Introduction
The ultimate goal of physiotherapy in stroke rehabilitation is focused towards physical independence and to restore their functional ability during activities of daily living (ADLs). Motor imagery (MI) is an active process during which a specific action is reproduced within working memory without any actual movements. MI training enhances motor learning, neural reorganization and cortical activation in stroke. The efficacy of MI training involving lower extremity mobility tasks need to be assessed.
Aim
To evaluate the effects of combining motor imagery with physical practice in paretic Lower Extremity Muscles Strength and Gait Performance in Ambulant Stroke subjects.
Materials and Methods
A Randomized Clinical Trial was conducted in Department of Physical Therapy, Tertiary Care Hospitals, Mangalore, India which includes 40 hemi paretic subjects (>3 months post-stroke) who were ambulant with good imagery ability in both KVIQ-20 ≥ 60 and Time dependent MI screening test were recruited and randomly allocated into task-oriented training group (n=20) and task-oriented training group plus MI group (n=20). Subjects in both groups underwent task orientated training for lower extremity 45-60 minutes, 4 days per week for 3 weeks. In addition, the experimental group received 30 minutes of audio-based lower extremity mobility tasks for MI practice. Isometric muscle strength of Hip, Knee and Ankle using a hand-held dynamometer and self-selected 10 m gait speed were assessed before and after 3 weeks of intervention.
Results
Both the groups had found a significant change for all the outcome measures following 3 weeks of interventions with p <.05. The experimental group had shown a significant improvement in paretic hip muscles (both flexors and extensors), knee extensors and ankle dorsiflexors and gait speed compare to control group with p < .05 between group analyses.
Conclusion
Additional task specific MI training improves paretic muscle strength and gait performance in ambulant stroke patients.
Introduction
The ultimate goal of physiotherapy in stroke rehabilitation is focused towards physical independence and to restore their functional ability during Activities of Daily Living (ADLs). There are substantial evidences that post stroke muscle weakness rather than spasticity (abnormal reflex activity) contributes for motor impairments in hemiparesis which further leads to loss or limitation in mobility functions including walking [1,2]. Recent trends in gait rehabilitation in stroke research have shown that there are substantial evidences that the treatment approaches should be focused on retraining functional tasks rather than impairments such as individual muscle strengthening [3,4].
Repetitive Task specific training which focuses on practicing specific functional tasks showed benefits for gait speed and coordination after stroke [4,5]. However in recent years there are new non-invasive rehabilitative techniques that are found to enhance cortical plasticity include mirror therapy, or mental practice with motor imagery are emerging as interesting options as adjunct interventions to standard physical therapies [6]. Hence, physical therapists should not limit their practice to a single ‘named’ approach rather they should incorporate multidimensional framework for successful locomotor rehabilitation programme [7].
Motor imagery (MI) is an act of producing an internal representation of a movement without generating any motor output [8]. Motor Imagery Training (MIT) is found to improve motor performance and learning, neural reorganization and cortical activation in Stroke [9–11]. Recent studies have recognized that MIT on movement tasks produce a positive effect on locomotor skills and these studies are limited to Functional mobility scales, Lower Extremity EMG muscle activations and Kinematic gait parameters [12–16]. Evidence of MI benefits in enhancing strength has been reported by other researchers [17,18]. However, efficacy of MIT on paretic muscle strength and gait performance is limited in Stroke literature.
Aim
To find the efficacy of lower extremity task specific motor imagery as an adjunct on muscle strength gain and gait functions in stroke.
Materials and Methods
Participants: Participants were identified from retrospective search from inpatient/ outpatient registry from April 2012-June 2013 and were referred for a comprehensive rehabilitation programme in Kasturba Medical College and Hospitals, Mangalore, Manipal University, Karnataka, India. Primary investigator (V.K., a Physical therapist) contacted the potential subjects through telephonic communication / information letter about the study purpose and interested participants were assessed for the eligibility. Subjects who met the following criteria were included: a) Unilateral first episode of stroke at least 3 months (ischemic / haemorrhagic) with residual hemi paresis before recruitment; b) Brunnstorm recovery stage ≥ 5 for lower extremity; c) Functional Ambulation Category level 2 and above; d) Mini –Mental state examination score was 24 points or higher; e) Kinesthetic and visual imagery score (KVIQ-20) Only ≥ 60 able to do Time dependent MI screening test [19]. The exclusion criteria was: history of CNS diseases, major head injury, Neuro psychiatric diseases, Cerebellar or Brain stem stroke, dizziness or vertigo that limits walking, severe visual defect, peripheral vascular diseases etc. Serious cardiac conditions which required hospitalization in the past 6 months, major musculoskeletal or orthopaedic surgeries in lower extremities and those who participated in MI program related to physical activity within the previous three months. This trial was conducted from April 2012-June 2014 and completed with 40 hemi paretic stroke subjects.
