Variations in Branching Pattern of Renal Artery in Kidney Donors Using CT Angiography
Kumaresan Munnusamy1, Sankaran Ponnusamy Kasirajan2, Karthikeyan Gurusamy3, Gunapriya Raghunath4, Shilpakala Leshappa Bolshetty5, Sudakshina Chakrabarti6, Priyadarshini Annadurai7, Zareena Begum Miyajan8
1 Tutor, Department of Anatomy, Saveetha Medical College and Hospital, India.
2 Associate Professor, Department of Anatomy, Saveetha Medical College and Hospital, India.
3 Assistant Professor, Department of Anatomy, Saveetha Medical College and Hospital, India.
4 Professor, Department of Anatomy, Saveetha Medical College and Hospital, India.
5 Assistant Professor, Department of Anatomy, Saveetha Medical College and Hospital, India.
6 Assistant Professor, Department of Anatomy, Saveetha Medical College and Hospital, India.
7 Tutor, Department of Anatomy, Saveetha Medical College and Hospital, India.
8 Tutor, Department of Anatomy, Saveetha Medical College and Hospital, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sankaran Ponnusamy Kasirajan, 18, Pillaiyar Koil ST, Thirumazhisai, Chennai-600124, India. E-mail : drpks@live.com
Introduction
Each kidney is supplied by a single renal artery originating from abdominal aorta. Since there are lots of renal surgeries happening now-a-days, it becomes mandatory for the surgeons to understand the abnormality and variations in the renal vasculature.
Aim
To study the variations in the branching pattern of renal artery for the presence of early division and accessory renal artery in Indian kidney donors using CT angiography.
Materials and Methods
The CT angiogram images of 100 normal individuals willing for kidney donation were analysed for early divisions and occurrence of accessory renal artery.
Results
A 51% of kidney donors showed variation in the renal artery. Out of 51% variations 38 individuals had accessory renal artery and 13 individuals had early division of renal artery. The distribution of accessory renal artery was equal on both sides (13% on right and left) and 12% of individuals had accessory renal artery on both sides. Out of 13% earlier divisions, 5% was on right side, 7% was on left side and 1% was on both sides.
Conclusion
This study concludes that 51% of kidney donors had renal artery variations. Hence, awareness of variations by evaluating the donors is a must before renal transplantation, urological procedures and angiographic interventions.
Abdominal aorta, Renal artery, Renal transplantation
Introduction
The right and left renal arteries supply approximately 20% of cardiac output to kidney for filtration. Usually renal arteries arise as lateral branch of abdominal aorta just below superior mesenteric artery (L1-L2) and divide into anterior and posterior branch near the hilum. The right renal artery is little longer because abdominal aorta is in left side and lies at a higher level than left renal artery. Around 70% of individuals the kidney is supplied by single renal artery arising from abdominal aorta [1]. However, renal artery variations are very common regarding their origin and number that have been reported by many researchers [2–4]. The renal arteries may vary in their level of origin, caliber, obliquity, number and precise relation. The commonest site of origin of renal arteries from abdominal aorta is lateral (92%), and less commonly on anterolateral (6%) and posterolateral (2%) aspect of abdominal aorta at the level of L1-L2. The frequencies of renal artery variations showed social, ethnic and racial differences [5] for example variations in renal artery and its branching pattern are more common in Africans and less common in Indians [6]. Renal artery variations are divided into two groups as early branching into segmental arteries before reaching hilum and accessory renal artery. Accessory renal artery is more than one main renal artery usually arising from aorta supplying kidney [7]. The anatomy of renal arteries is very important for selecting kidney donors since its impact on renal transplant surgeries [8]. So many studies had been conducted on renal arteries using CT angiography since it allows to obtain precise information on vascular anatomic information on renal arteries and aorta [9]. Variations in the origin, course and branching pattern of the renal artery occur frequently and are of special interest to the urologists, nephrologists, surgeons and radiologists, with respect to the diseases associated with it. Since the accurate knowledge about variations in renal arteries was lacking which is very important for various disciplines to perform better procedures, this study aims to determine the variations in the branching pattern of renal artery for presence of earlier division and accessory renal artery in Indian kidney donors using CT angiography.
Materials and Methods
This prospective study was conducted on 100 kidney donors of age group of 25 – 30 years. The CT angiographic images were collected from a specialized scan center in Chennai during the period of November 2010 – April 2012 for a period of one year and six months. Individuals willing to donate kidney with age group between 25-30 years were included in this study. The collected renal angiographic images of all 100 individuals were analysed for the early divisions into segmental branches and accessory renal artery. If the main renal artery was dividing into segmental branches within 1cm from its origin it was considered as earlier division. Any artery arising directly from aorta to supply kidney apart from renal artery was considered as accessory renal artery. The earlier division (dividing within 1cm) was seen only on main renal artery and the accessory renal artery was counted only for its occurrence.
