Co-existence of Endometriotic Cyst of the Ovary and Arias-Stella Reaction in a Non-Pregnant Woman: Report of a Rare Case
Volga Harikrishnan1, Muthuvel Esaki2, Chitra Srinivasan3, Parimala Arockiasamy4, Shanthi Ethirajan5
1 Assistant Professor, Department of Pathology, Saveetha Medical College, Thandalam, Tamilnadu, India.
2 Associate Professor, Department of Pathology, Saveetha Medical College, Thandalam, Tamilnadu, India.
3 Professor, Department of Pathology, Saveetha Medical College, Thandalam, Tamilnadu, India.
4 Associate Professor, Department of Obstetrics and Gynecology, Saveetha Medical College, Thandalam, Tamilnadu, India.
5 Assistant Professor, Department of Obstetrics and Gynecology, Saveetha Medical College, Thandalam, Tamilnadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Volga Harikrishnan, 5/235, Thiruvika Street, MPS Nagar, Behind SBI, Thiruvallur-602001, Tamilnadu, India.
E-mail: drhsvol@gmail.com
Endometriosis is defined as presence of endometrial tissue outside the uterus. It can occur anywhere in the ovary. In the ovary it is usually presented as cyst, termed as endometriotic cyst or Chocolate cyst. Arias-Stella reaction is usually seen in gestational endometrium or in ectopic gestation site and rarely in non-pregnant uterus with hormonal intake. Co-existence of endometriosis and Arias-Stella reaction is very rare. We present a very rare case of endometriotic cyst of the ovary exhibiting Arias –Stella reaction which was seen in of non pregnant patient without any history of hormonal intake.
Oligomenorrhoea, HCG, Hemosiderin laden macrophages
Case Report
A 31-year-old female presented with oligomenorrhoea for the past three months and lower abdominal pain while passing urine for the past three days.
She attained menarche at the age of 13 years. There was no history of hormonal intake and abdominal pain. Her first pregnancy was 8 years back, and it was full term normal delivery. She also gave history of emergency laprotomy and left salpingostomy for left tubal ectopic pregnancy 4 years back. After 11 months, right salphingostomy performed for right tubal ectopic pregnancy.
Per abdomen examination showed vertical scar. Per vaginal examination showed bulky uterus with cystic swelling in the right fornix with mild tenderness and restricted mobility. Per speculum examination showed congested cervix.
Ultrasound revealed right haemorrhagic cyst, left follicular cyst and the endometrial wall thickness of about 4 mm.
Urine pregnancy test was negative. Serum HCG level was 72 ng/ml. Laprotomy was planned. Since the ovaries were adherent to other organs, total abdominal hysterectomy with bilateral oophorectomy was done and the specimens sent for histopathological examination.
Gross Findings
Uterus with cervix measured about 9x6x2.5 cm. Endometrial cavity appeared normal and the wall measured about 0.3 cm. Right ovarian cyst received as collapsed cyst with dark brown inner surface which was measured about 2x1.5x0.5 cm. Left ovarian cyst also collapsed and measured 2x1.5x0.5 cm. No contents were present.