Study Design: The present study was on assessor-blinded randomized clinical trial design. Total 40 participants were randomly assigned to receive either experimental (n=20) or the control group (n=20) using block randomization (4 blocks with 10 subjects in each block). The primary investigator generated the randomization list using computer generated random numbers and allotted each subject interventions assignment which were enclosed in sealed opaque envelopes.
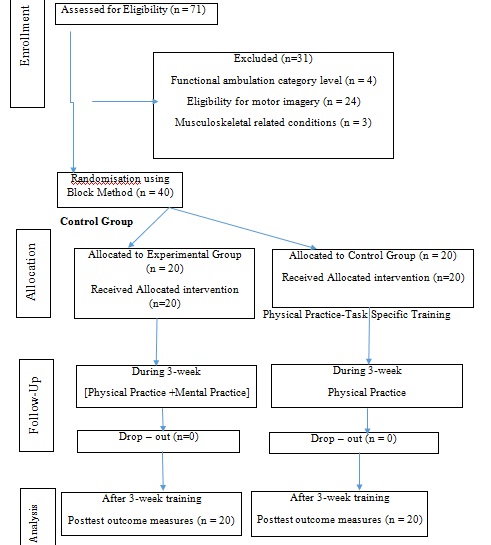
Procedure: This study was approved by Institutional Ethical Committee Board, Manipal University. A briefing about the study was given to the stroke subjects and the family members/caretaker. From the interested participants, a signed informed consent was obtained and then screened for study criteria. Selected subjects were then randomly allocated to Physical practice (Control) and Physical plus Mental practice (Experimental) group. Forty stroke subjects in both the groups underwent task specific training for lower extremity functions approximately 45-60 min per session, conducted 4 times a week for 3 weeks. All the sessions were delivered one-on-one by a primary investigator, who is a qualified trained physical therapist [Table/Fig-1].
CONSORT (consolidated standards of reporting trails) diagram showing the flowchart of participants through each stage of the Study.
Task specific training programme focused on improving the performance and endurance of functional tasks involving the lower extremities such as sit-to-stand, reaching in sitting and standing, marching, walking, turning and transfers. The participants were encouraged to perform all the exercises in all of the programme sessions to a maximum of 60 minutes with adequate rest periods for 10-15 minutes. The level of difficulty of the training programme was progressed by number of task repetitions, task complexity and environmental constraints which was matched according to the subject’s performance [20,21].
Experimental Group: Mental practice programme started with familiarization period and was followed by training of lower extremity tasks for the next 2 weeks. In the familiarization phase the subjects are explained about the basic action thoughts or motor representations of complex movements (for example drinking a cup of tea using Structural Dimension Analysis of Motor Memory) [22]. To enhance the imagery ability, verbal instructions and explanation of the lower extremity task components which were practiced in physical practice, by means of pre-recorded audio tape with total duration 15 minutes delivered in subjects own language, before and during the physical practice training. The taped intervention consists of 2 minutes relaxation followed by 12 minutes of cognitive visual images related to the lower extremity task characteristics (e.g. Imagine yourself in a warm, relaxing place and you are bending your knee and feel the tightness in your muscles). Subjects were then taught to visualize themselves performing the required task and also experience kinesthetic sensations related to the task. This was followed by refocusing of attention to the immediate surroundings and genuine body position [23] [Table/Fig-2].