Results
A 51% of kidney donors showed variation in the renal artery [Table/Fig-1]. Out of 51% variations, 38% had accessory renal artery [Table/Fig-2a] and 13% had earlier division [Table/Fig-3] of renal artery [Table/Fig-4]. The incidence of accessory renal artery was equally distributed on both sides respectively (13% on right and left) [Table/Fig-2b&c]. A 12% of individuals showed accessory renal artery on both sides [Table/Fig-5], 5% of individuals had earlier division on right side [Table/Fig-3a] and 7% individuals had earlier division on left side [Table/Fig-3b]. Only 1% individual had earlier division on both sides [Table/Fig-3c&6].
Number of kidney donors showing variations.
| S.No | Normal & variationsof renal artery | Number of donors |
|---|
| 1. | Normal | 49 |
| 2. | Variations | 51 |
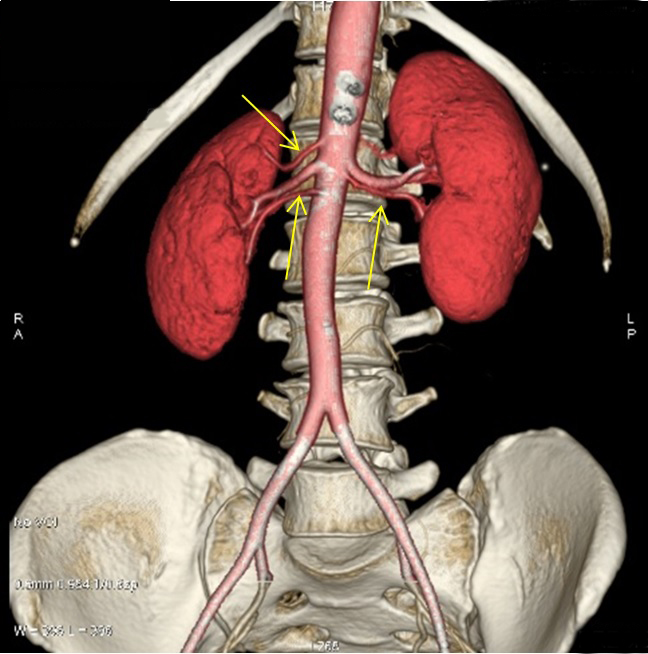
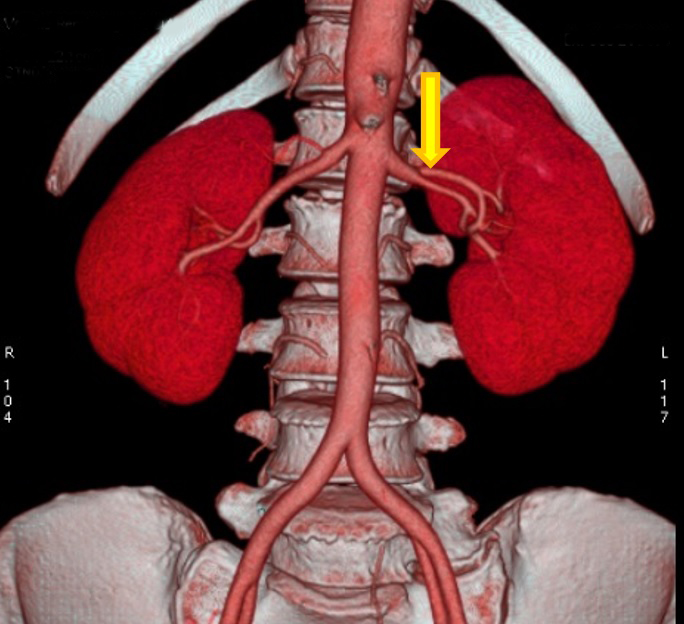
Yellow arrows showing accessory renal artery (triple renal artery). Two accessory renal arteries on right side (triple renal arteries) and one accessory renal artery on left side (double renal arteries).