Microscopic Findings
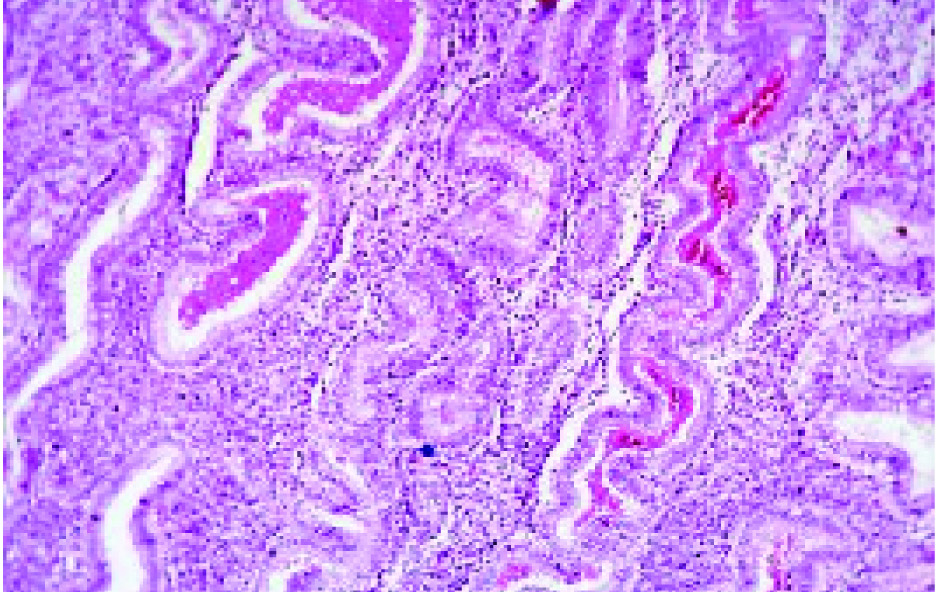
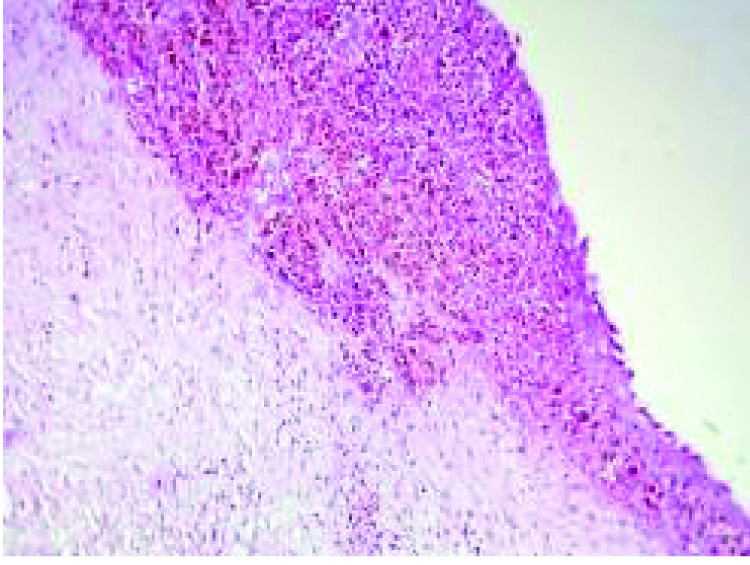
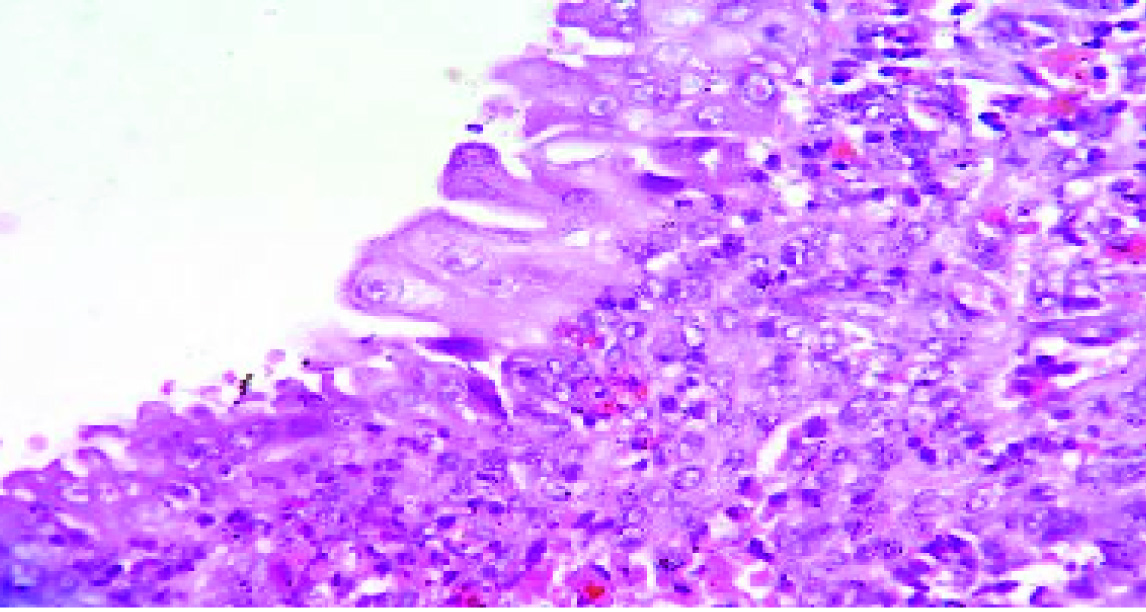
Sections from the uterus showed secretory phase of endometrium [Table/Fig-1] with pre-decidualized stroma. No Arias-stella reaction identified. Both fallopian tube showed normal histology. Sections from right ovary showed cyst wall lined by endometrial glands and stroma and sheets of haemosiderin laden macrophages [Table/Fig-2,3]. The glands exhibited typical Arias-Stella reaction focally with enlarged hyperchromatic irregular nuclei, some of which showed hob-nail pattern [Table/Fig-4,5 and 6]. Sections from the left ovarian cyst showed haemorrhagic corpus luteum.