Schematic representation of the experimental protocol for Motor Imagery Training.
| Pre treatment | Familiarization phase | Motor Imagery Training Programe | Post treatment |
|---|
| Baseline | Week 1 | Week 2 | Week 3 | Outcome Measures |
|---|
| Assessment ofImagery ability | Structured Dimension Analysis of Motor Memory (eg drinking a cup of tea) | Tasks related to Sitting, Standing | Tasks related to Walking | Muscle Strength-Hip-Knee-AnkleGait Speed |
| Dosage | 30 minutes for4 Sessions | 30 minutes for4 sessions | 30 minutes for4 sessions | |
Outcome measures: A trained physical therapist with five years of experience in stroke rehabilitation was assigned as an independent blinded assessor to administer the outcome measures at two assessment points. Data was collected at baseline and after 3 weeks of intervention period.
Strength evaluation by using hand held dynamometer: The test procedure consists of measurement of maximum isometric strength in six major muscle groups of bilateral lower extremities using hand held dynamometer (Baseline Push Pull Dynamometer, Fabrication Enterprises, New York, USA) a reliable and valid tool to measure muscle strength in stroke subjects [24,25]. All tests were ‘make’ test where the dynamometer was held stationary by the examiner while the subject exerts a maximum force against it [26]. Test positions were standardized [27,28] and the following six muscle groups were evaluated: hip flexors and extensors, knee flexors and extensors, ankle dorsi flexors and plantar flexors. Subjects were trained for one practice trial followed by three test trials for each six muscle groups. Each test trial lasted for approximately 5 seconds to allow the subject to generate maximum voluntary effort. A 30 second break was followed after each trial. The average of three trials was taken and muscle force was recorded in Newton (N) for all the six muscle groups.
Gait Speed: Subjects were asked to walk at their normal comfortable pace over a set distance clearly marked on the floor (10 m) and an average of 3 trials was taken. Subjects were rested one minute between each trial and their gait speed was calculated by dividing the distance walked by the time duration [29].
Statistical Analysis
All data was analysed using Statistical Package for Social Sciences version 16.0 for Windows. Group characteristics at baseline were presented using means and standard deviations for continuous variables and percentages for categorical variables. The results were statistically analysed using the Fisher-exact test, Chi Square test, paired and independent t-test to analyse and compare between the scores of control group with that of the experimental group. A p-value of <0.05 was considered to be statistically significant.
Results
There were 71 subjects screened for eligibility and 40 subjects were included in our study. Baseline Demographics showed the groups means and standard deviations for age, duration since the onset of stroke, NIHSS, KVIQ and MMSE scores. It also showed the frequency counts for gender, type of lesion, paretic side, risk factors, Brunstrom lower extremity stage of recovery, use of assistive devices and Functional Ambulation Category level. Mean age of our study participants were 51 years in control and 53 years in experimental group respectively. Majority of them were men, predominately haemorragic type of stroke and were less than one year post stroke duration before recruiting for the intervention in both the groups. National Institute of Health Stroke Scale (NIHSS) mean score for both the groups was found to be less than 8 which describes that our participants were mild in stroke severity. An 80% participant were in stage 5 of Burnstorm Lower extremity stage of recovery and level 3 of FAC in their ambulation level which also explains their better motor recovery. Participants’ imagery ability KVIQ mean score was 64.55 in control and 65.55 in experimental group respectively. Both the groups were matched for all the above-mentioned criteria, as there were no statistically significant differences found between the two groups as shown in [Table/Fig-3].
Demographic characteristics of the participants.