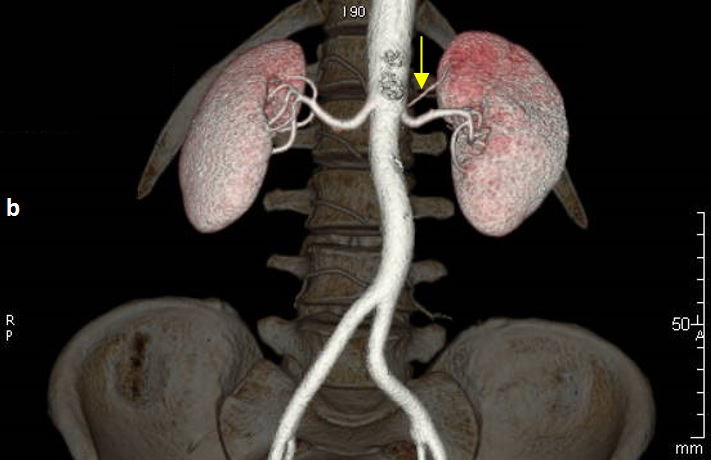
Yellow arrow showing accessory renal artery on left side (double renal arteries).
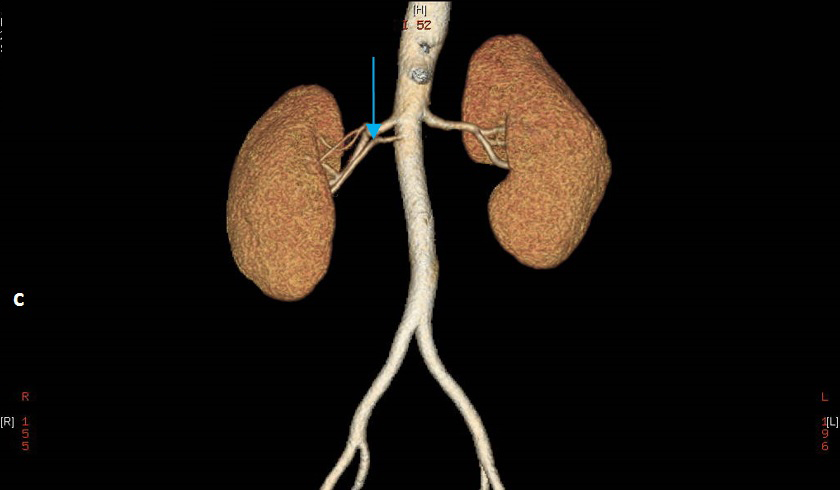
Blue arrow showing accessory renal artery on right side (right double renal arteries).
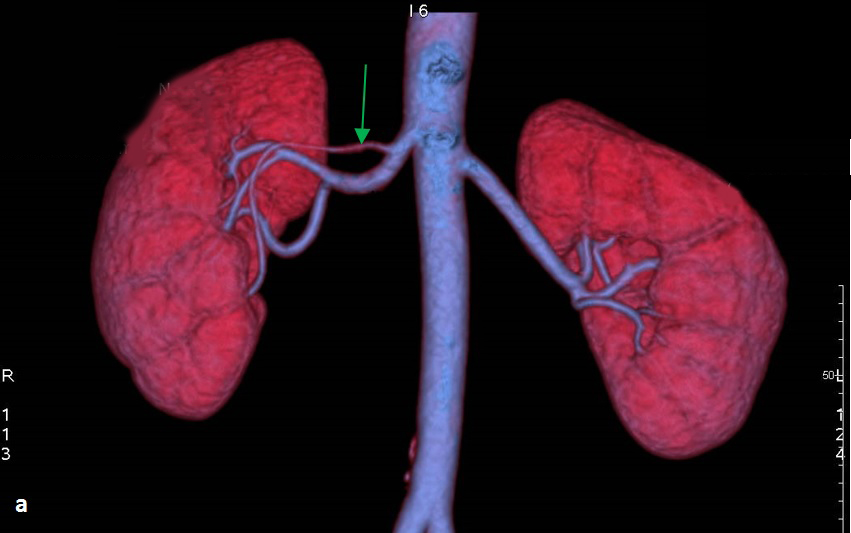
Green arrow showing earlier division on right side into segmental arteries.
YBlock yellow arrow showing earlier division of renal artery into segmental arteries on left side.
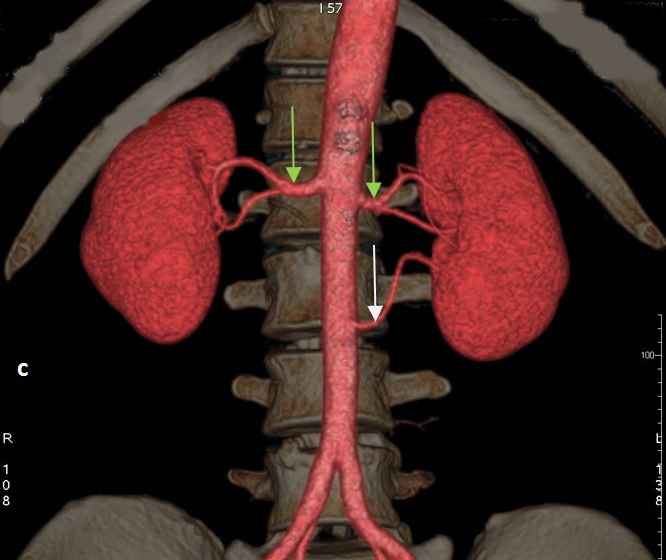
Green arrows showing earlier division of renal artery on both sides and white arrow showing accessory renal artery on left side.