(H&E, 10X) Endometrium showing tortuous glands with secretory activity.
(H&E, 10X) Cyst wall focally infiltrated by sheets of haemosiderin laden macrophages.
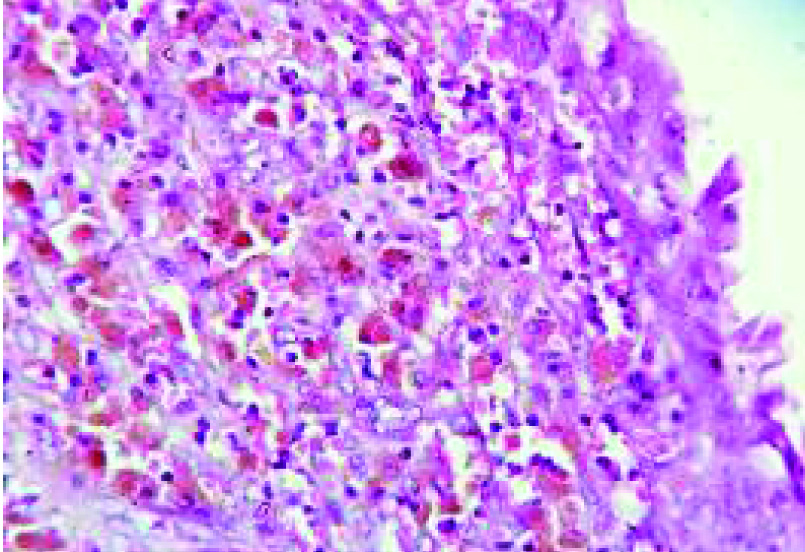
(H&E, 40X) Showing haemosiderin laden macrophages.
(H&E, 4X) Ovarian cyst wall showing foci of endometrial glands & stroma.
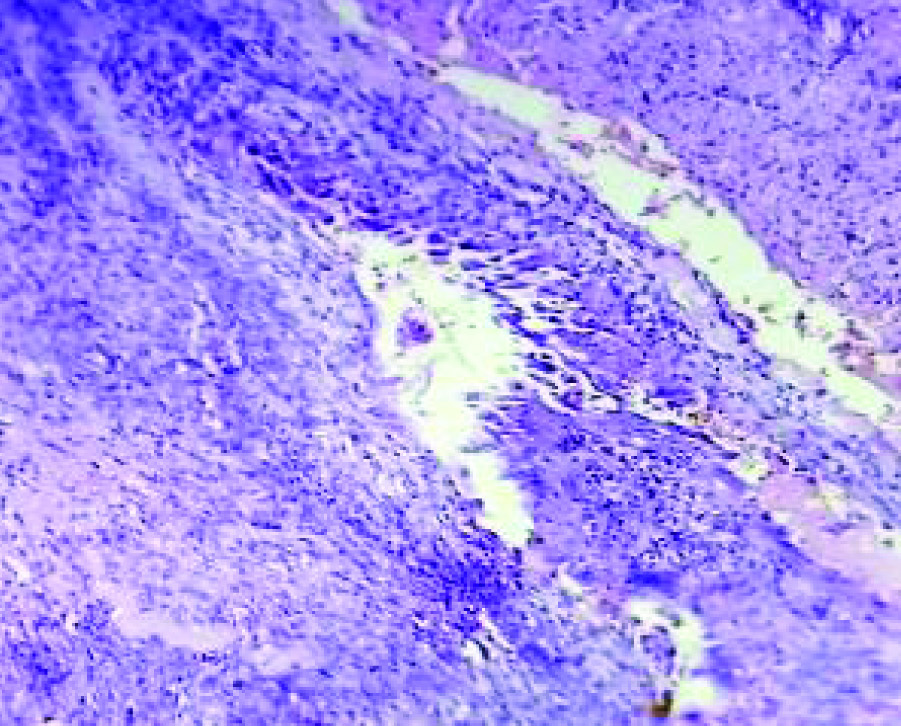
(H&E, 40X) Glands focally showing Arias-Stella reaction. The cells have hyperchromatic nuclei with hobnail pattern.