| Characteristic | Control Group (n=20) | Experimental Group (n=20) | Test statistics |
|---|
| Mean Age, Years (SD) | 51.0(±5.80) | 53.0(±6.40) | t: p =.49 |
| Male/Female (%) | 14 (70) / 6 (30) | 16 (80) / 4 (20) | f : p = .46 |
| Mean time since Stroke, in months (SD) | 5.6(±2.20) | 6.5(±2.41) | t: p =.25 |
| Type of Stroke Ischemic/Haemorrhagic (%) | 5 (25) /15 (75) | 8(40)/12(60) | f : p =.09 |
| Side of involment Right/Left (%) | 9 (35) /11(65) | 10 (50) /10 (50) | χ2: p =.27 |
| Risk Factors (%) Modifiable/Non Modifiable/Both | 6 (30)/0/14(70) | 4(20)/2(10) /14(70) | f : p =.08 |
| Mean NIHSS (SD) | 5.4(±1.53) | 5.1(±1.16) | t: p =.49 |
| Brunstorm stage of recovery Stage 5/Stage 6 | 16(80) /4 (20) | 14 (70) /6 (30) | χ2: p =.15 |
| FAC % -Level 3/Level 4 | 18 (90) /2 (10) | 17 (85) /3 (15) | χ2: p =.21 |
| Mean MMSE (SD) | 28.5(±1) | 28.8(±1) | t: p =.49 |
| AFO/Cane as assistive devices | 2/1 | 0/2 | |
| Mean KVIQ Total Score (SD) | 64.5(±3.74) | 65.5(±3.48) | t: p =.39 |
MMSE = Mini-Mental State Examination; NIHSS = National Institutes of Health Stroke Scale; t = independent t test; χ2 = chi-square test; f = Fisher exact test
There has been a significant improvement in all the outcome measures in both the groups following 3 weeks of interventions with p <0.05. Between groups analysis the experimental group had shown a significant improvement in paretic hip muscles (both flexors and extensors), knee extensors and ankle dorsiflexors and also for gait speed compare to control group with p< .05 a as shown in [Table/Fig-4].
Muscle strength in newton and gait speed for both groups.
| Paretic MuscleStrength | Groups (n=20) in each | PreMean±SD | PostMean±SD | Mean Change Scores(Post-Pre) with 95%CI | p-valueb |
|---|
| HipFlexors | Control | 25.80±7.29 | 36.90±11.28 | 11.10(5.74-16.45)* | 0.01§ |
| Experimental | 23.57±6.78 | 46.70±15.10 | 23.13(16.95-29.26)** |
| HipExtensors | Control | 43.15±12.02 | 63.60±20.86 | 20.45(13.45-32.82)* | 0.01§ |
| Experimental | 44.04±14.04 | 72.28±17.70 | 28.25(18.31-38.19)* |
| Knee Flexors | Control | 34.24±6.93 | 62.04±18.68 | 27.80(19.15-36.45)* | 0.12 |
| Experimental | 29.24±11.06 | 61.3±16.55 | 32.13(27.01-37.26)* |
| Knee Extensors | Control | 78.54±18.55 | 107.64±28.56 | 29.09(17.82-40.37)** | 0.01§ |
| Experimental | 72.23±24.08 | 123.15±32.99 | 50.92(28.43-65.85)** |
| Ankle Dorsiflexors | Control | 22.23±7.06 | 35.36±9.73 | 13.12(7.78-18.86)* | 0.01§ |
| Experimental | 20.20±7.87 | 41.58±10.82 | 21.38(16.37-26.38)* |
| Ankle Plantarflexors | Control | 48.03±13.11 | 72.05±16.74 | 24.02(20.89-27.14)* | 0.15 |
| Experimental | 42.03±12.78 | 64.04±18.75 | 22.01(17.82-26.02)* |
| Gait Speed | Control | .52±.09 | .60±.08 | .08(.06-.10)* | 0.01§ |
| Experimental | .49±.08 | .63±.07 | .14 (.12-.15)** |
*- p value <.05 within Group, **- p value <.001 within Group
p-valueb - changes between Groups, §-significant change between Groups
Discussion
The purpose of this study was to determine the effects of lower extremity task specific motor imagery training as an adjunct in stroke rehabilitation. Our study results have shown that combined MIT training was found to be more beneficial in comparison to task –specific training alone to improve the paretic muscle strength and gait performance in ambulant stroke subjects. Majority of the subjects included in our study were in Brunnstrom recovery stages 5 and 6 and level 3 of Functional Ambulation Category thus ensuring that excessive spasticity and lower limb basic synergy patterns were not contributing for balance and gait related performances [30]. Since the included subjects were post-stroke 3 months and above, spontaneous recovery was fairly ruled out for our findings [31,32]. The baseline characteristics of all the subjects were similar in both the groups. As presented in [Table/Fig-4] which showed no significant statistical difference between them and hence did not influence the results of our study findings.