Number of variations in renal artery.
| S.No | Variations of renal artery | Number of individuals |
|---|
| 1. | Accessory renal artery | 38 |
| 2. | Earlier division of renal artery | 13 |
Distribution of accessory renal artery.
| S.No | Accessory renal artery on right side 13% | Accessory renal artery on left side 13% | Accessory renal artery on both sides 12% |
|---|
| 1. | Single accessory renal artery (10%) (double renal artery) | Single accessory renal artery (11%) (double renal artery) | Single accessory renal artery (11%) (double renal artery) |
| 2. | Double accessory renal artery (3%) (triple renal artery) | Double accessory renal artery (2%) (triple renal artery) | Double accessory renal artery (1%) (triple renal artery) |
Distribution of earlier divisions of renal artery.
| S.No | Earlier division of renal artery | Number of individuals |
|---|
| 1. | Right | 5 |
| 2. | Left | 7 |
| 3. | Both | 1 |
Discussion
Accessory Renal Artery: In the current study the normal renal arterial pattern was found only in 49% whereas 51% of renal artery showed variations. Similar study on accessory renal artery and earlier division of renal artery were conducted by Gumus et al., [7]. They reported earlier division in 27% and accessory renal artery in 27%. In this current study earlier division was seen in 12% and accessory renal artery was seen in 38% of individuals. This increased incidence of accessory renal arteries in this study as compared to previous studies may be due to regional difference in individuals as this study was conducted on Chennai population. Similar study on arterial pattern was also done by Sathyapal et al., [4], where they analysed 130 renal angiograms on donors. They found 23.2% of first (single accessory renal artery) and second (double accessory renal artery) additional arteries on both sides, and the frequency of such incidence was more on left side 32% than right side 23.3% and on both sides it was 10.2%, for first additional arteries only. In this current study the accessory renal arteries were found in 38 individuals (38%), out of 38% variations, 13% were on the right side and 13% were on the left side. Accessory renal artery on both right and left side was present in 12% individuals. Ragiba et al., analysed angiographic images of 150 individuals with 42% of multiple renal arteries which correlates with this current study [10]. The incidence of accessory renal arteries are equal on both sides also there was not much significant difference in its bilateral incidence.
The presence of multiple renal artery did not have significant association in complications like intraoperative blood loss in donor, one year graft survival and creatinine clearance [11] in recipients provided the appropriate anatomy of multiple renal arteries are known to the surgeons operating in that area.
Embyological Basis: The origin of renal arteries and its variations can be explained by the development of mesonephric arteries. These mesonephric arteries supply the kidneys, suprarenal glands and gonads on both sides of the aorta, from sixth cervical vertebra to third lumbar vertebra, a region known as rete arteriosum urogenitale. As the development progresses these arteries degenerate, leaving one prominent mesonephric artery. Deficiency in the development of mesonephric arteries results in more than one renal artery [12]. The existence of one or multiple accessory renal artery is due to the non-obliteration of mesonephric arteries [13]. Also, the multiple renal arteries can be explained that during ascent of kidney, it receives blood supply from its adjacent arteries like common iliac and aorta. Persistence of those arteries may result in multiple renal arteries [14]. Such subjects with accessory renal arteries are not ideal candidates for transplantation.
Earlier Divisionof Renal Artery: The earlier division of renal artery was observed in 13% of individuals. Right side early division was found in 5 individuals (5%), left side early division was seen in 7 individuals (7%) and on both side early division was found in one individual (1%). Similar study was done to show early division of renal artery into segmental arteries which was seen in 8% of individuals [15].
The earlier division could have been due to delay in communication between the factors present in mesenchyme of the blood vessel and the factors present in the mesenchyme of metanephros like glial derived neurotropic factor and hepatocytic growth factor [16]. The 13% of earlier division of renal artery population is not a suitable candidate for transplantation. Since the surgeon would not have a long pedicle for anastomosis of renal artery [17].