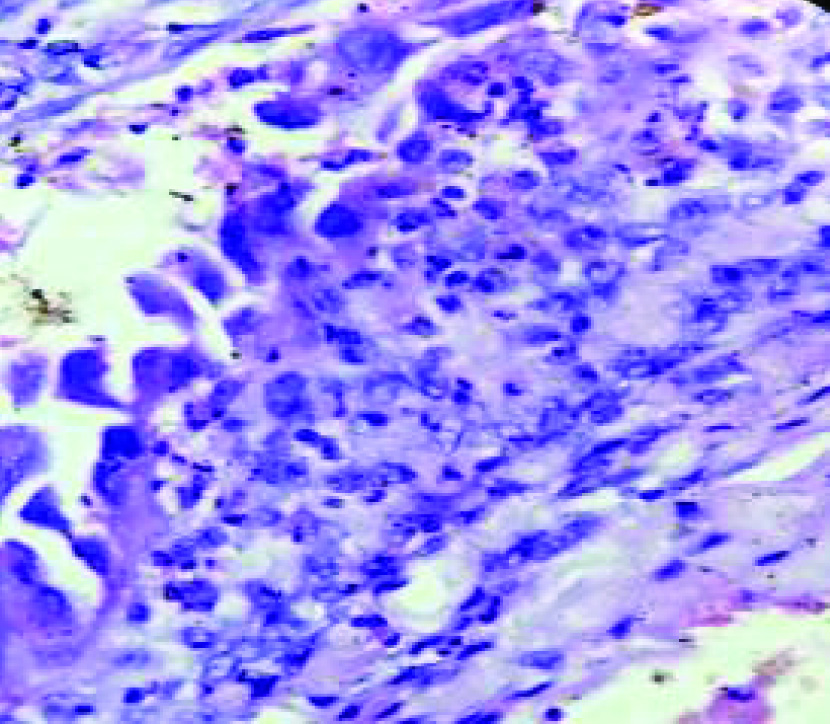
(H&E, 40X) Arias-Stella reaction -The cells have abundant eosinophilic cytoplasm and large nuclei.
Discussion
Endometriosis is defined as presence of endometrial tissue outside the uterus and is closely related to adenomyosis. Common sites involved are ovaries, uterine ligaments, rectovaginal septum, pelvic peritoneum and previous scar. Rarely it may involve the lymphnodes and intestine [1].
Microscopically it is diagnosed by the presence of endometrial epithelial cells, stromal cells and haemosiderin laden macrophages. But it does not always show all three components mentioned previously [2]. Organizing haemorrhage may cause adhesions especially in ovarian chocolate cyst. Our case also showed adhesions since it is a feature of endometriotic cyst.
Usually endometriosis presents as separate lesion, but rarely it may be seen along with ectopic pregnancy. Toki et al., found out a case of ovarian pregnancy with endometriosis showing decidulaized change [3].
Very rarely endometriosis can transform into malignancy. Slavin et al., conducted a study and they found that the primary Mullerian tumours of the bowel arising in foci of endometriosis [4].