Our study results showed that following 3 weeks of lower extremity task specific training there was a significant improvement in the lower extremity muscle strength and gait performance for both groups and this effect was more in experimental group which received MIT training as an adjunct. These results are in consistent with previous studies on task specific training on lower extremity paretic muscle strength and gait performance in stroke population [33–35].
Recent evidences have shown that MIT is found to be effective for motor performance and motor learning in stroke rehabilitation. Our results have shown that MIT training also added benefits to improve paretic muscle strength in hip flexors and extensors, knee extensors and dorsiflexors. Neural adaptation is a key factor for strength gain in voluntary skeletal muscle training [36]. Earlier studies on MIT and muscle strength had shown that mental practice with motor imagery actively changes in central programming process such as motor planning which enhances for neural adaptation for maximal voluntary contraction (MVC) [37] and also kinesthetic imagery training could alter the greater activation in motor units which may attribute for our present findings [38–40].
Better improvement in walking speed was also observed in task specific MIT group as we found a greater change in key muscles for gait performance. Extensors play a major role in phase of gait cycle hence greater change in glutes and quadriceps strength in our study attribute for increase weight acceptance and loading of the paretic limb which may facilitate better swing phase [41]. Increased hip flexor and dorsiflexor activity in MIT group also contributes for better toe clearance in swing phase [42–44]. These findings could have attributed to better performance in 10 m walk test in the MIT group.
Limitations
This study has some limitations. Inadequate sample size or the effect size of the interventions were not addressed hence the difference in the groups may have arisen by chance that reduces the generalizability of our results. Our study participants had a high level walking functional ability hence, our results are limited and also to incorporate for low functional level stroke subjects. Our study also could not determine the long- term follow up. Hence there is a need to conduct a high quality clinical trial with more objective outcome measures such as brain imaging to improve internal and external validities.
Conclusion
Three weeks of task specific lower extremity imagery training as an adjunct was found to better improvement in lower limb paretic muscle strength and gait speed in ambulant stroke subjects.
MMSE = Mini-Mental State Examination; NIHSS = National Institutes of Health Stroke Scale; t = independent t test; χ2 = chi-square test; f = Fisher exact test
*- p value <.05 within Group, **- p value <.001 within Group
p-valueb - changes between Groups, §-significant change between Groups
[1]. Gray V, Rice CL, Garland SJ, Factors that influence muscle weakness following stroke and their clinical implications: a critical reviewPhysiother Can 2012 64(4):415-26. [Google Scholar]
[2]. Patten C, Lexell J, Brown HE, Weakness and strength training in persons with post stroke hemiplegia: rationale, method, and efficacyJ Rehabil Res Dev 2004 41(3A):293-312. [Google Scholar]
[3]. Hollands KL, Pelton TA, Tyson SF, Hollands MA, van Vliet PM, Interventions for coordination of walking following stroke: systematic reviewGait Posture 2012 35(3):349-59. [Google Scholar]
[4]. French B, Thomas L, Leathley M, Sutton C, McAdam J, Forster A, Does repetitive task training improve functional activity after stroke? A Cochrane systematic review and meta-analysisJ Rehabil Med 2010 42(1):9-14. [Google Scholar]
[5]. Rensink M, Schuurmans M, Lindeman E, Hafsteinsdóttir T, Task-oriented training in rehabilitation after strokeJ Adv Nurs 2009 65(4):737-54. [Google Scholar]