Henceforth the study on anatomical variations in vascularization of kidney is very important to transplant surgeons involving in donor nephrectomies [18]. With these knowledge the surgeon can explore and treat renal trauma, renal transplantation, renal vascular embolization, angioplasty and radical renal surgeries [19]
Conclusion
This study concludes that 51% of population have variations in the pattern of renal arteries. The incidence of accessory renal artery is more common than early divisions, also the incidence of accessory renal artery showed equal distribution in right, left and both sides.
[1]. Susan standring. Gray’s Anatomy 2008 40Churchill Livingstone:1183 [Google Scholar]
[2]. Shakeri AB, Tubbs RS, Shoja MM, Pezeshk P, Farahani RM, Khaki AA, Bipolar supernumerary renal arterySurg Radiol Anat 2007 29(1):89-92. [Google Scholar]
[3]. Rao M, Bhat SM, Venkataramana V, Deepthinath R, Bolla SR, Bilateral prehilar multiple branching of renal arteries: a case report and literature reviewKathmandu University Medical Journal (KUMJ) 2006 4(3):345-48. [Google Scholar]
[4]. Satyapal KS, Haffejee AA, Singh B, Ramsaroop L, Robbs JV, Kalideen JM, Additional renal arteries incidence and morphometrySurg Radiol Anat 2001 23(1):33-38. [Google Scholar]
[5]. Kadir S, Kidneys. In: Kadir S, edAtlas ofnormal and variant angiographic anatomy 1991 PhiladelphiaW.B. Saunders Company:387-429. [Google Scholar]
[6]. Boijsen E, Renal angiography: Techniquesand hazards; anatomic and physiologicconsiderations. In: Baum S, edAbrams’ angiography 1997 4th edPhiladelphiaLittle, Brown and Company:1101-1131. [Google Scholar]
[7]. Gumus H, Brdal Ozdemir E, Cetincakmak ML, Tekbas G, Ekici Onder H, Variations of renal artery in 820 patients using 64-detector CT-AngiographyRenal Faliure 2012 34:286-90. [Google Scholar]
[8]. Turba UC, Uflacker R, Bozlar U, Hagspiel KD, Normal renal arterial anatomy assessed by multidetector CT angiography: are there differences between men and women?Clin Anat 2009 22(2):236-42. [Google Scholar]
[9]. Thatipelli MR, Sabater EA, Bjarnason H, McKusick MA, Misra S, CT angiography of renal artery anatomy for evaluating embolic protection devicesJ Vasc Interv Radiol 2007 18(7):842-46. [Google Scholar]
[10]. Zaoyapan R, Pelin C, Ayla K, A retrospective study on multiple renal arteries in Turkish populationInternational journal of experimental and clinical anatomy 2009 (3):35-39. [Google Scholar]
[11]. Hsu TH, Su Li, Ratner LE, Trock BJ, Kavoussi LR, Impact of renal artery multiplicity on outcomes of renal donors and recipients in laparoscopic donor nephrectomyUrology 2003 61(2):323-27. [Google Scholar]
[12]. Felix W, The development of the urogenital organs. In: Keibel F, Mall FP, editorsManual of Human Embryology 1912 PhiladelphiaJ.B. Lippincott Company:752-880. [Google Scholar]
[13]. Praveen KG, Bilateral Superior Accessory Renal Arteries – It’s embryological basis & Surgical Importance A – case reportJournal clinic case reports 2011 2(1):100-03. [Google Scholar]
[14]. Keibel F, Mall FP, Manual of human embryology 1912 2PhiladelphiaJ.B. Lippincott:820-25. [Google Scholar]
[15]. Ozkan U, Oguzkurt L, Tercan F, Kizilkilic O, Koc Z, Koca N, Renal artery origins and variations: angiographic evaluation of 855 consecutive patientsDiagn Interv Radiol 2006 12:183-86. [Google Scholar]
[16]. Ferrara N, Role of vascular endothelial growth factor in the regulation of angiogenesisKidney Int 1999 56:794-814. [Google Scholar]
[17]. Weld KJ, Bhayani SB, Belani J, Ames CD, Hruby G, Landman J, Extrarenal vascular anatomy of kidney: assessment of variations and their relevance to partial nephrectomyUrology 2005 66(5):985-89. [Google Scholar]
[18]. Flechner SM, Sandler CM, Houston GK, Van Buren CT, Lorber MI, Karan BD, 100 living related kidney donor evaluations using digital subtraction angiographyTransplantation 1985 40:675-78. [Google Scholar]
[19]. Fox M, Yalin R, Renal transplantation with multiple arteriesBr J Urol 1979 51:333-36. [Google Scholar]