Arias-Stella Reaction (ASR) is a common recognized characteristeric feature of gestational endometrium. Hormonally induced histologic changes seen with intrauterine pregnancy, ectopic pregnancy and progesterone therapy [5] and is usually present focally. Commonly seen in cervix, post-abortion curettings, endocervical polyps, adenomyosis [6] endometriosis [7] pregnancies, moles and choriocarcinoma.
Microscopically it is characterized by focal involvement of the glands which are lined by large polyhedral cells with abundant eosinophilic cytoplasm with large hyperchromatic, pleomorphic and smudged nuclei. Usually it has hobnail cells, intraglandular tufts and intranuclear inclusions. Absence of invasion and prominent nucleoli with rare or absent mitotic figures are features of ASR and these are the differentiating features from adenocarcinoma [8].
Association of endometriosis with Arias-Stella reaction is rare. Niels conducted a study and found ASR in endometriosis with co-existent intra-uterine pregnancy. They also observed that regardless of site of the pregnancy, endometrium showed ASR. But in our case, endometrium did not show any ASR and other pregnancy related changes [9].
Presence of Arias-Stella reaction is a histological clue to the presumptive diagnosis of the presence of chorial tissue in cases where the chorionic material is not found in the endometrial biopsy. This finding was identified in a study conducted by Dhingara et al., [10].
Heuttner et al., conducted a study among the non-pregnant females with Arias-Stella reaction and clinicopathological correlation of those cases were done. Most of the patients had a history of hormonal intake especially progesterone. They emphasized the importance of ASR recognition in the samples because overinterpretation of adenocarcinoma will take place in some situations because of cytological atypia [11].
Conclusion
The findings of the present study emphasize that Arias-Stella reaction can occur in the absence of pregnancy or hormonal intake. Though it is very rare finding, we have to look for or rule out pregnancy and history of hormone intake.
[1]. Kumar V, Abbas AK, Aster JC, Robbins and Cotran Pathologic basis of disease 2015 9th editionPhiladelphiaElsevier Saunders [Google Scholar]
[2]. Sakaki M, Hirokawa M, Sano T, Ovarian endometriosis showing decidual change and Arias-Stella reaction with biotin-containing intranuclear inclusionsActa Cytol 2003 47(2):321-24. [Google Scholar]
[3]. Toki T, Obinata M, Nakayama K, Oguchi O, Fujii S, Ovarian pregnancy associated with microscopic decidualized endometriosis of the ovary: report of a caseJ Obstet Gynaecol Res 1998 24(1):45-48. [Google Scholar]
[4]. Slavin RE, Krum R, Van Dinh T, Endometriosis-associated intestinal tumours: a clinical and pathological study of 6 cases with a review of the literatureHum Pathol 2000 31(4):456-63. [Google Scholar]
[5]. Arias-Stella J, The Arias-Stella reaction: facts and fancies four decades afterAdv Anat Pathol 2002 9:12 [Google Scholar]
[6]. Sato H, Nanjo H, Tanaka H, Tanaka T, Arias stella reaction in an adenomatous polyp of the uterusActa Obstet Gynecol Scand 2007 86:106 [Google Scholar]
[7]. Felix A, Nogales FF, Arias-Stella J, Polypoid endometriosis of the uterine cervix with Arias-stella reaction in a patient taking phytoestrogensInt J Gynecol Pathol 2010 29(2):185-88. [Google Scholar]
[8]. Juan Rosai, Rosai and Ackerman’s Surgical Pathology 2011 Tenth editionNewyorkMosby Elsevier [Google Scholar]
[9]. Moller NE, The Arias-stella phenomenon in EndometriosisActa Obstet Gynec Scandinav 1959 38:271 [Google Scholar]
[10]. Dhingra N, Punia RS, Radotra A, Mohan H, Arias-Stella reaction in upper genital tract in pregnant and non-pregnant women: a study of 120 randomly selected casesArch Gynecol Obstet 2007 276(1):47-52. [Google Scholar]
[11]. Huettner PC, Gersell DJ, Arias-Stella reaction in nonpregnant women: a clinicopathologic study of nine casesInt J Gynecol Pathol 1994 13(3):241-47. [Google Scholar]