[6]. Faralli A, Bigoni M, Mauro A, Rossi F, Carulli D, Noninvasive strategies to promote functional recovery after strokeNeural Plast 2013 2013:854597doi:10.1155/2013/854597 [Google Scholar]
[7]. Bowden MG, Embry AE, Gregory CM, Physical therapy adjuvants to promote optimization of walking recovery after strokeStroke Res Treat 2011 2011:601416doi: 10.4061/2011/601416 [Google Scholar]
[8]. Decety J, Grèzes J, Neural mechanisms sub serving the perception of human actionsTrends Cogn Sci 1999 3(5):172-78. [Google Scholar]
[9]. Dickstein R, Deutsch JE, Motor imagery in physical therapist practicePhys Ther 2007 87(7):942-53. [Google Scholar]
[10]. Cha YJ, Yoo EY, Jung MY, Park SH, Park JH, Effects of functional task training with mental practice in stroke: A meta-analysisNeuro Rehabilitation 2012 30(3):239-46. [Google Scholar]
[11]. García Carrasco D, Aboitiz Cantalapiedra J, Effectiveness of motor imagery or mental practice in functional recovery after stroke: a systematic reviewNeurologia. SEGO 2013 16:pii: S0213–4853(13):00023-26. [Google Scholar]
[12]. Hwang S, Jeon H-S, Yi C, Kwon O, Cho S, You S, Locomotor imagery training improves gait performance in people with chronic hemiparetic stroke: a controlled clinical trialClin Rehabil 2010 24:514-22. [Google Scholar]
[13]. Kim JS, Oh DW, Kim SY, Choi JD, Visual and kinesthetic locomotor imagery training integrated with auditory step rhythm for walking performance of patients with chronic strokeClin Rehabil 2011 25(2):134-45. [Google Scholar]
[14]. Dickstein R, Levy S, Shefi S, Holtzman S, Peleg S, Vatine JJ, Motor imagery group practice for gait rehabilitation in individuals with post-stroke hemiparesis: A pilot studyNeuro Rehabilitation 2014 34(2):267-76. [Google Scholar]
[15]. Vijayakumar K, Chakrapani M, Integrated Mental Practice Training Improves Functional Mobility in Chronic Stroke: A Pilot StudyInternational Journal of Neurology Neurosurgery 2011 3(2):15-20. [Google Scholar]
[16]. Vijayakumar K, Chakrapani M, Shennoy UV, Mental practice with motor imagery on functional mobility in chronic stroke: A pilot randomized clinical trialInternational Journal of Scientific Research 2013 2(5):434-37. [Google Scholar]
[17]. Yue G, Cole KJ, Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractionsJ Neurophysiol 1992 67(5):1114-23. [Google Scholar]
[18]. Lebon F, Collet C, Guillot A, Benefits of motor imagery training on muscle strengthJ Strength Cond Res 2010 24(6):1680-87. [Google Scholar]
[19]. Malouin F, Richards CL, Durand A, Doyon J, Clinical assessment of motor imagery after strokeNeurorehabil Neural Repair 2008 22(4):330-40. [Google Scholar]
[20]. Outermans JC, van Peppen RPS, Wittink H, Takken T, Kwakkel G, Effects of a high-intensity task-oriented training on gait performance early after stroke: a pilot studyClin Rehabil 2010 24(11):979-87. [Google Scholar]
[21]. Verma R, Arya KN, Garg RK, Singh T, Task-oriented circuit class training program with motor imagery for gait rehabilitation in post stroke patients: a randomized controlled trialTop Stroke Rehabil 2011 18(Suppl 1):620-32. [Google Scholar]
[22]. Braun SM, Beurskens AJ, Schack T, Marcellis RG, Oti KC, Schols JM, Is it possible to use the Structural Dimension Analysis of Motor Memory (SDA-M) to investigate representations of motor actions in stroke patients?Clin Rehabil 2007 21(9):822-32. [Google Scholar]
[23]. Braun S, Kleynen M, Schols J, Schack T, Beurskens A, Wade D, Using mental practice in stroke rehabilitation: a frameworkClin Rehabil 2008 22:579-91. [Google Scholar]
[24]. Andrews AW, Bohannon RW, Distribution of muscle strength impairments following strokeClin Rehabil 2000 14(1):79-87. [Google Scholar]
[25]. Kolber MJ, Cleland JA, Strength testing using hand-held dynamometryPhys Ther Rev 2005 10:99-112. [Google Scholar]
[26]. Burns SP, Spanier DE, Break-technique handheld dynamometry: Relation between angular velocity and strength measurementsArch Phys Med Rehabil 2005 86(7):1420-26. [Google Scholar]
