. No symptoms, no mobility, no pain on percussion were present and the vitality of the tooth were maintained (positive response to cold test). Prior to commencement of the procedure, treatment modality, cost benefit and risk were explained to the patient and appropriate consent was taken.
Initial radiograph with evidence of IRR at the crown.
Local anaesthesia was administered. Enamel and dentine around the lesion were removed [Table/Fig-2] and a cervical restoration with composite resine was planned. At the same time the palatine access cavity was open with a diamond bur and all pulpal tissue was removed using Endoflare Ni-Ti rotary file (MicroMega, Besancon, France) and hand stainless-steel K files n.10 and n.15. The canal was irrigated with 5% sodium hypochlorite (NaOCl) to control the bleeding and to dissolve residual pulp tissue. So the restoration with composite resin (Filtek Supreme XTE, 3M Espe, Seefeld, Germany) of the coronal perforation was done, respecting all the protocols for adhesion. An intraoperative radiographic control of the restoration was done after removal of the rubber dam clamp, in order to control the fitting of the restoration [Table/Fig-3]. Then the rubber dam was replaced and root canal treatment was continued with the Revo-S Ni-Ti system (MicroMega, Besancon, France): all the sequence was done using SC1, SC2 and SC: the root canal was prepared at 25/.06. All the steps were done in presence of abundant irrigation with 5% NaOCl and 17% EDTA solutions. Irrigating solutions were frequently replaced. At the end of the treatment NaOCl was activated for 4 minutes using the Endo Activator(MailleferSimit Dental, Baillagues, Switzerland) and the whole root canal was filled with Calcium hydroxide (MM Paste, MicroMega, Besancon, France). A temporary restoration of the access cavity was placed and a radiograph was taken for control [Table/Fig-4]. [Table/Fig-5] shows the restored tooth immediately at the end of the treatment.
Intraoral view of the incisor after cleaning of coronal resoprtion with high- and low-speed burs: the root canal is visible through the cavity.

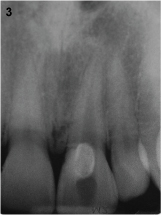
Radiographic control of composite resin restoration of the cervical cavity
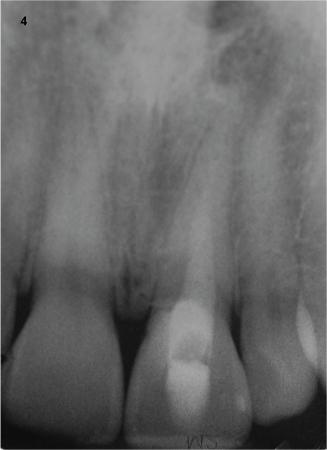
Radiographic control of the temporary filling with Calcium hydroxide after initial treatment and removal of whole pulp tissue.
Aspect of the tooth after restoration with composite resin.

The patient was recalled three weeks later for a second visit: no symptoms were present and the root canal treatment was finished. The root canal was irrigated with the copious amount of 5% NaOCl and the shaping was completed with Revo-S Apical 30 and 35 (MicroMega, Besancon, France). After verifying the complete removal of the Calcium hydroxide with the aid of the operating microscope, the final rinse with activated 5% NaOCl was done and the root canal was dried with paper points. The root canal obturation was done with the continuous wave technique [Table/Fig-6]: sealing of the apical third with warm gutta-percha compacted by the System B Heat source (Sybron Endo, Orange, CA, USA) and the MM Seal (MicroMega, Besancon, France) as sealer; backfilling obtained using Obtura II syringe (Spartan, Fenton, MO, USA). The patient was recalled one week later for the final obturation of the access cavity with composite resin (Filtek Supreme XTE, 3M Espe, Seefeld, Germany).
Radiographic control after obturation of the root canal.

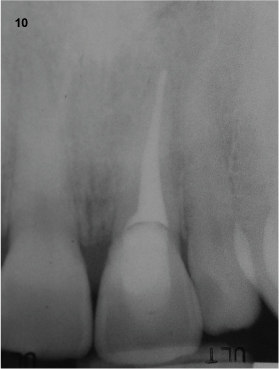
Radiographs were taken after two months [Table/Fig-7], after six months [Table/Fig-8] and after 12 months [Table/Fig-9]. The last control was done after two years [Table/Fig-10,11]. The tooth was asymptomatic and completely healed. No apical and peri-radicular lesions or signs of new resorption were visible.
A 2 months recall radiograph.

A 6 months recall radiograph.

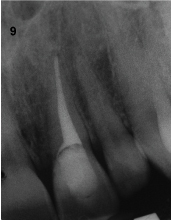
A 12 months recall radiograph.
A 24 months recall radiograph.
Clinical and healthy aspect of the tooth after 24 months recall.

Discussion
Internal Root Resorptionn (IRR) is a process associated with either a physiologic or a pathologic process resulting in the loss of dentin, cementum and/or bone [1].
Aetiology of IRR is quite unclear. Various aetiologic factors have been proposed for the loss of dental tissue, but trauma and pulpal inflammation/infection seems to be the major contributory factors in the initiation of internal resorption [2,3]. It’s usually asymptomatic and often recognized clinically through routine full mouth radiographs. Pain may occur depending on the pulpal condition or perforation of the root resulting in a periodontal lesion [4].
The correct diagnosis of IRR is necessary to program the right endodontic and restorative treatment. Only the complete removal of the vital pulp tissue and the repair of the perforation can preserve the tooth.
[1]. American Association of Endodontists, “Glossary of endodontic terms,” 2012, http://www.aae.org/glossary/ [Google Scholar]
[2]. Patel S, Ricucci D, Durak C, Tay F, Internal root resorption: A reviewJ Endod 2010 36:1107-21. [Google Scholar]
[3]. Nilsson E, Bonte E, Bayet F, Lasfargues JJ, Management of internal root resorption on permanent teethInt J Dent 2013 2013:929486doi:10.1155/2013/929486. Epub 2013 Nov 21 [Google Scholar]
[4]. Caliskan MK, Turkun M, Prognosis of permanent teeth with internal resorption: a clinical reviewDent Traumatol 1997 13(2):75-81. [Google Scholar]