[27]. Cooper A, Alghamdi GA, Alghamdi MA, Altowaijri A, Richardson S, The Relationship of Lower Limb Muscle Strength and Knee Joint Hyperextension during the Stance Phase of Gait in Hemiparetic Stroke PatientsPhysiother Res Int 2012 17(3):150-56. [Google Scholar]
[28]. Dorsch S, Ada L, Canning CG, Al-Zharani M, Dean C, The strength of the ankle dorsiflexors has a significant contribution to walking speed in people who can walk independently after stroke: An observational studyArch Phys Med Rehabil 2012 93(6):1072-76. [Google Scholar]
[29]. van Bloemendaal M, van de Water AT, van de Port IG, Walking tests for stroke survivors: a systematic review of their measurement propertiesDisabil Rehabil 2012 34(26):2207-21. [Google Scholar]
[30]. Mehrholz J, Wagner K, Rutte K, Meissner D, Pohl M, Predictive validity and responsiveness of the functional ambulation category in hemiparetic patients after strokeArch Phys Med Rehabil 2007 88(10):1314-19. [Google Scholar]
[31]. Verheyden G, Nieuwboer A, De Wit L, Thijs V, Dobbelaere J, Devos H, Time course of trunk, arm, leg, and functional recovery after ischemic strokeNeurorehabil Neural Repair 2008 22(2):173-79. [Google Scholar]
[32]. Kyoung Bo L, Six-Month Functional Recovery of Stroke Patients: A Multi-Time-Point Study. International Journal of Rehabilitation Research. Internationale Zeitschrift Fur Rehabilitations forschungRevue Internationale De Recherches De Readaptation 2015 38(2):173-80. [Google Scholar]
[33]. Wevers L, Van I, Vermue M, Mead G, Kwakkel G, Effects of task-oriented circuit class training on walking competency after stroke: A systematic reviewStroke 2009 40(7):2450-59. [Google Scholar]
[34]. Yang YR, Wang RY, Lin KH, Chu MY, Chan RC, Task-oriented progressive resistance strength training improves muscle strength and functional performance in individuals with strokeClin Rehabil 2006 20(10):860-70. [Google Scholar]
[35]. Nadeau SE, Wu SS, Dobkin BH, Azen SP, Rose DK, Tilson JK, Effects of task-specific and impairment-based training compared with usual care on functional walking ability after inpatient stroke rehabilitation: LEAPS TrialNeurorehabil Neural Repair 2013 27(4):370-80. [Google Scholar]
[36]. Farthing JP, Borowsky R, Chilibeck PD, Binsted G, Sarty GE, Neuro-physiological adaptations associated with cross-education of strengthBrain Topogr 2007 20(2):77-88. [Google Scholar]
[37]. Williams J, Pearce AJ, Loporto M, Morris T, Holmes PS, The relationship between corticospinal excitability during motor imagery and motor imagery abilityBehav Brain Res 2012 226(2):369-75. [Google Scholar]
[38]. Yao WX, Ranganathan VK, Allexandre D, Siemionow V, Yue GH, Kinesthetic imagery training of forceful muscle contractions increases brain signal and muscle strengthFront Hum Neurosci 2013 7:561 [Google Scholar]
[39]. Herbert RD, Dean C, Gandevia SC, Effects of real and imagined training on voluntary muscle activation during maximal isometric contractionsActa Physiol Scand 1998 163(4):361-68. [Google Scholar]
[40]. Yue G, Cole KJ, Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractionsJ Neurophysiol 1992 67(5):1114-23. [Google Scholar]
[41]. Saunders DH, Greig CA, Young A, Mead GE, Association of Activity Limitations and Lower-Limb Explosive Extensor Power in Ambulatory People with StrokeArch Phys Med Rehabil 2008 89(4):677-83. [Google Scholar]
[42]. Hyngstrom AS, Onushko T, Heitz RP, Rutkowski A, Hunter SK, Schmit BD, Stroke-related changes in neuromuscular fatigue of the hip flexors and functionalimplicationsAm J Phys Med Rehabil 2012 91(1):33-42. [Google Scholar]
[43]. Rybar MM, Walker ER, Kuhnen HR, Ouellette DR, Berrios R, Hunter SK, Hyngstrom AS, The stroke-related effects of hip flexion fatigue on over ground walkingGait Posture 2014 39(4):1103-08. [Google Scholar]
[44]. Mentiplay BF, Adair B, Bower KJ, Williams G, Tole G, Clark RA, Associations between lower limb strength and gait velocity following stroke: a systematic reviewBrain Inj 2015 29(4):409-22. [Google Scholar]